特发性脊柱侧弯颈椎曲度影像学特征分析
2016-06-21邓俊才
唐 瑶,邓俊才,明 星,吴 非
(1.遵义医学院,贵州 遵义 563003;2.四川省医学科学院·四川省人民医院神经内科,四川 成都 610072;3.大连大学附属中山医院放射科,辽宁 大连 116000)
特发性脊柱侧弯颈椎曲度影像学特征分析
唐 瑶1,3,邓俊才2,明 星1,3,吴 非3
(1.遵义医学院,贵州 遵义 563003;2.四川省医学科学院·四川省人民医院神经内科,四川 成都 610072;3.大连大学附属中山医院放射科,辽宁 大连 116000)
目的 探讨特发性脊柱侧弯患者颈椎曲度的特点及颈椎曲度与脊柱侧弯角度大小的关系。方法 回顾性分析93例特发性脊柱侧弯患者全脊柱正侧位X射线片影像资料,在标准侧位片上测量颈椎矢状面Cobb角和颈椎夹角,在正位片上测量脊柱侧弯Cobb角。比较颈椎Cobb角和颈椎夹角的差异,分析脊柱侧弯Cobb角、颈椎Cobb角和颈椎夹角的相关性。结果 93例特发性脊柱侧弯患者侧弯Cobb角(27.9±16.9)°,颈椎矢状面Cobb角(-3.7±16.0)°,颈椎夹角(-2.0±16.6)°。颈椎Cobb角异常者占69.89%,颈椎夹角异常者占67.74%,颈椎Cobb角和颈椎夹角比较差异有统计学意义(t=-2.641,P= 0.010)。颈椎Cobb角与颈椎夹角呈正相关(r=0.935,P= 0.000);颈椎侧弯Cobb角与颈椎Cobb角及颈椎夹角呈弱正相关(r=0.246,P= 0.018;r=0.215,P= 0.039)。结论 特发性脊柱侧弯患者中颈椎矢状面曲度异常者占有较高的比例,颈椎矢状面曲度的大小与脊柱侧弯角度的大小无确切的相关性。
颈椎曲度;特发性脊柱侧弯;影像学
特发性脊柱侧弯是临床较为常见的脊柱畸形疾病之一,既往研究主要关注胸腰段畸形的发病原因、畸形特点及各种治疗方法等,而关于特发性脊柱侧弯患者颈椎曲度的研究较少。本研究对93例特发性脊柱侧弯患者颈椎的影像学资料进行回顾性分析,探讨其颈椎曲度的特点及颈椎曲度与脊柱侧弯角度大小的关系。
1 资料与方法
1.1 一般资料 收集四川省人民医院及大连大学附属中山医院2009年1月至2015年1月门诊和住院的特发性脊柱侧弯患者93例,男39例,女54例,年龄10~25岁[(15.62±3.36)岁]。纳入标准:标准全脊柱正侧位片符合特发性脊柱侧弯诊断的脊柱畸形患者。排除标准:既往有脊柱手术史、感染、肿瘤、椎体发育异常患者。
1.2 测量方法 患者均摄标准全脊柱正侧位X射线片,在标准侧位片上测量颈椎矢状面颈椎Cobb角及颈椎夹角,在正位片上测量脊柱侧弯主弯Cobb角(图1)。颈椎Cobb角分别自C2、C7椎体下缘做切线,切线之间的夹角作为颈椎弧度值。颈椎夹角分别自C2、C7椎体后缘作切线,取两线间的夹角。脊柱侧弯Cobb角上端椎上缘平行线与下端椎下缘平行线的夹角。颈椎Cobb角和颈椎夹角>5°为颈椎曲度正常,<5°为颈椎曲度异常(-5°~5°为变直,<-5°为后凸)[1,2]。
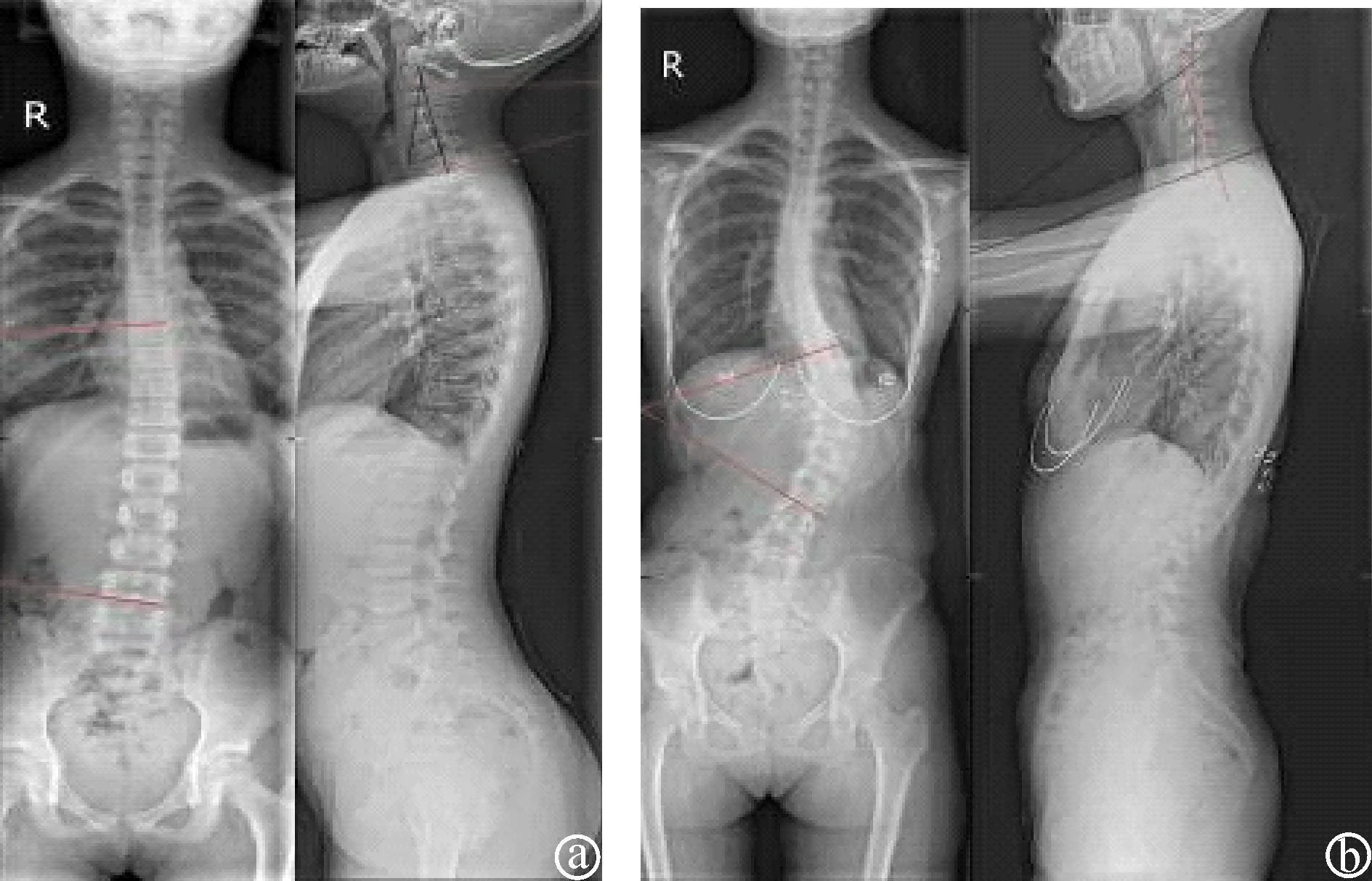
图1 脊柱侧弯X射线片 a:Cobb角14°,颈椎Cobb角17°,颈椎夹角15°;b:Cobb角48°,颈椎Cobb角-15°,颈椎夹角-18°
1.3 统计学方法 采用SPSS 19.0统计软件进行数据分析。计量资料以均数±标准差表示,颈椎Cobb角和颈椎夹角比较采用t检验;脊柱侧弯Cobb角、颈椎Cobb角与颈椎夹角相关性分析采用Pearson相关分析。P< 0.05为差异有统计学意义。
2 结果
2.1 颈椎矢状面及脊柱侧弯参数分析 93例患者侧弯Cobb角(27.9±16.9)°,颈椎矢状面Cobb角(-3.7±16.0)°,颈椎夹角(-2.0±16.6)°。按照颈椎Cobb角和颈椎夹角大小分组结果见表1。颈椎Cobb角和颈椎夹角比较差异有统计学意义(t=-2.641,P< 0.05)。
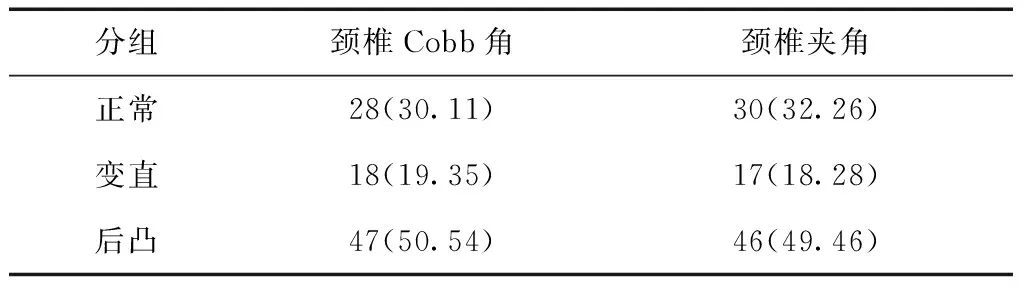
表1 颈椎Cobb角和颈椎夹角大小分组构成比 [n(%)]
2.2 脊柱侧弯与颈椎曲度的相关性分析 颈椎Cobb角与颈椎夹角呈正相关(r=0.935,P= 0.000,见图2);颈椎侧弯Cobb角与颈椎Cobb角及颈椎夹角呈弱正相关(r=0.246,P= 0.018,见图3;r=0.215,P= 0.039,见图4)。
3 讨论
3.1 特发性脊柱侧弯患者颈椎曲度变化 关于特发性脊柱侧弯患者颈椎曲度的研究国外已讨论多年[3~6]。目前关于颈椎畸形在特发性脊柱侧弯患者中的发生率还未有大样本流行病学调查结果,Canavese等[4]在32例特发性脊柱侧弯患者中发现,有34.4%患者伴有的平均11°的颈椎后凸畸形,Smith等[5]通过对470例成人胸椎畸形的患者进行调查分析发现有31%的患者伴发有颈椎后凸畸形。国内有研究表明有40%的青少年特发性脊柱侧弯患者合并有颈椎后凸畸形[7]。本组研究中特发性脊柱侧弯患者中颈椎Cobb角异常者占69.89%(5°~-5°者占19.35%,<-5°者占50.54%),颈椎夹角异常者占67.74%(5°~-5°者占18.28%,<-5°者占49.46%),研究结果显示特发性脊柱侧弯患者中颈椎曲度异常者占有较大的比例。在临床工作中对于特发性脊柱侧弯患者在关注侧弯脊柱节段的同时也应关注脊柱整体的序列,尤其对伴发有颈椎后凸畸形的患者,应通过各种措施予以干预,尽可能改善颈椎曲度,防止颈椎后凸加重,避免出现远期的颈脊髓神经症状。对于颈椎后凸畸形不严重、神经脊髓没有明显压迫的患者,通过非手术综合治疗干预,可显著改善患者的临床症状,减小后凸角度,有效阻止后凸畸形加重[8]。

图2 颈椎Cobb角与颈椎夹角的散点图
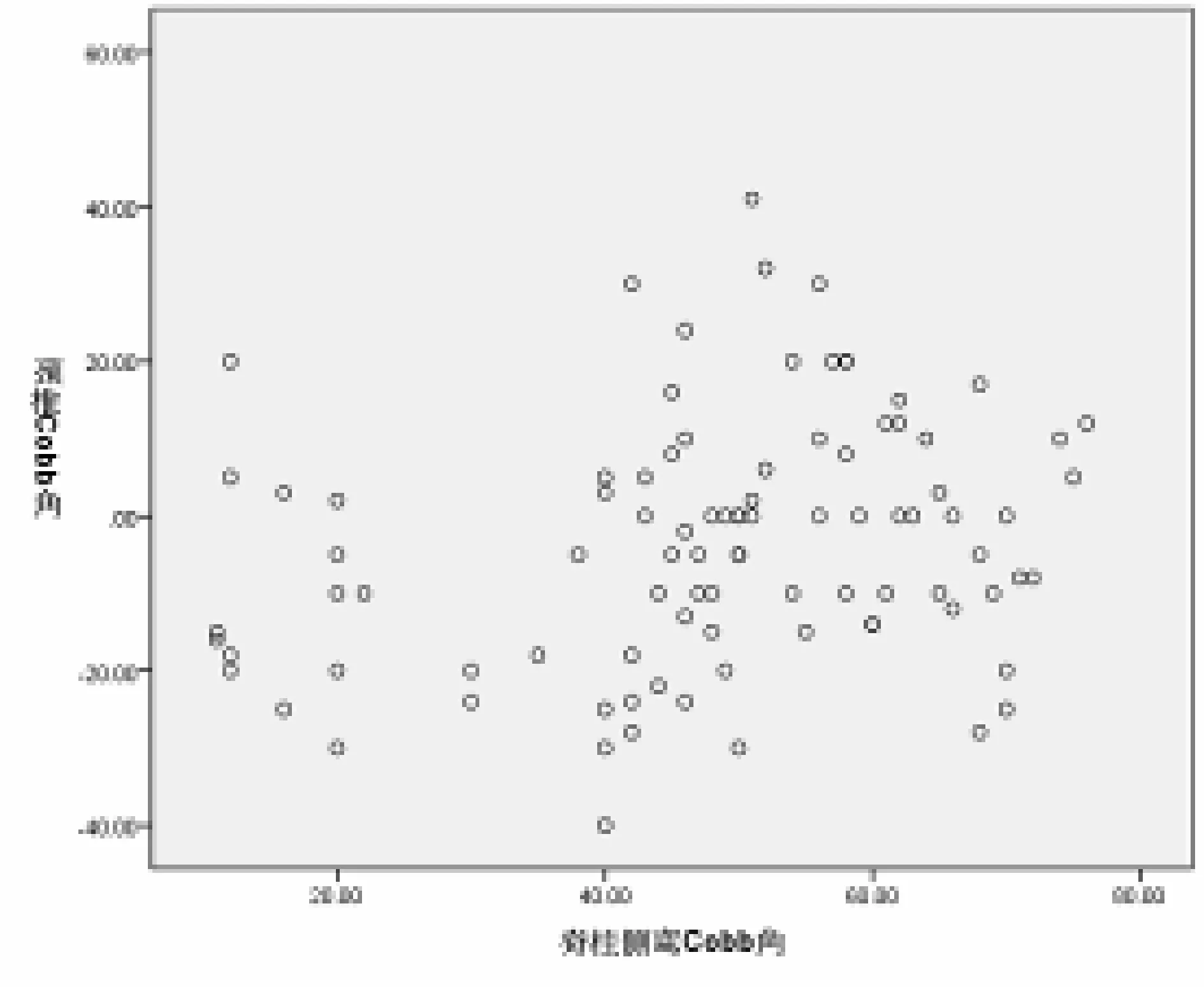
图3 颈椎Cobb角与脊柱侧弯Cobb角的散点图
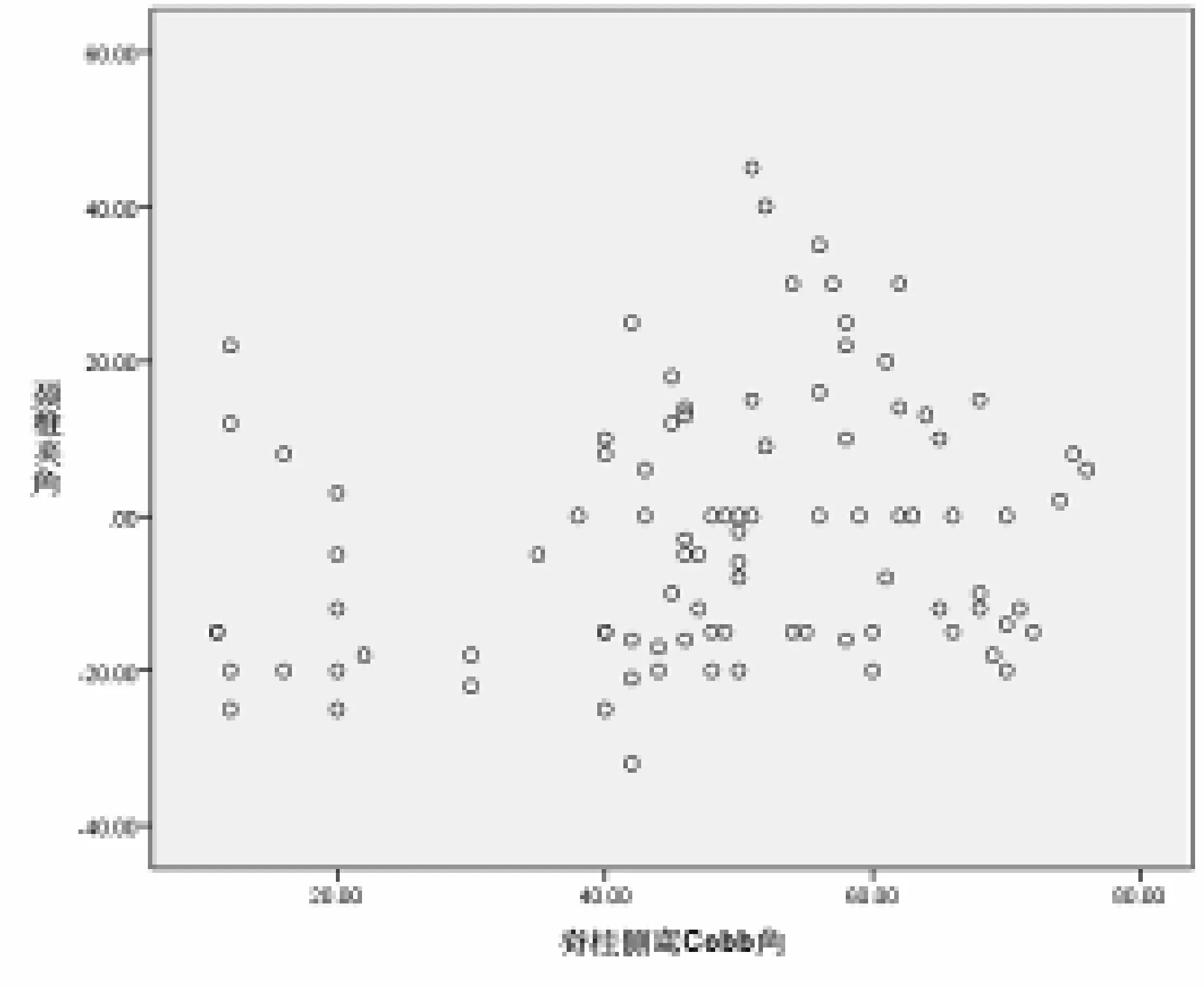
图4 颈椎夹角与脊柱侧弯Cobb角的散点图
3.2 颈椎曲度的评价方法 在多种影像学快速发展的今天,影像学所提供的信息甚至已经超过临床症状表示与临床体征发生[9]。关于颈椎曲度的测量评价方法很多,有研究表明使用不同的测量方法可直接影响对颈椎异常曲度的判断[10],选择适当颈椎曲度评价方法对颈椎疾病的临床诊治、尤其是对选择手术矫形的患者具有非常重要的临床意义。目前临床上采用的颈椎曲度测量法有Borden法、Ishihara法、Harrison法、Cobb法等。Borden法[11]的优点在于可最大限度避免椎体退变所造成的影响,但因个体骨骼大小的差异和X射线片放大率的不同,影响测量数据的准确性[12]。Ishihara法[13]又称曲率法,因个体差异较大,颈椎曲度变直或S形时变异指数较高,且计算相对复杂,临床应用甚少。Harrison法[14]即颈椎夹角、也称颈椎后切线夹角,此法不仅可用于全颈段的夹角测量,可更精确地应用于颈椎的每一个节段,每个节段的角度能反应颈椎曲度的变化趋势,变化趋势中断表示颈椎曲度异常。Cobb法,临床广泛应用于颈椎、胸椎、腰椎的矢状面的曲度变化及脊柱侧弯角度的测量。目前临床上应用最为广泛的测量方法为Cobb法和Harrison法,Harrison法是测量椎体后缘夹角,更准确地反映了颈椎的曲度,而Cobb法则是测量椎体终板间的夹角,椎体的终板与椎体的后缘并非绝对垂直,导致Cobb法的测量结果降低对颈椎曲度的评价,Harrison等通过研究认为,后切线夹角较Cobb法更能准确地反应颈椎曲度[1,13,15]。因此,本研究采用Cobb法和Harrison法测量颈椎Cobb角和环椎夹角,结果显示二者呈高度相关性,但两种测量方法测得的数据比较结果具有显著差异,证明不同的测量方法可直接影响对颈椎曲度的判断。
3.3 特发性脊柱侧弯与颈椎曲度的相关性 颈椎作为脊柱整体的一部分,其曲度与脊柱其他节段的曲度相关,目前国内外关于脊柱侧弯与颈椎曲度的相关研究报道较多[5~7,16~18],但颈椎曲度与脊柱侧弯相关性的研究还不够深入。有研究认为颈椎后凸畸形同全脊柱矢状序列存在相关性,并且是青年特发性脊柱侧弯颈胸矢状面畸形的一部分[7],另有一些研究表明在特发性脊柱侧弯患者中颈椎的曲度与胸椎的后凸有一定相关性,腰椎的前凸量影响颈椎的前凸,胸椎的后凸量影响颈椎的曲度,胸椎的后凸角度过小会发生代偿性颈椎后凸[19~22]。既往多项研究已经证实胸腰椎矢状面曲度会影响颈椎的曲度,但没有研究证实特发性脊柱侧弯患者中脊柱侧弯角度的大小与颈椎曲度的大小有一定的相关性,本研究结果显示,不管是颈椎Cobb角还是颈椎夹角,与脊柱侧弯角度大小相关性较弱。
综上所述,特发性脊柱侧弯患者中颈椎矢状面曲度异常者占有较高的比例,本研究显示脊柱侧弯角度的大小与颈椎矢状面曲度大小的相关性较弱,确切的结论需要今后进一步的探讨。
[1] Loder RT.The sagittal profile of the cervical and lumbosacral spine in scheuermann thoracic kyphosis[J].J Spinal Disord,2001,14:226-231.
[2] Bone E,Vaccaro AR,Fehlings M,et al.Measurement techniques for lower cervical spine injuries:consensus statement of the spine trauma study group[J].Spine,2006,31(5):603-609.
[3] Hilibrand A,Tannenbaum D,Graziano G,et al.The sagittal alignment of the cervical spine in adolescentidiopathic scoliosis[J].J Pediatr Orthop,1995,15(5):627-632.
[4] Canavese F,Turcot K,De Rosa V,et al.Cervical spinesagittal alignment variations following posterior spinal fusion andinstrumentation for adolescent idiopathic scoliosis[J].Eur Spine J,2011,12(7):1141-1148.
[5] Smith JS,Lafage V,Schwab FJ,et al.Prevalence and type of cervical deformity among 470 adults with thoracolumbar deformity[J].Spine,2014,9(17):1001-1009.
[6] Aykac B,Ayhan S,Yuksel S,et al.Sagittal alignment of cervical spine in adult idiopathic scoliosis[J].Eur Spine J,2015,24(6):1175-1182.
[7] Yu M,Silvestre C,Mouton T,et al.Analysis of the cervical spine sagittal alignment in young idiopathic scoliosis:a morphological classification of 120 cases[J].Eur Spine J,2013,2(11):2372-2381.
[8] 胡豇,邓俊才,唐六一,等.非手术治疗轻度颈椎后凸畸形的疗效观察[J].实用医院临床杂志,2014,11(4):198-200.
[9] 蒋瑾,于淼淼.影像学的发展与颈椎退行性变的诊断和治疗[J].实用医院临床杂志,2012,9(2):168-170.
[10]Ohara A,Miyamoto K,Naganawa T,et al.Reliabilities of correlations among five standard methods of assessing the sagittal alignment of the cervical spine[J].Spine,2006,31(22):2585-2591.
[11]Borden AG,Rechtman AM,Gershon CJ.The normal cervical lordosis[J].Radiology,1960,74:806-809.
[12]万超,沈惠良,刘钊.Borden氏法与Harrison氏法测量颈椎曲度的一致性比较[J].中国脊柱脊髓杂志,2012,22(1):34-36.
[13]Ishihara A.Roentgenographic studies on the normal pattern of the cervical curvature[J].Nihon Seikeigeka Gakkai Zasshi,1968,42(11):1033-1044.
[14]Harrison DE,Harrison DD,Cailliet R,et al.Cobb method or Harrison posterior tangent method:which to choose for lateral cervical radiographic analysis[J].Spine,2000,25(16):2072-2078.
[15]Troyanovich SJ,Stroink AR,Kattner KA,etal.Does anterior plating maintain cervical lordosis versus conventional fusion techniques?A retrospective analysis of patients receiving single-level fusions[J].J Spinal Disord Tech,2002,15:69-74.
[16]Boissière L,Bernard J,Vital JM,et al.Cervical spine balance:postoperative radiologic changes in adult scoliosis surgery[J].Eur Spine J,2015,24(7):1356-1361.
[17]Vidal C,Ilharreborde B,Azoulay R,et al.Reliability of cervical lordosis and global sagittal spinal balance measurements in adolescent idiopathic scoliosis[J].Eur Spine J,2013,22(6):1362-1367.
[18]Hilibrand AS,Tannenbaum DA,Graziano GP,et al.The sagittal alignment of the cervical spine in adolescent idiopathic scoliosis[J].J PediatrOrthop,1995,15(5):627-632.
[19]Hwang SW,Samdani AF,Tantorski M,et al.Cervical sagittal plane decompensation after surgery for adolescent idiopathic scoliosis:an effect imparted by postoperative thoracic hypokyphosis[J].J Neurosurg Spine,2011,15(5):491-496.
[20]Roussouly P,Labelle H,Rouissi J,et al.Pre-and post-operative sagittal balance in idiopathic scoliosis:a comparison over the ages of two cohorts of 132 adolescents and 52 adults[J].Eur Spine J,2013,22(2):203-215.
[21]Legarreta CA,Barrios C,Rositto GE,et al.Cervical and thoracic sagittal misalignment after surgery for adolescent idiopathic scoliosis:a comparative study of all pedicle screws versus hybrid instrumentation[J].Spine,2014,39(16):1330-1337.
[22]Charles YP,Sfeir G,Matter-Parrat V,et al.Cervical sagittal alignment in idiopathic scoliosis treated by posterior instrumentation and in situ bending[J].Spine,2015,40(7):419-427.
Imaging features of cervical spine curvature of idiopathic scoliosis
TANG Yao1,DENG Jun-cai2,MING Xing1,WU Fei3
(1.Zunyi Medical University,Zunyi 563003,China;2.Department of Orthopedics,Sichuan Academy of Medical Sciences & Sichuan Provincial People’s Hospital,Chengdu 610072,China;3.Department of Radiology,Zhongshan Hospital Affiliated to Dalian University,Dalian 116000,China)
WUFei
Objective To analyze the imaging characteristics of cervical spine curvature of idiopathic scoliosis and to explore the relationship between cervical curvature and scoliosis angle size.Methods Frontal and lateral full-spine X-ray imaging of 93 patients with idiopathic scoliosis were retrospectively analyzed.Cervical sagittal Cobb angle and cervical spine angle were measured on lateral view,and scoliosis Cobb angle was measured on the anteroposterior films.The differences between cervical Cobb angle and the cervical angle were compared and the correlation among cervical sagittal Cobb angle,scoliosis Cobb angle,and cervical spine angle was analyzed.Results In the 93 patients,the scoliosis Cobb angle was (27.9±16.9)°,cervical sagittal Cobb angle (-3.7±16.0)° and average of cervical angle was (-2.0±16.6)°.The abnormalities of cervical Cobb angle accounted for 69.89%.The abnormalities of cervical angle accounted for 67.74%.There was a significant difference between cervical Cobb angle and the cervical angle (t=-2.641,P= 0.010).They were highly correlated (r= 0.935,P= 0.000).The correlations between cervical scoliosis Cobb angle and Cobb angle and between cervical scoliosis Cobb angle and cervical angle were weak (r= 0.246,P= 0.018 andr= 0.215,P= 0.039,respectively).Conclusion The abnormalities of curvature in sagittal cervical of idiopathic scoliosis have a high proportion.There is no exactly correlation between the size of the curvature in sagittal cervical and the scoliosis curvature.
Cervical curvature; Idiopathic scoliosis; Imaging
吴 非
R682.3;R814.41
A
1672-6170(2016)04-0119-04
2015-11-03;
2016-01-24)
