汉族人群载脂蛋白A5基因多态性与2型糖尿病易感性及肾损害的关系*
2022-10-13洪娟苏钢宣小明吴水梅
洪娟, 苏钢, 宣小明, 吴水梅
汉族人群载脂蛋白A5基因多态性与2型糖尿病易感性及肾损害的关系*
洪娟, 苏钢△, 宣小明, 吴水梅
(芜湖市第一人民医院全科医学科,安徽 芜湖 241000)
探讨载脂蛋白A5()基因多态性与汉族人群2型糖尿病(T2DM)易感性及肾损害的关系。选取汉族T2DM患者189例(T2DM组),且根据随机配对原则选取189例健康者(对照组),另根据T2DM组患者肾脏检查情况将其分为肾损害者与无肾损害者。采取聚合酶链反应-限制性片段长度多态性(PCR-RFLP)检测受检对象-1131T>C和c.553G>T基因型及统计等位基因频率,并采用logistic回归分析法分析基因多态性与汉族T2DM易感性及肾损害的关系。T2DM组基因-1131T>C位点的TC基因型和c.553G>T位点的GT基因型占比均高于对照组,T2DM组-1131T>C位点等位基因C和c.553G>T位点等位基因T频率均高于对照组,差异均有统计学意义(<0.05);T2DM组并发肾损害者基因-1131T>C位点的TC基因型和c.553G>T位点的GT基因型占比均高于无肾损害者,-1131T>C位点等位基因C和c.553G>T位点等位基因T频率均高于无肾损害者,差异均有统计学意义(<0.05);经logistic回归分析,-1131T>C位点的基因型TC和等位基因C,以及c.553G>T位点的基因型GT和等位基因T均可增加汉族人群T2DM发生风险[优势比(OR)分别为3.575、2.782、4.063和3.995,<0.05]及并发肾损害风险(OR分别为2.807、2.347、2.977和2.954,<0.05)。基因-1131T>C和c.553G>T多态性均与汉族人群T2DM易感性及并发肾损害有关,其中-1131T>C位点基因型TC和等位基因C携带者,以及c.553G>T位点基因型GT和等位基因T携带者发生T2DM及肾损害的风险更高。
载脂蛋白A5;基因多态性;2型糖尿病;肾损害
糖尿病(diabetes mellitus, DM)属于全身慢性代谢性疾病,在临床以2型DM(type 2 DM, T2DM)最为常见,其常可并发微血管病变,引发肾损害,严重威胁人类身体健康与生命安全[1]。除典型的糖代谢紊乱外,血脂代谢异常亦是T2DM的重要特征之一,可增加患者心脑血管病变等发生风险。T2DM属于多基因遗传性疾病,与遗传及环境因素紧密相关。载脂蛋白A5(apolipoprotein A5, ApoA5)在血脂代谢中发挥重要调控作用,其与甘油三酯浓度关系密切,可降低血清甘油三酯和低密度脂蛋白胆固醇含量[2]。近年来,单核苷酸多态性已逐渐应用于人类患病风险的探索分析中,对指导临床防控具有重要意义。-1131T>C、c.56C>G和c.553G>T是当前研究较多的基因多态性位点,已有研究报道,-1131T>C多态性可影响血清甘油三酯浓度[3],且c.553G>T与汉族高甘油三酯血症发病存在一定的相关性[4]。但关于基因多态性是否与汉族T2DM易感性及肾损害有关尚需进一步探讨。而c.56C>G在亚洲人群中存在极低,有研究显示,对贵州汉族老年人群行基因c.56C>G多态性检测,只检测出基因型CC[5]。鉴于此,本研究特探讨基因-1131T>C和c.553G>T多态性与汉族T2DM易感性及肾损害的关系,为临床预防及治疗提供依据及新思路。
材料和方法
1 一般资料
选取汉族人群378名,其中男201例,女177例;年龄28~80岁,平均(55.23±9.69)岁;体质量指数17.94~28.13 kg/m2,平均(22.11±2.08) kg/m2。纳入标准:均为汉族人群,无血缘关系;知情同意,且自愿参与研究。排除标准:伴心、肝、肺功能障碍者;伴脑血管疾病者;伴原发性肾病综合征、肾小球肾炎等;伴自身免疫性疾病;伴甲状腺功能亢进或减退等。本研究符合《世界医学协会赫尔辛基宣言》。
2 方法
2.1分组对选取的汉族人群行血糖、糖化血红蛋白、胰岛素等检查,根据《中国2型糖尿病防治指南》[6]中T2DM诊断标准,其中有189例符合T2DM诊断标准,将其归为T2DM组;另根据随机配对原则,选取189名健康者(血糖和血脂水平正常,无肾脏、内分泌等疾病,无糖尿病家族史),将其归为对照组。
2.2T2DM组患者肾脏检查均抽取患者空腹静脉血并送至本院检验科,检查血清肌酐、血尿素氮、胱抑素C、内生肌酐清除率等指标;收集患者24 h尿液,检测24 h尿蛋白、尿微量白蛋白、尿微球蛋白等,并检测尿白蛋白/肌酐比值、肾小球滤过率等;另行肾脏彩超检查,观察肾体积及结构改变。结合上述检查结果及临床表现,判断患者肾损害发生情况[7],将其分为肾损害者和无肾损害者。
2.3基因多态性检测(1)提取外周血DNA:均抽取受试者外周肘静脉血2 mL,抗凝,根据DNA提取试剂盒(北京诺博莱德科技有限公司)说明书操作步骤进行基因组DNA提取;然后取5 μL的基因组DNA+1 μL的6×上样缓冲液进行点样,以1%琼脂糖凝胶电泳(90 V电压)60 min后,放置于凝胶成像仪上,观察基因组DNA亮度与纯度。(2)PCR扩增:参照相关文献[8-9]设计引物,并由上海生工生物工程股份有限公司合成。-1131T>C的上游引物序列为5'-GGAGCTTGTGAACGTGTGTATGAGT-3',下游引物序列为5'-CTACAGCCAGAACCCGAGCAG-3',产物长度为188 bp(图1);c.553G>T的上游引物序列为5'-AGACACCAAGGCCCAGTTGCTGGG-3',下游引物序列为5'-ATGCCGCTCACCAGCTCTCG-3',产物长度为227 bp(图2)。扩增体系为25 μL,含3 μL模板DNA、12.5 μL Premix Taq、0.3 μL上游引物和0.3 μL下游引物,再以双蒸水补充。扩增条件为:94 ℃预变性5 min;94 ℃变性30 s,59 ℃复性30 s,72 ℃延伸30 s,共计35个循环;然后72 ℃延伸7 min。取5 μL的PCR产物以2%琼脂糖凝胶电泳(90 V电压)40 min后,放于凝胶成像仪观看并摄像,确定是否为目的DNA。(3)PCR产物酶切:-1131T>C位点以I限制性内切酶在37 ℃水浴下4 h进行消化,酶切反应体系为8 μL的PCR产物、2 μL的10×缓冲液、0.5 μL的I、0.2 μL的牛血清白蛋白溶液和9.3 μL的双蒸水;c.553G>T以I限制性内切酶在37 ℃水浴下4 h进行消化,反应体系为5 μL的PCR产物、2.5 μL的10×缓冲液、1 μL的I和16.5 μL的双蒸水。酶切产物均以4%琼脂糖凝胶电泳(80 V电压)2 h后,置于凝胶成像仪观看且摄像。

Figure 1. Electrophoretic map of -1131T>C gene polymorphism digested by Mse I enzyme. M: DNA marker; 1 to 10: homozygotes of different genotypes.
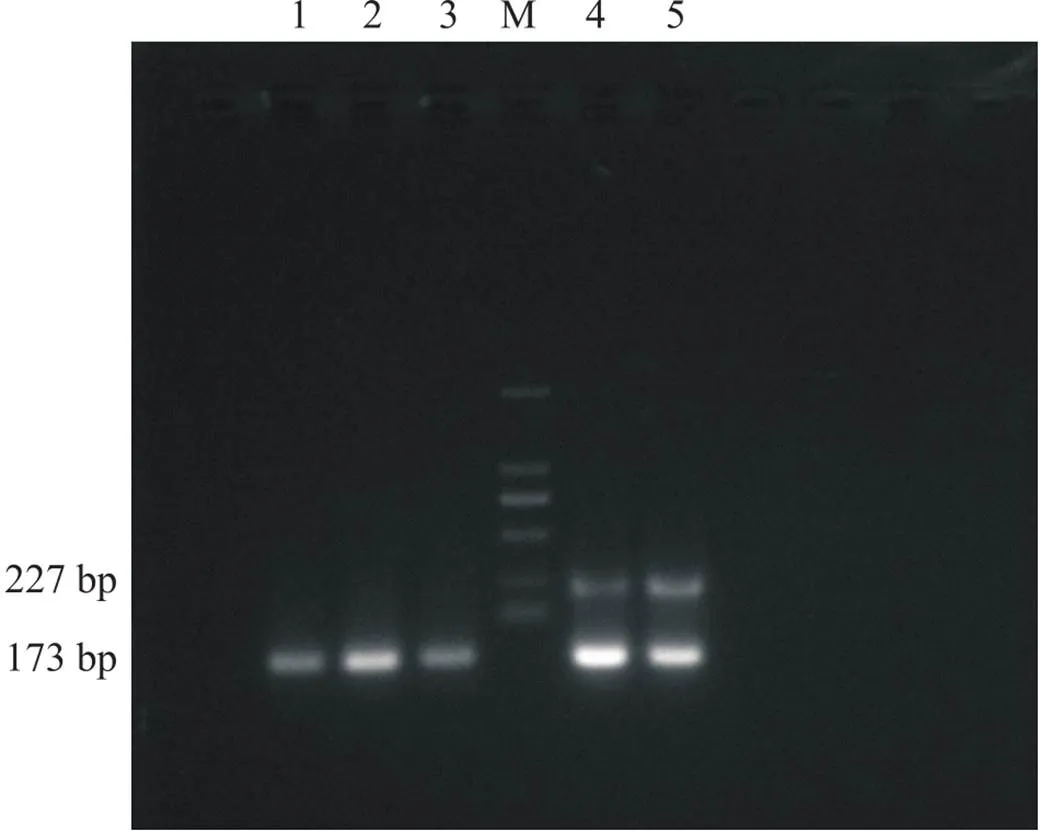
Figure 2. Electrophoretic map of c.553G>T gene polymorphism digested by Msp I enzyme. M: DNA marker; 1 to 5: homozygotes of different genotypes.
2.4基因多态性与汉族T2DM易感性及肾损害的关系分析以-1131T>C和c.553G>T基因型和等位基因分布情况为自变量,以T2DM发生情况和肾损害发生情况为因变量,进行logistic回归分析。
3 统计学方法

结果
1 T2DM组与对照组ApoA5基因多态性分布情况
T2DM组基因-1131T>C位点的TC基因型和c.553G>T位点的GT基因型占比均高于对照组,T2DM组-1131T>C位点的TT基因型和c.553G>T位点的GG基因型占比均低于对照组,差异均有统计学意义(<0.05);T2DM组-1131T>C位点等位基因C和c.553G>T位点等位基因T频率均高于对照组,差异均有统计学意义(<0.05),见表1、2。

表1 T2DM组与对照组ApoA5基因多态性的基因型分布
**<0.01control group.

表2 T2DM组与对照组ApoA5基因多态性的等位基因分布
*<0.05,**<0.01control group.
2 T2DM组肾损害者与无肾损害者ApoA5基因多态性分布情况
根据临床检查及患者表现、体征等,T2DM组189例患者中有43例并发肾损害;并发肾损害者基因-1131T>C位点的TC基因型和c.553G>T位点的GT基因型占比均高于无肾损害者,肾损害者-1131T>C位点的TT基因型和c.553G>T位点的GG基因型占比均低于无肾损害者,差异均有统计学意义(<0.05);肾损害者-1131T>C位点等位基因C和c.553G>T位点等位基因T频率均高于无肾损害者,差异均有统计学意义(<0.05),见表3、4。

表3 T2DM组肾损害者与无肾损害者ApoA5基因多态性的基因型分布
*<0.05,**<0.01without renal damage.

表4 T2DM组肾损害者与无肾损害者ApoA5基因多态性的等位基因分布
*<0.05,**<0.01without renal damage.
3 ApoA5基因多态性与汉族T2DM易感性及肾损害的关系
经logistic回归分析,-1131T>C位点基因型TC和等位基因C,以及c.553G>T位点基因型GT和等位基因T均可增加汉族T2DM发生风险(OR分别为3.575、2.782、4.063和3.995,<0.05)及并发肾损害风险(OR分别为2.807、2.347、2.977和2.954,<0.05),见表5、6。

表5 ApoA5基因多态性与汉族T2DM易感性的logistic回归分析

表6 ApoA5基因多态性与汉族T2DM并发肾损害的logistic回归分析
讨论
糖代谢异常是T2DM的重要临床特征,T2DM病因及发病机制复杂,多认为该病与遗传因素、环境因素、胰岛素抵抗等有关。长期的糖代谢紊乱可引发多种血管病变,其中糖尿病肾病(diabetic nephropathy, DN)是DM患者常见的微血管病变,严重影响患者生存质量[10]。此外,以甘油三酯升高为主要特征的血脂代谢异常亦在DM的发生发展进程中占据重要地位,且有研究报道,其参与了DN的发病[11]。T2DM相关基因多态性是近年来研究的热点,而ApoA5可影响甘油三酯水平,本研究特对基因多态性与汉族T2DM易感性及肾损害的关系进行探讨,以期能够为临床工作提供实验依据及思路。
本研究结果发现,T2DM组基因-1131T>C位点的TC基因型和等位基因C,以及c.553G>T位点的GT基因型和等位基因T的占比均较对照组高,且logistic回归分析显示,以上均是汉族T2DM发病的危险因素。血脂代谢紊乱,可导致游离脂肪酸增加,进而促使胰岛素生物活性降低,影响糖代谢,引发DM[12]。ApoA5对甘油三酯具有重要调节作用,其可激活脂蛋白脂酶而加速甘油三酯水解,并可对极低密度脂蛋白的合成与分泌产生抑制作用等。有研究表明,基因多态性可能与代谢综合征的发病有关[13]。基因-1131T>C位于启动子区域,相关研究报道,-1131T>C与甘油三酯、低密度脂蛋白胆固醇等有关,可增加血浆甘油三酯含量,增加代谢综合征发病风险[14]。另有研究表明,-1131T>C基因型TC携带者发生代谢综合征的风险较基因型TT携带者高,代谢综合征患者-1131T>C等位基因C频率较健康人群高[15]。此外,有研究报道,T2DM患者-1131T>C基因型TC频率较正常健康体检者高[16],此与本研究结果相符合。c.553G>T位于编码区第4个外显子处,有研究显示,其与血脂含量相关,对中国人高甘油三酯血症可能具有一定的预测作用[17]。另有研究报道,冠心病患者基因c.553G>T基因型GT占比高于健康者,冠心病等位基因T携带者血清甘油三酯水平高于等位基因G携带者[18]。基因c.553G>T与血脂代谢紊乱具有一定的相关性,可进一步增加DM发生几率,其中T等位基因携带者发生DM的风险更高。
本研究结果还发现,T2DM组并发肾损害者基因-1131T>C位点的TC基因型和等位基因C,以及c.553G>T位点的GT基因型和等位基因T频率的占比均较无肾损害者高,且经logistic回归分析显示,以上均是T2DM并发肾损害的危险因素。有研究表明,基因-1131T>C多态性与T2DM患者DN的发生具有一定的相关性,其中含C等位基因者患DN的风险较含T等位基因者高[19]。另有研究显示,基因c.553G>T的等位基因T可增加高甘油三酯血症发生风险,与血脂代谢紊乱存在一定的关系[20]。血脂代谢异常可造成肾小球毛细血管壁损伤,引发肾损害。此外,有研究报道,DN患者中携带等位基因C者的血清同型半胱氨酸水平较等位基因T携带者高,但DN组-1131T>C各基因型及等位基因频率与健康对照组无明显差异[21],此与本研究结果不相符合,可能与所选样本数量及个体间的差异有关。
综上所述,-1131T>C和c.553G>T基因多态性均与汉族T2DM易感性及并发肾损害有关,其中-1131T>C位点基因型TC和等位基因C携带者,以及c.553G>T位点基因型GT和等位基因T携带者发生T2DM及肾损害的风险更高。但本研究尚存在一定的不足,关于基因多态性的具体作用机制仍需进一步探讨。
[1]赵心怡, 吴勇, 黄文庆, 等. 葡萄糖上调胰腺β细胞CFTR表达而升高胰岛素水平在2型糖尿病中的作用[J]. 中国病理生理杂志, 2021, 37(11):1942-1948.
Zhao XY, Wu Y, Huang WQ, et al. Elevated insulin level in pancreatic islet β cells by glucose via up-regulation of CFTR contributes to pathogenesis of type 2 diabetes mellitus[J]. Chin J Pathophysiol, 2021, 37(11):1942-1948.
[2] Castleberry M, Davis X, Liu M, et al. Functional recombinant apolipoprotein A5 that is stable at high concentrations at physiological pH[J]. J Lipid Res, 2020, 61(2):244-251.
[3] Kim M, Yoo HJ, Lee HJ, et al. Longitudinal interaction between-1131T>C and overweight in the acceleration of age-related increase in arterial stiffness through the regulation of circulating triglycerides[J]. Hypertens Res, 2019, 42(2):241-248.
[4] Kim M, Kim M, Yoo HJ, et al. A promoter variant of thegene increases atherogenic LDL levels and arterial stiffness in hypertriglyceridemic patients[J]. PLoS One, 2017, 12(12):e0186693.
[5]黄健, 黄韻祝, 杨国珍, 等. 贵州汉族老年人群载脂蛋白A5基因多态性与2型糖尿病的相关性[J]. 中国老年学杂志, 2015, 35(19):5514-5516.
Huang J, Huang YZ, Yang GZ, et al. Association between apolipoprotein A5 gene polymorphism and type 2 diabetes in Guizhou Han elderly population[J]. Chin J Gerontol, 2015, 35(19):5514-5516.
[6]中华医学会糖尿病学分会. 中国2型糖尿病防治指南(2017年版)[J]. 中国实用内科杂志, 2018, 38(4):292-344.
Chinese Diabetes Society. Guidelines for the prevention and control of type 2 diabetes in China (2017 Edition)[J]. Chin J Pract Intern Med, 2018, 38(4):292-344.
[7]张玉玲, 褚志强, 周赛君, 等. IVIM评估不同尿白蛋白排泄率2型糖尿病患者肾功能损伤的价值[J]. 临床放射学杂志, 2021, 40(10):2004-2009.
Zhang YL, Chu ZQ, Zhou SJ, et al. Evaluation of renal impairment using IVIM in type 2 diabetes mellitus with different urinary albumin excretion rates[J]. J Clin Radiol, 2021, 40(10):2004-2009.
[8] Liu SM, Xu FX, Shen F, et al. Rapid genotyping of-1131T>C polymorphism using high resolution melting analysis with unlabeled probes[J]. Gene, 2012, 498(2):276-279.
[9] Bogari NM, Aljohani A, Amin AA, et al. A genetic variant c.553G > T (rs2075291) in the apolipoprotein A5 gene is associated with altered triglycerides levels in coronary artery disease (CAD) patients with lipid lowering drug[J]. BMC Cardiovasc Disord, 2019, 19(1):2.
[10] 熊哲学, 唐明娟, 李凝旭. 达格列净通过上调SIRT1增强糖尿病肾病大鼠肾脏细胞自噬从而抑制足细胞损伤[J]. 中国病理生理杂志, 2022, 38(4):680-687.
Xiong ZX, Tang MJ, Li NX. Dapagliflozin enhances renal cell autophagy in diabetic kidney disease rats by up-regulating expression of SIRT1, thereby preventing podocyte damage[J]. Chin J Pathophysiol, 2022, 38(4):680-687.
[11] Srinivasan S, Singh P, Kulothungan V, et al. Relationship between triglyceride glucose index, retinopathy and nephropathy in Type 2 diabetes[J]. Endocrinol Diabetes Metab, 2020, 4(1):e00151.
[12] Shahwan MJ, Jairoun AA, Farajallah A, et al. Prevalence of dyslipidemia and factors affecting lipid profile in patients with type 2 diabetes[J]. Diabetes Metab Syndr, 2019, 13(4):2387-2392.
[13] Fiaz M, Shaiq PA, Raj GK, et al. Association study of apolipoprotein A5 gene (gene) variant with the metabolic syndrome in local Pakistani population[J]. J Pak Med Assoc, 2019, 69(3):301-305.
[14] Zafar U, Khaliq S, Lone KP. Genetic association of apolipoprotein A5 -1131T>C polymorphism with traits of metabolic syndrome[J]. J Coll Physicians Surg Pak, 2019, 29(7):626-630.
[15] 徐勤霞, 徐璐扬, 张明, 等. NFATC1基因多态性对肾移植患者慢性排斥反应发生率的影响[J]. 药物流行病学杂志, 2020, 29(6):413-420.
Xu QX, Xu LY, Zhang M, et al. Influence of NFATC1 polymorphisms on the incidence of chronic rejection in renal transplant patients[J]. Chin J Pharmacoepidemiol, 2020, 29(6):413-420.
[16] Mahrooz A, Zargari M, Ansari V, et al. Association ofgene promoter region -1131T>C polymorphism (rs662799) to plasma triglyceride level in patients with type 2 diabetic nephropathy[J]. J Clin Diagn Res, 2016, 10(5):BC09-BC13.
[17] 余晓, 戴华玉, 王业忠, 等. 遵义汉族载脂蛋白A5(c.553G/T)基因多态性与高甘油三酯血症[J]. 实用医学杂志, 2016, 32(20):3386-3390.
Yu X, Dai HY, Wang YZ, et al. Apolipoprotein A5 (c.553G/T) gene polymorphism and hypertriglyceridemia in Zunyi Han nationality[J]. J Pract Med, 2016, 32(20):3386-3390.
[18] 肖懿慧, 舒娟, 袁祖贻, 等. 陕西地区心血管疾病患者基因多态性分布及其与血脂水平和冠心病类型的相关性[J]. 西安交通大学学报(医学版), 2021, 42(3):398-401.
Xiao YH, Shu J, Yuan ZY, et al. Distribution ofpolymorphism and its correlation with blood lipid level and type of coronary heart disease in Shaanxi[J]. J Xi'an Jiaotong Univ (Med Sci), 2021, 42(3):398-401.
[19] 冯佳, 齐婷, 王述进, 等.基因多态性与2型糖尿病血管病变的相关性研究[J]. 中西医结合心脑血管病杂志, 2020, 18(18):3077-3079.
Feng J, Qi T, Wang SJ, et al. Association betweengene polymorphism and angiopathy in type 2 diabetes mellitus[J]. Chin J Integr Med Cardiocerebrovasc Dis, 2020, 18(18):3077-3079.
[20] Chiou KR, Chen CY, Charng MJ. Genetic diagnosis via whole exome sequencing in Taiwanese patients with hypertriglyceridemia[J]. J Atheroscler Thromb, 2015, 22(9):887-900.
[21] 俞刚, 陆峰泉, 沈静, 等. 2型糖尿病肾病患者血清同型半胱氨酸、叶酸和亚甲基四氢叶酸还原酶基因多态性的关系[J]. 中华核医学与分子影像杂志, 2021, 41(3):145-148.
Yu G, Lu FQ, Shen J, et al. Relationship of serum homocysteine, folic acid and genetic polymorphism of methyltetrahydrofolate reductase in patients with type 2 diabetic nephropathy[J]. Chin J Nucl Med Mol Imaging, 2021, 41(3):145-148.
Relationships betweengene polymorphism and susceptibility to T2DM and renal damage in Han Chinese population
HONG Juan, SU Gang△, XUAN Xiao-ming, WU Shui-mei
(,,241000,)
To investigate the relationship between apolipoprotein A5 () gene polymorphism and susceptibility to type 2 diabetes mellitus (T2DM) and renal damage in Han Chinese population.A total of 189 Han patients with T2DM (T2DM group) and 189 healthy controls (control group) were selected according to the principle of random pairing. In addition, according to the renal examination, the patients in T2DM group were further divided into renal damage group and without renal damage group. The-1131T>C and c.553G>T genotypes of tested objects were detected by polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP), and allelic frequencies were counted. The relationship betweengene polymorphism and T2DM susceptibility/renal damage in Han Chinese population was evaluated by logistic regression analysis.The proportions of TC genotype at -1131T>C locus and GT genotype at c.553G>T locus ofgene in T2DM group were significantly higher than those in control group, and the frequencies of allele C at -1131T>C locus and allele T at c.553G>T locus in T2DM group were significantly higher than those in control group (<0.05). The proportions of TC genotype at -1131T>C locus and GT genotype at c.553G>T locus ofgene in T2DM patients with renal damage were significantly higher than those in T2DM patients without renal damage, and the frequencies of allele C at -1131T>C locus and allele T at c.553G>T locus in T2DM patients with renal damage were significantly higher than those in T2DM patients without renal damage (<0.05). Logistic regression analysis showed that TC genotype and allele C at -1131T>C locus and GT genotype and allele T at c.553G>T locus increased the risk of T2DM [odds ratios (OR) were 3.575, 2.782, 4.063 and 3.995, respectively;<0.05] and renal damage (OR were 2.807, 2.347, 2.977 and 2.954, respectively;<0.05).The-1131T>C and c.553G>T gene polymorphisms are associated with the susceptibility to T2DM and renal damage in Han Chinese population, and the risks of T2DM and renal damage are higher in carriers of TC genotype and allele C of -1131T>C locus and GT genotype and allele T of c.553G>T locus.
Apolipoprotein A5; Gene polymorphism; Type 2 diabetes mellitus; Renal damage
1000-4718(2022)09-1653-06
2022-04-23
2022-08-05
13505530139; E-mail: hongjuan8704@163.com
R587.1; R394.3
A
10.3969/j.issn.1000-4718.2022.09.015
[基金项目]芜湖市卫生健康委员会科研和技术项目(No. 2019WWKJ01)
(责任编辑:林白霜,罗森)