轻或重症手足口病患儿HEV71分离鉴定及其VP1基因型分析
2016-07-29蒋卓婧何婷婷陈金堃
蒋卓婧,何婷婷,陈金堃,严 杰
轻或重症手足口病患儿HEV71分离鉴定及其VP1基因型分析
蒋卓婧1,2,何婷婷2,陈金堃2,严杰1
1. 浙江大学医学院病原生物学系,杭州310058;2. 浙江省绍兴市疾病预防控制中心,绍兴312071
摘要:目的从不同病情手足口病(HFMD)患儿中分离鉴定人肠道病毒71型(HEV71)并分析其VP1基因型及药物结合位点突变情况。方法从2014年浙江省绍兴地区轻、重症各4例HFMD患儿标本中分离HEV71并用RT-PCR进行鉴定。采用RT-PCR扩增病毒分离株全长VP1基因并测序。采用专业生物信息学软件,对HEV71分离株进行VP1基因分型、确定VP1基因中药物结合位点突变情况及构建HEV71分离株系统进化树。结果8例HFMD患儿标本中均分离出HEV71。HEV71分离株与文献报道的VP1-C4a基因亚型的核苷酸和氨基酸序列相似性分别高达97.2%~98.8%和99.3%~99.7%。2例重症患儿HEV71分离株分别在VP1基因序列第179位药物结合位点发生V179L点突变。5株HEV71与安徽和湖南分离株、3株与上海和山东分离株亲缘关系较近。结论本地区不同病情HFMD患儿分离的HEV71均为VP1-C4a基因亚型,重症患儿HEV71分离株VP1基因第179位药物结合位点突变可能与病情严重程度有关。
关键词:手足口病;人肠道病毒71型;VP1基因;基因分型;药物结合位点/突变
人肠道病毒71型(humanenterovirus71,HEV71)为肠道病毒A组单股正链RNA病毒,是手足口病(hand-foot-and-mouthdisease,HFMD)主要病原体[1-3]。HEV71壳粒由VP1~VP4 4种病毒蛋白组成,其中VP1具有细胞受体结合位点、中和抗体表位及抗病毒药物结合位点,故在病毒吸附、穿入、脱壳等感染过程以及抗病毒免疫应答、药物治疗效果等方面发挥重要作用[4-6]。近年文献报道,若VP1功能相关重要位点发生突变,可使HEV71毒力和耐药性发生改变,从而对HFMD患者病情严重程度产生明显影响[7-9]。业已发现,HEV71的VP1序列中有一个微小RNA病毒衣壳蛋白样功能结构域(picornavirus capsid protein domain-like,rhv_like),该结构域含有9个药物结合位点[10-12]。此外,根据VP1序列差异可将HEV71分为A、B0~5和C1~5基因型,不同地区流行的优势VP1基因型明显不同[13-15]。本研究中,我们从当地轻症或重症HFMD患儿标本中分离并鉴定了HEV71株,继而测定并分析了HEV71分离株的VP1基因序列,以期了解本地区优势流行的HEV71基因型以及VP1药物结合位点突变与患儿病情严重程度之间的关系。
1材料与方法
1.1病例来源、诊断及分类2014年绍兴地区未经治疗的HFMD初诊患者。参照我国卫生部2013年版《手足口病诊疗指南》[16],根据患儿临床表现及实时荧光RT-PCR检测结果等进行疾病诊断。轻症病例判断标准:手、足、口、臀部皮疹可伴发热;重症病例判断标准:有神经系统受累临床表现或出现下列情况之一者:1)频繁抽搐、昏迷、脑疝;2)呼吸困难、紫绀、血性泡沫痰、肺部罗音等;3)休克等循环功能不全表现。4例轻症或4例重症HFMD患儿中,均为男性3例、女性1例,年龄1~3岁,前者编号为SXQ1~4,后者编号为SXZ1~4[16]。
1.2RT-PCR根据我国卫生部2013年版《手足口病诊疗指南》[16],采集上述HFMD患儿鼻咽拭子、肛拭子和/或疱疹液标本。根据High Pure Viral Nucleic Acid Kit(Roche)说明书,提取上述标本中的总RNA。根据One Step PrimerScript RT-PCR Kit(TaKaRa)说明书,以总RNA为模板,先逆转录生成cDNA,然后分别用人肠道病毒(HEV)和HEV71引物及其探针,对逆转录产物进行扩增及检测。反应总体积25 μL,反应程序:42 ℃ 30 min,95 ℃ 2 min;95 ℃ 5 s、55 ℃ 35 s,40个循环,被检样本Ct值≤35.0判为阳性。HEV 5′-非编码区通用PCR引物和探针序列:上游引物5′-CTG YRG CGG AAC CGA CTA C-3′(Y=C或T,R=G或A),下游引物5′-ATT GTC ACC ATA AGC AGC CA-3′,探针5′-FAM-TTG GGT GTC CGT GTT T-MGB-3′[17]。HEV71-VP1基因PCR引物和探针序列:上游引物5′-TGA TTG AGA CAC GST GTG TYC TTA-3′(S=G或C),下游引物5′-CCC GCT CTG CTG AAG AAA CT-3′,探针5′-FAM-TCG CAC AGC ACA GCT GAG ACC ACT C-MGB-3′[18]。
1.3病毒分离与鉴定根据我国卫生部2012年版《手足口病预防控制指南》[19],采集上述8例HFMD患儿鼻咽拭子、肛拭子和/或疱疹液标本置于保存液(MEM 80.5 mL,3%L-谷氨酰胺1.0 mL,胎牛血清5 mL,7.5%NaHCO3溶液3.5 mL,10 000 U/mL青霉素和链霉素各10 mL)中。非洲绿猴肾细胞(Vero)株由浙江省疾病预防控制中心提供,采用含10%小牛血清、100 U/mL青霉素、100 μg/mL链霉素的MEM培养液(Gibco)培养。Vero细胞接种于6孔细胞培养板中,37 ℃、5%CO2条件下预培养24 h,使之形成单层细胞,然后接种病毒保存液,继续培养5 d,每天用倒置光学显微镜观察,若出现细胞病变(cytopathic effect,CPE)者判为HEV71阳性,CPE阴性培养物盲传两代仍未出现CPE者判为阴性。按上法提取CPE阳性培养物总RNA并用RT-PCR检测其病毒及其类型[17-19]。1.4全长HEV71-VP1基因扩增按上法提取8例HFMD患儿HEV71分离株总RNA。根据Titan One Tube RT-PCR试剂盒(Roche)说明书,先以Oligo-dT为引物进行逆转录,然后以逆转录产物为模板,扩增全长HEV71-VP1基因的DNA片段。上游引物:5′-GCA GCC CAA AAG AAC TTC AC-3′;下游引物:5′-AAG TCG CCA GAG CTG TCT TC-3′[14]。反应总体积50 μL,反应程序:95 ℃ 3 min;95 ℃ 15 s、58 ℃ 15 s、72 ℃ 1.5 min,30个循环;72 ℃ 10 min。扩增产物委托杭州华大基因公司测序。
1.5HEV71-VP1基因序列分析参照GenBank中HEV71参考标准株VP1基因A、B0~5、C1~5基因型序列,根据HEV71分离株全长VP1基因测序结果,采用Mega5.2软件确定其VP1基因型并构建系统进化树。采用病毒蛋白结构分析软件(http://www.ncbi.nlm.nih.gov/Structure/cdd/wrpsb.cgi),确定HEV71-VP1中药物结合位点及HEV71分离株VP1基因序列中相关位点突变情况。
2结果
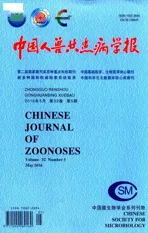
2.1HFMD患儿临床诊断SXQ1~4 4例轻症HFMD患儿有典型皮疹并伴发热,SXZ1~4 4例重症HFMD患儿尚有神经或呼吸系统症状和体征,但所有患儿标本HEV和HEV71 RT-PCR检测结果均为阳性(图1),表明上述患儿均感染了HEV71。
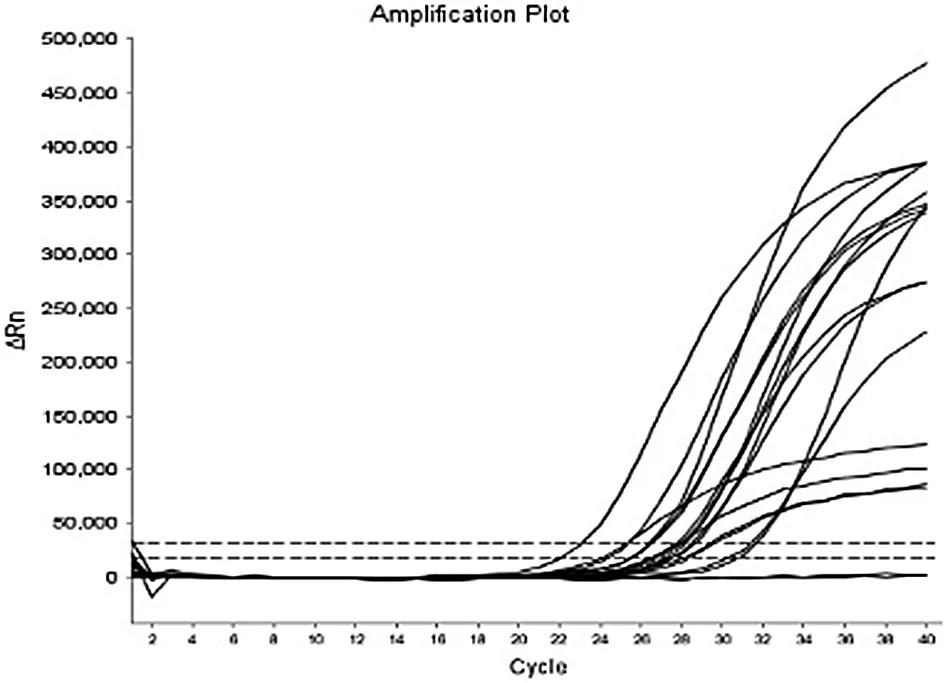
图1 8例HFMD患儿标本中HEV和HEV71 RT-PCR检测结果Fig.1 RT-PCR detection results of HEV and HEV71 in samples of eight HFMD children
2.2HFMD患儿病毒分离与鉴定结果SXQ1~4 4例轻症及SXZ1~4 4例重症HFMD患儿标本中分
离的病毒株RT-PCR检测结果显示均为HEV71,与患儿临床标本RT-PCR直接检测结果相符。上述HFMD患儿标本中HEV71感染Vero细胞3 d后,出现典型的细胞圆缩、分散、折光性增强甚至脱落等CPE现象(图2)。
2.3HEV71分离株VP1基因型分析结果与GenBank中HEV71各基因型参考标准株VP1基因序列(基因型/登录号:A/U22521、B0/AB524081、B1/AB524096、B2/AF135888、B3/AF376074、B4/AF376111、B5/DQ341364、C1/AB524215、C2/JQ621841、C3/JN874555、C4a/EU753409、C4b/AF302996、C5/AM490163)比较,SXQ1~4四例轻症及SXZ1~4四例重症HFMD患儿标本中分离的8株HEV71株VP1基因核苷酸及氨基酸序列均与C4a基因型相似性最高,分别为97.2%~98.8%和99.3%~99.7%(表1),表明所有患儿均感染了VP1-C4a基因型HEV71。
表1HEV71分离株VP1基因型比较结果
Tab.1Comparison results of VP1 genotypes of HEV71 isolates

基因型genotype核苷酸/氨基酸序列相似性(%)theidentitiesofnucleotideandaminoacidsequences(%)SXQ-1SXQ-2SXQ-3SXQ-4SXZ-1SXZ-2SXZ-3SXZ-4A81.9/94.381.4/94.682.4/95.382.3/94.982.2/94.382.0/94.682.0/94.381.7/94.3B084.6/96.384.9/96.985.2/96.684.7/96.384.7/96.384.3/95.984.9/96.384.3/96.9B184.4/96.683.9/97.384.9/96.984.9/96.684.7/96.683.8/96.384.9/96.684.3/97.3B284.1/96.383.8/96.984.6/96.684.6/96.384.2/96.383.8/95.984.6/96.384.2/96.9B384.5/96.683.8/96.984.6/96.984.2/96.684.6/96.684.5/96.384.9/96.684.2/96.6B483.5/96.983.5/97.683.4/97.383.6/96.983.4/96.983.4/96.683.9/96.983.5/97.3B583.6/96.983.2/96.983.7/97.383.5/96.983.7/96.983.6/96.683.8/96.983.2/96.6C189.8/98.989.1/98.990.1/98.789.2/98.990.0/98.989.2/98.789.6/98.988.9/98.7C288.3/98.387.9/98.488.2/98.388.2/98.788.8/98.387.8/97.988.6/98.387.9/97.9C388.8/98.388.7/98.989.1/97.988.4/98.388.8/98.387.9/97.988.8/98.388.3/98.7C4a98.7/99.797.3/99.798.8/99.398.1/99.798.4/99.797.4/99.397.2/99.797.4/99.3C4b92.7/96.992.0/96.992.7/96.692.0/96.993.2/96.992.4/96.692.0/96.992.3/97.3C587.9/98.787.9/98.787.8/98.387.9/98.788.1/98.787.3/98.388.2/98.986.9/98.3
2.4HEV71分离株VP1基因突变在HEV71-VP1基因rhv_like功能结构域中,有I113、A133、F135、F137、F155、V179、Y201、M230和M253 9个药物结合位点(图3)。尽管HEV71分离株VP1基因序列较为保守,但2株分离自重症HFMD患儿病毒株VP1基因第179位药物结合位点由缬氨酸(V)突变为亮氨酸(L),即出现V179L突变,其余2株分离自重症HFMD患儿以及所有4株分离自轻症HFMD患儿HEV71株VP1基因中药物结合位点均未发生突变(图4)。

图3 HEV71-VP1基因中功能结构域及药物结合位点Fig.3 Domains and drug-binding sites in VP1 genes of HEV71
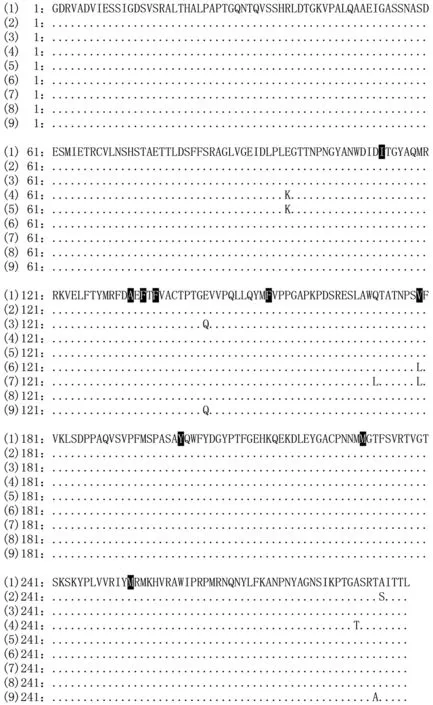
注:(2)~(5)分别为轻症患儿HEV71分离株SXQ1~4,(6)~(9)分别为重症患儿HEV71分离株SXZ1~4;黑底白色者为9个药物结合位点图4 8株HEV71分离株VP1基因氨基酸序列比较Fig.4 Amino acid sequence comparison of VP1 genes from eight HEV71 isolates
2.5HEV71分离株VP1基因系统进化树分析结果与国内外不同地区HEV71分离株VP1基因比较,3株分离自重症HFMD患儿标本及2株分离自轻症HFMD患儿标本的HEV71株(SXZ2~4,SXQ1和SXQ2)与安徽、湖南地区HEV71分离株亲缘关系较近,1株分离自重症HFMD患儿标本及2株分离自轻症HFMD患儿标本的HEV71株(SXZ1,SXQ3和SXQ4)与上海、山东地区HEV71分离株亲缘关系较近(图5)。

图5 不同地区HEV71分离株VP1基因系统进化树分析Fig.5 Analysis about phylogenetic evolution tree of VP1 genes in HEV71 isolates from different areas
3讨论
HFMD是由多种肠道病毒感染引起的儿童常见新发传染病(emerging infectious disease),其病原体有HEV71、柯萨奇病毒(coxasckievirus,CV)A组(CVA 2、4、5、6、10、16型)和B组(CVB 1~5型)、埃可病毒(echovirus,ECHO)等,但以HEV71和CVA16较为常见[2,20]。多数HFMD患儿临床症状和体征轻微,以手、足、口腔等处皮疹或疱疹及发热为主要特征,少数重症患儿可因并发神经系统病变、呼吸道感染、脑炎、心肌炎等导致死亡[16]。VP1不仅是HEV71主要衣壳蛋白, 也是肠道病毒血清型分型依据[9]。根据VP1基因核苷酸序列差异,HEV71分为A(BrCr原型株)、B0~5和C1~5基因型,其中C4基因型又可分为C4a和C4b亚型[21-25],不同地区优势流行的VP1基因型明显不同[13-15]。欧美国家主要流行C1和C2基因型,东南亚国家以B3~B5基因型为主,香港、台湾地区和韩国以C4和C5基因型为主[15,20-23]。我国1998年以来主要流行的HEV71一直是C4基因型, 但2004年前以C4b亚型为主,此后以C4a为主[14, 24]。本研究中来自4例轻症和4例重症HFMD患儿的HEV71分离株VP1基因序列分析结果显示,所有HEV71分离株VP1基因核苷酸及氨基酸序列与C4a基因型相似性最高(97.2%~98.8%和99.3%~99.7%),表明本地区主要流行的HEV71仍然是C4a基因型,且基因型与患儿病情严重程度无明显相关性。
HFMD患儿病情严重程度,不仅与其遗传因素、抗感染免疫力、病毒感染量及早期就诊等有关,HEV71抗药性以及不同HEV71株毒力强弱也可对患儿病情产生较大影响[16,25]。HEV71-VP1基因rhv_like功能结构域中有9个药物结合位点,若发生突变,可影响抗病毒药物治疗效果,从而对HFMD患儿病情产生不良影响[10-12]。我们的实验结果显示,2株分离自重症患儿HEV71株(SXZ1和SXZ2) VP1基因中第179位药物结合位点出现V179L突变,可能与病情严重程度有关。此外,SXQ2和SXZ4分离株VP1基因E145Q突变、SXZ2分离株VP1基因Q172L突变虽不在药物结合位点,但在药物结合位点区域内,是否与病毒抗药性有关有待于进一步研究。
系统进化树反映病原微生物分离株之间的亲缘关系,可在病原微生物传染源溯源中发挥重要作用。我们的VP1基因系统进化树分析结果显示,3例重症患儿标本中分离的HEV71株SXZ2~4、2例轻症患儿标本中分离的HEV71株SXQ1和SXQ2与安徽、湖南地区分离的HEV71株亲缘关系较近,但1例重症患儿标本中分离的HEV71株SXZ1、2例轻症HFMD患儿标本中分离的HEV71株SXQ3和SXQ4与上海、山东地区分离的HEV71株亲缘关系较近,提示本地区流行的HEV71来源复杂,这可能与本地区经济发达及人群流动性大有关。
参考文献:
[1] Solomon T, Lewthwaite P, Perera D, et al. Virology, epidemiology, pathogenesis, and control of enterovirus 71 [J]. Lancet Infect Dis, 2010, 10(11):778-790. DOI: 10.1016/S1473-3099(10)70194-8.
[2] Wang Y, Feng ZJ, Yang Y, et al. Hand, foot and mouth disease in China: patterns of spread and transmissibility during 2008-2009 [J]. Epidemiology, 2011, 22(6):781-792. DOI: 10.1097/EDE.0b013e318231d67a.
[3] Weng YW, Yan YS. Research progress on enterovirus 71[J].Chin J Zoonoses, 2014, 30(1):79-84. (in Chinese)
翁育伟,严延生.肠道病毒71型研究进展 [J]. 中国人兽共患病学报, 2014, 30(1):79-84. DOI:10.3969,j.issn.1002-2694.2014.01.017.
[4] Yamayoshi S, Yamashita Y, Li JF, et al. Scavenger receptor B2 is a cellular receptor for enterovirus 71[J]. Nat Med, 2009, 15(7):798-801. DOI: 10.1038/nm.1992.
[5] Nishimura Y,Shimojima M,Tano Y, et al. Human P-selectin glycoprotein ligand-1 is a functional receptor for enterovirus 71 [J]. Nat Med, 2009, 15(7):794-797. DOI: 10.1038/nm.1961.
[6] Foo DG, Alonso S, Phoon MC, et al. Identification of neutralizing linear epitopes from the VP1 capsid protein of enterovirus 71 using synthetic peptides [J]. Virus Res, 2007, 125(1):61-68. DOI:10.1016/j.virusres.2006.12.005.
[7] Kung YH, Huang SW, Kuo PH, et al. Introduction of a strong temperature-sensitive phenotype into enterovirus 71 by altering an amino acid of virus 3D polymerase [J]. Virology, 2010, 396(1):1-9. DOI: 10.1016/j.virol.2009.10.017.
[8] Li J, Huo XX, Dai Y, et al. Evidences for intertypic and intratypic recombinant events in EV71 of hand, foot and mouth disease during an epidemic in Hubei Province, China, 2011 [J]. Virus Res, 2012, 169(1):195-202. DOI: 10.1016/j.virusres.2012.07.028.
[9] Plevka P, Perera R, Cardosa J, et al. Crystal structure of humanenterovirus 71 [J]. Science, 2012, 336(6086):1274. DOI: 10.1126/science.1218713.
[10] Marchler-Bauer A, Anderson JB, Chitsaz F, et al. CDD: specific functional annotation with the Conserved Domain Database [J]. Nucleic Acids Res, 2009, 37(D):205-210. DOI: 10.1093/nar/gkn845.
[11] Marchler-Bauer A, Lu S, Anderson JB, et al. CDD: a Conserved Domain Database for the functional annotation of proteins [J]. Nucleic Acids Res, 2011, 39(D):225-229. DOI: 10.1093/nar/gkq1189.
[12] Marchler-Bauer A, Derbyshire MK, Gonzales NR, et al. CDD: NCBI's conserved domain database [J]. Nucleic Acids Res, 2015, 43(D):222-226. DOI: 10.1093/nar/gku1221.
[13] Deshpande JM, Nadkarni SS, Francis PP. Enterovirus 71 isolated from a case of acute flaccid paralysis in India represents a new genotype [J]. Currentence, 2003, 84(10):1350-1353.
[14] Zhang Y, Tan XJ, Wang HY, et al. An outbreak of hand, foot, and mouth disease associated with subgenotype C4 of human enterovirus 71 in Shandong, China [J]. J Clin Virol, 2009, 44(4):262-267. DOI: 10.1016/j.jcv.2009.02.002.
[15] Yip CC, Lau SK, Lo JY, et al. Genetic characterization of EV 71 isolates from 2004 to 2010 reveals predominance and persistent circulation of the newly proposed genotype D and recent emergence of a distinct lineage of subgenotype C2 in Hong Kong [J]. Virol J, 2013, 10:222-233. DOI: 10.1186/1743-422X-10-222.
[16] Health Ministry of the People's Republic of China. Diagnosis and treatment guideline on hand-foot-mouth disease[S].2013 (in Chinese)
中华人民共和国卫生部.手足口病诊疗指南(2013年版)[S].
[17] Yan JY, Lu YY, Xu CP, et al. Rapid detection of enterovirus with TaqMan real-time RT-PCR [J]. Chin J Public Health, 2007, 23(7):818-820.(in Chinese)
严菊英,卢亦愚,徐昌平,等. 肠道病毒TaqMan荧光定量RT-PCR法快速检测 [J]. 中国公共卫生杂志, 2007, 23(7):818-820. DOI:10.3321/j.issn:1001-0580.2007.07.023.
[18] Yan JY, Lu YY,Xu CP, et al. Rapid detection of enterovirus 71 by real time RT-PCR [J]. Chin J Public Health, 2009, 25(7):843-844. (in Chinese)
严菊英,卢亦愚,徐昌平,等. 肠道病毒EV71荧光定量RT-PCR法快速检测 [J]. 中国公共卫生杂志, 2009, 25(7):843-844. DOI:10.3321/j.issn:1001-0580.2009.07.062.
[19] Health Ministry of the People's Republic of China. Hang-foot-mouth disease control and prevention guide[S]. 2012.(in Chinese)
中华人民共和国卫生部. 手足口病预防控制指南(2012年版)[S].
[20] Wong SS, Yip CC, Lau SK, et al. Human enterovirus 71 and hand, foot and mouth disease [J]. Epidemiol Infect, 2010, 138(8):1071-1089. DOI:10.1017/s0950268809991555.
[21] van der Sanden S, Koopmans M, Uslu G, et al. Epidemiology of enterovirus 71 in the Netherlands, 1963 to 2008 [J]. J Clin Microbiol, 2009, 47(9):2826-2833. DOI:10.1128/JCM.00507-09.
[22] Cardosa MJ, Perera D, Brown BA, et al. Molecular epidemiology of human enterovirus 71 strains and recent outbreaks in the Asia-Pacific region: comparative analysis of the VP1 and VP4 genes [J]. Emerg Infect Dis, 2003, 9(4):461-468. DOI:10.3201/eid0904.020395.
[23] Chia MY,Chiang PS,Chung WY,et al. Epidemiology of enterovirus 71 infections in Taiwan [J]. Pediatr Neonatol, 2014, 55(4):243-249. DOI: 10.1016/j.pedneo.2013.07.007.
[24] Zhang Y, Wang J, Guo W, et al. Emergence and transmission pathways of rapidly evolving evolutionary branch C4a strains of human enterovirus 71 in the Central Plain of China [J]. PLoS One, 2011, 6(11):e27895-27907. DOI: 10.1371/journal.pone.0027895.
[25] He Y, Ong KC, Gao Z, et al. Tonsillar crypt epithelium is an important extra-central nervous system site for viral replication in EV71 encephalomyelitis[J]. Am J Pathol, 2014, 184(3):714-720. DOI: 10.1016/j.ajpath.2013.11.009.
DOI:10.3969/j.issn.1002-2694.2016.05.003
通讯作者:严杰,Email: med_bp@zju.edu.cn
中图分类号:R373
文献标识码:A
文章编号:1002-2694(2016)05-429-06
收稿日期:2015-12-22修回日期:2016-02-13
Isolation and identification of HEV71 strains from children with hand-foot-and-mouth disease in different conditions and analysis of their VP1 genotypes
JIANG Zhuo-jing1,2, HE Ting-ting2, CHEN Jin-kun2, YAN Jie1
(1.DepartmentofMedicalMicrobiologyandParasitology,ZhejiangUniversitySchoolofMedicine,Hangzhou310058,China;2.ShaoxingCenterforDiseaseControlandPrevention,Shaoxing312071,China)
Abstract:The aim of this study was to isolate the human enterovirus 71 (HEV71) strains from the hand-foot-and-mouth disease (HFMD)-suffering children with different pathogenetic conditions, and the VP1 genotypes of the viral isolates and the mutation of drug-binding sites in the VP1 genes were amalyzed. Firstly, HEV71 strains were isolated from the samples of four mild and four severe HFMD children, and then the viral isolates were identified by RT-PCR. The entire VP1 genes in the isolated HEV71 strains were amplified by RT-PCR for sequencing. Using professional bioinformatic softwares, the VP1 genotypes of the HEV71 isolates and the mutation of drug-binding sites in the VP1 genes were determined, and then the VP1 gene-based phylogenetic evolution tree of these viral isolates was generated. The results showed that HEV71 strains could be isolated from all the samples of the eight cases. Compared with the reported VP1-C4a genotype of HEV71, the identities of nucleotide and amino acid sequences of the viral isolates were 97.2%-98.8% and 99.3%-99.7%, respectively. The mutation at 179th drug-binding site in the VP1 genes (V179L) from two of the four severe cases was found. Five or three of the eight isolates presented the higher genetic relationship with those from Anhui and Hunan, or Shanghai and Shandong areas. All the results led to the conclusions that all the HEV71 strains isolated from the HFMD children in the local area with different pathogenetic conditions belong to VP1-C4a genotype, and the mutation at 179th drug-binding site may be associated with severity of the disease.
Key words:hand-foot-mouth disease/ HFMD; human enterovirus 71/ HEV71; VP1 gene; genotyping; drug-binding site/ mutation Corresponding author: Yan Jie, Email: med_bp@zju.edu.cn