重症监护病房急性呼吸窘迫综合征患者不良预后的危险因素分析
2021-11-30邓鸿胜怀佳萍陈科强
邓鸿胜 怀佳萍 陈科强

[关键词] 重症监护病房; 急性呼吸窘迫综合征;感染性休克;危险因素
[中图分类号] R563.8 [文献标识码] B [文章编号] 1673-9701(2021)18-0087-04
Risk factors of poor prognosis in patients with acute respiratory distress syndrome in intensive care unit
DENG Hongsheng1 HUAI Jiaping1 CHEN Keqiang2
1. Department of Critical Care Medicine,Jinhua Municipal Central Hospital in Zhejiang Province,Jinhua 321000,China;2. Department of Laboratory Medicine,Jinhua Municipal Central Hospital in Zhejiang Province,Jinhua 321000,China
[Abstract] Objective To explore the risk factors of death in patients with acute respiratory distress syndrome (ARDS) in intensive care unit (ICU). Methods A retrospective analysis method was used to collect the clinical data of 108 patients with acute respiratory distress syndrome(ARDS) admitted to our hospital from January 2012 to October 2013. They were divided into the 28-day survival group with 65 patients and the death group with 43 patients. The general information was recorded in detail,including gender,age,transfer location,vasoactive medicine,course of illness when entering the ICU, oxygenation index (PaO2/FiO2), Glasgow score,ICU stay,patient category and related laboratory indicators [Total bilirubin (TBIL), Creatinine (Cr), Platelet (Plt)]. Univariate and multivariate analyses were conducted to investigate the risk factors of death. Results Multivariate Logistic regression analysis showed that age ≥65 years,ARDS combined with shock,and platelets <100×109/L were risk factors for 28-day death in ARDS patients (OR>1, P<0.05). Conclusion Elder age,ARDS combined with shock and thrombocytopenia are risk factors for 28-day death in ARDS patients. It should be identified early in clinical practice and intervened using effective measures.
[Key words] Intensive care unit; Acute respiratory distress syndrome; Septic shock; Risk factors
急性呼吸窘迫综合征(Acute respiratory distress syndrome,ARDS)最初定义于1967年,1篇病例报告描述了危重成人和儿童急性低氧血症、非心源性肺水肿、肺顺应性降低的临床表现,与创伤、肺炎、败血症和误吸等多种临床疾病相关的呼吸功增加及呼吸机正压机械通气需求增加。ARDS最常见于肺炎(细菌性和病毒性,真菌性较少见)、非肺源性脓毒症(来源包括扁桃体周围、泌尿道、软组织和皮肤)、胃和(或)口腔和食道内容物吸入和严重创伤(如钝挫伤或外伤穿透伤或烧伤[1])。ARDS患者的长期预后越来越被认为是重要的研究目标,在全世界重症监护病房中约有10%的患者出现ARDS。尽管有所改善,但在大多数研究中,死亡率仍高达30%~40%[2]。本研究收集我院108例合并或不合并感染性休克患者的临床资料,旨在研究影响ARDS患者预后的可能危險因素,促进早期认识、早期干预ARDS,现报道如下。
1 资料与方法
1.1 一般资料
回顾性分析2012年1月至2013年10月在我院收治的108例ARDS患者的临床资料,分为28 d存活组65例和死亡组43例。28 d存活组男46例,女19例;年龄18~86岁,平均(59.1±16.3)岁;重症监护病房(Intensive care unit,ICU)住院时间2~42 d,平均(14.3±11.5)d。死亡组男31例,女12例;年龄18~89岁,平均(67.3±17.3)岁;ICU住院时间2~28 d,平均(8.5±6.3)d。疾病类型:ARDS不伴感染性休克57例,ARDS伴感染性休克51例。两组患者一般资料(性别、年龄及ICU住院时间)比较,差异无统计学意义(P>0.05),具有可比性。见表1。
1.2 纳入标准及排除标准
1.2.1 纳入标准[3] ①符合2019年柏林关于ARDS的診断标准和《2019中国感染性休克指南》,在进入ICU后24 h内符合ARDS或合并有感染性休克临床标准的成人患者(至少18岁);②患者或其家属同意翻阅其病历资料;③临床资料完整者。
1.2.2 排除标准[4] ①18岁以下;②经历失血性休克;③濒死状态;④患者或其家属不同意翻阅其病历资料。由于所有数据均是从实验室检测信息系统中回顾性检索,没有额外的血样或实验室分析,因此没有获得患者的知情同意。该研究已获得金华市中心医院医学伦理委员会批准。
1.3 方法
1.3.1 一般情况 设计一般资料调查表,仔细阅览患者病历资料,详细记录其一般情况,包括性别、年龄、转入地(急诊室、手术室、普通病房)、血管活性药物、入ICU时病程、氧合指数氧分压比吸入氧浓度(PaO2/FiO2)、格拉斯哥评分(Glasgow coma score,GCS)[5]、ICU住院时间、患者类别(ARDS患者是否合并感染性休克):ARDS定义为PaO2/FIO2急性下降至200 mmHg或更低,无论呼气末正压水平如何;双侧肺浸润或胸片符合水肿;无左房高压的临床证据;需要正压通气[3]。休克的定义[6]:①心率至少90次/min;②呼吸频率至少为20次/min或二氧化碳分压为32 mmHg或更低,或使用机械通气;③在液体复苏、低剂量多巴胺[≤5 μg/(kg·min)]或多巴酚丁胺的情况下,使用血管升压药维持至少90 mmHg的收缩压;④三种低灌注迹象中至少有一种(每小时尿量<0.5 mL/kg体重,持续1 h或更长时间;神经功能障碍定义为精神错乱、精神病或格拉斯哥昏迷评分≤6分;血浆乳酸高于正常值的上限)。
1.3.2主要生化指标 包括脂代谢指标[总胆红素(Total bilirubin,TBIL)、肌酐(Creatinine,Cr)、血小板(Platelet,Plt)],使用美国贝克曼公司生产的自动生化分析仪和希森美康公司生产的血常规分析仪,试剂盒均为仪器配套,分别为贝克曼库尔特实验系统(苏州)有限公司和希森美康医用电子(上海)有限公司,操作严格按照试剂盒说明书执行。
1.4 统计学方法
采用 SPSS 26.0 统计学软件进行数据处理,计数资料以[n(%)]表示,采用χ2检验,采用多因素Logistic回归计算ARDS患者死亡风险的OR值及对应的95%CI,P<0.05为差异有统计学意义。
2 结果
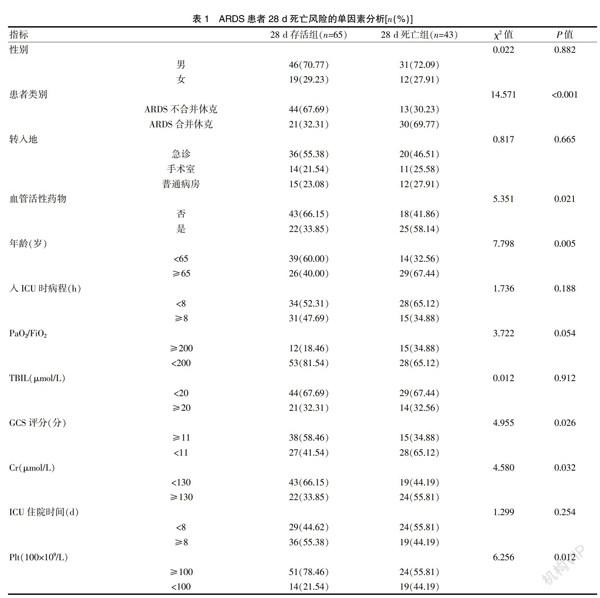
2.1 ARDS患者28 d死亡风险的单因素分析
两组患者性别、转入地、入ICU时病程≥8 h、PaO2/FiO2<200、TBIL≥20 μmol/L和ICU住院时间≥8 d比较,差异无统计学意义(P>0.05),而两组患者类别、血管活性药物、年龄≥65岁、GCS评分<11分、Cr≥130 μmol/L、Plt<100×109/L比较,差异有统计学意义(P<0.05)。见表 1。
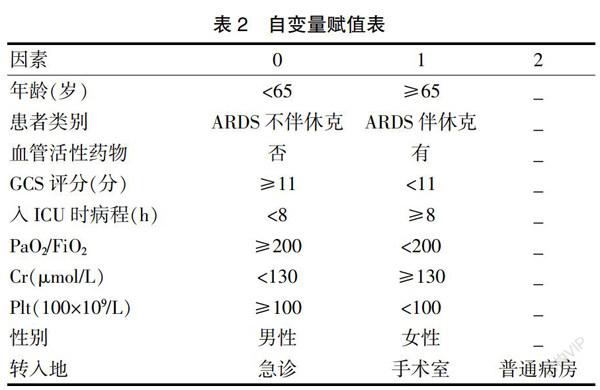
2.2 ARDS患者28 d死亡的危险因素分析
自变量赋值表见表2。经多因素Logistic回归分析显示,年龄≥65岁、ARDS合并休克以及Plt<100×109/L是ARDS患者28 d死亡的危险因素(OR=3.186、2.050和2.904,P<0.05)。见表3。
3讨论
ARDS定义为非心源性肺水肿、低氧血症的急性发作和机械通气的需要。在全球范围内,ARDS占重症监护病房住院人数的10%,每年有300多万ARDS患者,死亡率仍高达30%~40%,治疗的重点是肺保护性通气,目前还没有明确的药物治疗方法。因此研究ARDS不良预后的相关危险因素,及早干预可减少ARDS患者的死亡率[7-9]。
本研究结果显示,经多因素Logistic回归分析证实,年龄≥65岁、ARDS合并休克以及Plt<100×109/L是ARDS患者28 d死亡的危险因素,提示ARDS患者不良预后与年龄≥65岁、ARDS合并休克以及Plt<100×109/L有关。分析其原因主要为以下几点:①年龄。根据国外的研究报告显示,急性肺损伤的风险和死亡率随着年龄的增长而增加,不同的年龄阶段ARDS的发病情况也不相同,对于年龄≥65岁患者,随着年龄的增大,患者的预后也变差。ARDS老年患者对各种急性应激因素,如炎症反应或创伤打击等抵御能力,相比年轻患者而言更弱,更容易引起各脏器器官功能的紊乱,同时储备能力也普遍下降。而且高龄患者对治疗的敏感性降低,机械通气所造成的肺损伤也更明显,最终导致不良的预后[10-12]。②ARDS合并休克。据国外资料报道,脓毒症相关的ARDS死亡率最高[8,13-14];当ARDS继发于其他原因时,如胃误吸、多发性创伤或脂肪栓塞,死亡率则较低。ARDS在菌血症或败血症患者中很常见,各种研究报告的发病率为18%~38%。ARDS是脓毒症的并发症,从轻微的肺功能不全到严重威胁生命安全[9,15-18]。脓毒症诱导的ARDS主要参与粒细胞的活化,在随后的过程中,可能会在几个正反馈系统中放大彼此的影响。在最后阶段可能产生氧自由基[19],导致不良预后。③Plt<100×109/L。血小板是止血的重要细胞效应物,作为病理性血栓形成的循环效应物参与疾病。近十年来的研究表明,血小板及其前体巨核细胞在肺组织中具有独特的相互作用,提示血小板是实验性急性肺损伤和临床急性呼吸窘迫综合征的重要效应因子[20-21]。血小板对肺和全身内皮通透性和血管屏障完整性有复杂的影响,肺泡-毛细血管膜通透性增加伴富含蛋白质的肺水肿液渗漏是ARDS病理生理学的一个中心特征。与肺泡内和间质水肿一样,肺泡出血和红细胞间质积聚是急性肺损伤(ALI)早期的主要特征,其病理相关性为弥漫性肺泡损伤。实验模型表明,血小板减少导致皮肤、大脑和肺部在急性炎症条件下发生非创伤性出血,并与经典的血小板止血活性无关。严重血小板减少与自发性肺泡出血有关。血小板数量在危重疾病中改变,影响ARDS的预后,血小板减少症在有ARDS风险或伴有ARDS的危重患者中很常见,并与包括死亡在内的负性结局相关[22-23]。
綜上所述,高龄、ARDS合并休克以及血小板减少是ARDS患者28 d死亡的危险因素,临床上应早期识别并积极采取有效措施进行干预。
[参考文献]
[1] Bellani G,Laffey JG,Pham T,et al. Epidemiology,patterns of care,and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries[J]. Jama,2016,315(8):788-800.
[2] Shao S,Kang H,Tong Z. Early neuromuscular blocking agents for adults with acute respiratory distress syndrome:A systematic review,meta-analysis and meta-regression[J]. BMJ Open,2020,10(11):e037 737-e037 753.
[3] Ranieri VM,Rubenfeld GD,Thompsonb T,et al. Acute respiratory distress syndrome:The Berlin Definition[J]. Jama,2012,307(23):2526-2533.
[4] Dellinger RP,Levy MM,Carlet JM,et al. Surviving sepsis campaign:International guidelines for management of severe sepsis and septic shock:2008[J]. Intensive Care Med,2008,34(1):17-60.
[5] Orso D,Vetrugno L,Federici N,et al. Endotracheal intubation to reduce aspiration events in acutely comatose patients:A systematic review [J]. Scand J Trauma Resusc Emerg Med,2020,28(1):116-126.
[6] Cecconi M,De Backer D,Antonelli M,et al. Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine[J].Intensive Care Med,2014,40(12):1795-1815.
[7] Rubenfeld GD,Caldwell E,Peabody E,et al. Incidence and outcomes of acute lung injury[J]. N Engl J Med,2005, 353(16):1685-1693.
[8] Sharma S,Kumar A. Septic shock,multiple organ failure,and acute respiratory distress syndrome[J]. Curr Opin Pulm Med,2003,9(3):199-209.
[9] Wang H,Das S,Wieruszewski PM,et al. Unexpected BP sensitivity to angiotensin Ⅱ in a patient with coronavirus disease 2019,ARDS,and septic shock[J]. Chest,2020, 158(2):e55-e58.
[10] Zilberberg MD,Epstein SK. Acute lung injury in the medical ICU:Comorbid conditions,age,etiology,and hospital outcome [J]. Am J Respir Crit Care Med,1998,157(4 Pt 1):1159-1164.
[11] Walmrath D,Grimminger F,Pappert D,et al. Bronchoscopic administration of bovine natural surfactant in ARDS and septic shock:Impact on gas exchange and haemodynamics [J]. Eur Respir J,2002,19(5):805-810.
[12] Shiloh AL,Kazzi MG,Mathew R,et al. A man in his 40s with a history of hypertension and alcohol dependency presenting to the ED with respiratory distress[J]. Chest,2014,145(2):e3-e6.
[13] Thong MK. Dengue shock syndrome and acute respiratory distress syndrome[J]. Lancet,1998,352(9141):1712.
[14] Stahl K,Schenk H,Seeliger B,et al. Extracorporeal membrane oxygenation for acute respiratory distress syndrome due to pneumocystis pneumonia[J]. Eur Respir J,2019,54(3):1900 410-1900 418.
[15] Carcillo JA,Davis AL,Zaritsky A. Role of early fluid resuscitation in pediatric septic shock[J]. Jama,1991,266(9):1242-1245.
[16] Dumler JS,Bakken JS. Human ehrlichioses:Newly recognized infections transmitted by ticks[J]. Annu Rev Med,1998,49(1):49 201-49 213.
[17] Evans NA,Walker JM,Manchester AC,et al. Acute respiratory distress syndrome and septic shock in a cat with disseminated toxoplasmosis[J]. J Vet Emerg Crit Care(San Antonio),2017,27(4):472-478.
[18] Wan L,Liao G,Wan X,et al. The incidences of organ dysfunction in the early resuscitation of severe sepsis and septic shock patients:A retrospective analysis[J]. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue,2016,28(5):418-422.
[19] Günther A,Schmidt R,Harodt J,et al. Bronchoscopic administration of bovine natural surfactant in ARDS and septic shock:Impact on biophysical and biochemical surfactant properties [J]. Eur Respir J,2002,19(5):797-804.
[20] Leturcq DJ,Moriarty AM,Talbott G,et al. Antibodies against CD14 protect primates from endotoxin-induced shock [J]. J Clin Invest,1996,98(7):1533-1538.
[21] Takei Y,Yamada M,Saito K,et al. Increase in circulating ACE-positive endothelial microparticles during acute lung injury[J]. Eur Respir J,2019,54(4):1801 188-1801 265.
[22] Disilvio B,Young M,Gordon A,et al. Complications and outcomes of acute respiratory distress syndrome[J]. Crit Care Nurs Q,2019,42(4):349-361.
[23] Ichikawa D,Jwa SC,Seto T,et al. Successful treatment of severe acute respiratory distress syndrome due to Group A streptococcus induced toxic shock syndrome in the third trimester of pregnancy-effectiveness of venoarterial extracorporeal membrane oxygenation:A case report[J]. J Obstet Gynaecol Res,2020,46(1):167-172.
(收稿日期:2021-02-03)
