复方甘草酸苷片配合米诺地尔酊治疗斑秃的效果及对血清细胞因子 Anti-TPOAb和Anti-TGAb水平的影响
2021-01-16杨今言杨敏陈赵慧卢娟李丽华
杨今言 杨 敏 陈赵慧 卢 娟 李丽华




[關键词]斑秃;复方甘草酸片;米诺地尔酊;甲状腺自身抗体;甲状腺激素;毛发镜
[中图分类号]R758.71 [文献标志码]A [文章编号]1008-6455(2021)12-0093-05
Effect of Compound Glycyrrhizin Tablets Combined with Minoxidil Tincture in the Treatment of Alopecia Areata and the Influence on Serum Levels of Anti-TPOAb and Anti-TGAb
YANG Jin-yan,YANG Min,CHEN Zhao-hui,LU Juan,LI Li-hua
(Department of Dermatology,the Second Affiliated Hospital of Xinjiang Medical University,Urumqi 830064,Xinjiang,China)
Abstract: Objective To investigate the clinical value of compound glycyrrhizin tablets combined with minoxidil tincture in the treatment of alopecia areata and the influence on levels of thyroid autoantibodies. Methods Eighty-nine patients with alopecia areata were selected and divided into the control group (44 cases) and the observation group (45 cases). All subjects were treated with external application of minoxidil tincture, and patients in observation group were additionally treated with compound glycyrrhizin tablets for 12 weeks. Therapeutic effects of the two groups were compared, and trichoscopy was performed before treatment and after treatment. The follicle density, hair density and vellus hair rate were determined. Blood samples were collected to detect changes in levels of peripheral blood interleukin-10 (IL-10), interferon-γ (IFN-γ), transforming growth factor-β (TGF-β), substance P (SP), thyroid autoantibodies [anti-thyroglobulin antibody (Anti-TGAb), anti-thyroid peroxidase antibody (Anti-TPOAb)], thyroid hormones [thyroid stimulating hormone (TSH), free triiodothyronine (FT3), free thyroxine (FT4)]. The occurrence of adverse reactions and recurrence during 6 months of follow-up were statistically analyzed. Results The curative effect of the observation group was better than that of the control group (95.56% vs 86.36%), the difference was statistically significant (P<0.05). After 12 weeks of treatment, the hair follicle density and hair density in the observation group were higher than those in the control group [(92.25±10.14)cm2,(129.52±10.96)cm2 vs (86.52±7.98)cm2,(123.35±11.75)cm2], and the hairiness rate was lower than that in the control group [(8.25±2.14)% vs (11.36±3.33)%], the differences were statistically significant (P<0.05). After 12 weeks of treatment, IL-10 and TGF-β in the observation group higher than the control group [(89.52±10.55)pg/ml, (53.52±7.25)ng/ml vs (84.75±8.51)pg/ml, (50.63±5.44)ng/ml], IFN-γ and SP was lower than those in the control group [(28.41±5.15)ng/L, (10.52±3.06)pg/ml vs (33.65±6.98)ng/L, (13.25±4.17)pg/ml], the differences were statistically significant (P<0.05). There was no significant difference in the positive rate of Anti-TGAb and the levels of TSH, FT3 and FT4 between the two groups before and after treatment (P>0.05). After 12 weeks of treatment, the positive rate of Anti-TPOAb in the observation group decreased, which was statistically significant compared with that in the same group before treatment (P<0.05), and there was no significant difference compared with that in the control group after treatment (P>0.05). There was no significant difference in the incidence of adverse reactions between the two groups (P>0.05). The recurrence rate of alopecia areata in the observation group (6.67%) was lower than that in the control group (22.73%, P<0.05). Conclusion Compound glycyrrhizin tablets combined with minoxidil tincture is superior to minoxidil tincture alone in the treatment of alopecia areata. The former can reduce inflammatory response, regulate immune balance and the expression of thyroid autoantibodies, and reduce the recurrence of alopecia areata. Besides, it is safe and effective.
Key words: alopecia areata; compound glycyrrhizic acid tablets; minoxidil tincture; thyroid autoantibodies; thyroid hormones; trichoscopy
斑秃属非瘢痕型、炎性脱发,是以圆形脱发、圆秃为特点的皮肤附属器疾病,各年龄均可发病,青壮年及儿童常见,影响外观及社交[1]。斑秃病因尚未完全阐明,多认为精神高度紧张、心理创伤、压力过大、内分泌代谢障碍、微量元素缺乏、高自身抗体水平及免疫紊乱等均与其发病有关[2]。以往多采用糖皮质激素类药物局部干预,但重度斑秃应用大剂量糖皮质激素毒副反应多,耐受性差[3]。米诺地尔酊最早用于控制重度高血压,有强效扩血管作用。后续发现该药物应用过程中患者可出现不同程度多毛症,后逐渐批准于雄激素性脱发及斑秃治疗[4]。复方甘草酸苷片系以甘草苷酸、半胱氨酸、甘氨酸等为主要成分的复方制剂,有较强免疫调节、抗炎、抗变态反应作用,存在与类固醇激素相似作用,但无激素类药物相关不良反应,已证实对皮肤科炎症疾病控制效果良好[5]。最新报道认为对斑秃患者在米诺地尔酊外用治疗的基础上加用复方甘草酸苷存在增益效果[6]。但两者联合对甲状腺自身抗体的影响及机制尚未阐明。为探讨两者联合治疗斑秃的可行性,研究其对甲状腺自身抗体的影响及其作用机制,现对收治的89例斑秃患者展开随机对照研究,报道如下。
1 资料和方法
1.1 一般资料:选择2017年2月-2019年10月医院收治的斑秃患者89例。纳入标准:满足斑秃诊断标准[7],突发或短期内单处或多处头发呈圆形或片状脱落,脱发区皮肤正常,未见瘢痕或萎缩,无自觉症状;无自身免疫性疾病;皮肤镜下未见新生毳毛;入组前4周未接受其他如糖皮质激素等治疗;履行告知义务,家属或患者已签署知情同意书;本辖区常住居民,经评估可完成近期规律复诊。排除标准:瘢痕型脱发;先天性秃发、梅毒性秃发、头藓或拔毛癖者;严重心肝肾肺功能不全;严重脑血管疾病;局部细菌感染;孕妇或哺乳期女性;对已知药物成分过敏;接受植发治疗者;经评估无法完成随诊者。
按就诊编号奇偶数分为对照组与观察组,分别为44例与45例。两组性别、年龄、病程、脱发直径、斑秃分度[8]等资料比较差异无统计学意义(P>0.05),见表1。研究通过医院伦理委员会审批。
1.2 方法:两组均予5%米诺地尔酊(浙江万晟药业有限公司,国药准字H20010714)局部外用治疗,每次1ml(约7喷),直接喷于脱发局部,自患处中心向外涂抹,指腹轻柔按摩约3~5min,2次/天。使用前保持头皮、头发干燥。观察组在此基础上加用复方甘草酸苷片[卫材(中国)药业有限公司,国药准字J20130077,25毫克/片]治疗,成人50~75毫克/次,儿童25毫克/次,3次/天,饭后口服,依据症状适当增减,2周后减量至25~75mg/d,两组均治疗12周。治疗期间禁食刺激性食物,均衡、清淡饮食,戒烟戒酒,保持睡眠充足,避免过度劳累,规律作息,并予防脱发宣教,保持积极、乐观的心态。
1.3 观察指标:①毛发镜检查:治疗前、治疗12周后进行CBS-1600型毛发镜(中国台湾AnMo Electronics公司)检查,观察斑秃改善情况,标准毛发镜拍摄模式,校准软件自动测量结果,记录毛囊密度(70倍视野下毛干总数/总视野面积)、毛发密度(70倍下毛囊總数/总视野面积)及毳毛率(70倍视野下毛漩毳毛数目/毛发总数);②细胞因子测定:治疗前、治疗12周后采集外周肘静脉血,采用酶联免疫吸附试验法测定外周血白介素-10(Interleukin-10,IL-10)、干扰素-γ(Interferon-γ,IFN-γ)、转化生长因子-β(Transforming growth factor-β,TGF-β)、P物质(Substance P,SP)水平,试剂盒购自武汉Elabscience Biotechnology Co.,Ltd,试验检测过程严格按试剂说明进行;③甲状腺自身抗体及激素测定:治疗前、治疗12周后采血测定甲状腺自身抗体及甲状腺激素水平。包括抗甲状腺球蛋白抗体(Anti-thyroglobulin antibody,Anti-TGAb)、抗甲状腺过氧化酶抗体(Anti-thyroid peroxidase antibody,Anti-TPOAb)、促甲状腺素(Thyroid stimulating hormone,TSH)、游离三碘甲状腺原氨酸(Free triiodothyronine 3,FT3)、游离甲状腺素(Free triiodothyronine 4,FT4),均采用化学发光免疫法测定,TSH、FT3、FT4试剂盒购自美国雅培公司,Anti-TPOAb、Anti-TGAb试剂盒购自武汉博士德生物工程有限公司,均按试剂说明规范操作。甲状腺激素正常值范围:TSH:0.88~2.44mIU/L,FT3:2.63~5.70pmol/L,FT4:9.01~19.05pmol/L;甲状腺自身抗体阳性标准:Anti-TPOAb>40kU/L,Anti-TGAb>110kU/L;④安全性及复发观察:统计两组治疗期间不良反应发生情况;出院后每3个月复诊1次,统计随访6个月斑秃复发率。
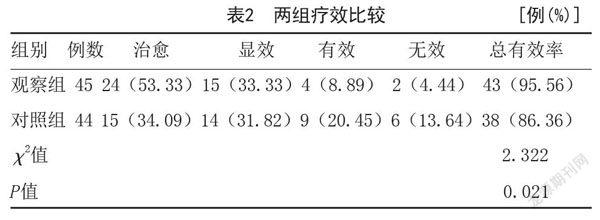
1.4 疗效标准:治疗后12周评估疗效。参照《临床皮肤病学》[9]。治愈:斑秃全区见终毛生长,达美容覆盖要求,与正常毛发相似,拔毛试验阴性;显效:斑秃区大部分均见毳毛生长,停止脱发,终毛覆盖率超过1/2,拔毛试验阴性;好转:斑秃区见毳毛生长,停止脱发,终毛覆盖率不超过1/2;无效:未达上述标准或有斑秃有加重。总有效率=(治愈+显效+好转)例数/总例数×100%。
1.5 统计学分析:利用SPSS 24.0统计学软件处理数据,计数资料构成比(%)描述,行χ2检验或Fisher确切概率分析;计量资料行正态性与方差齐性检验,满足要求采用(x¯±s)描述,组间比较采用t检验。P<0.05表示差异有统计学意义。
2 结果
2.1 两组疗效比较:观察组疗效优于对照组,差异有统计学意义(P<0.05),见表2。
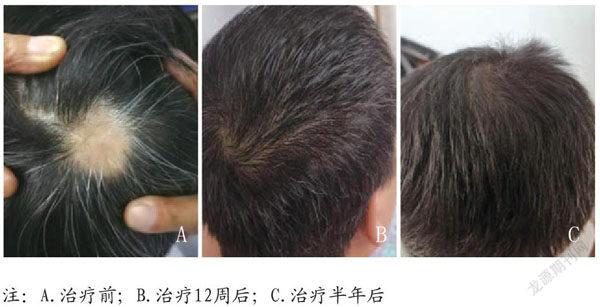
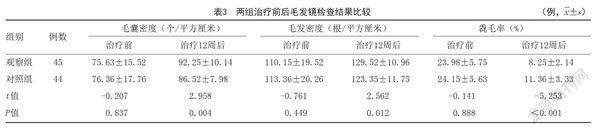
2.2 两组治疗前后毛发镜检查结果比较:治疗前,两组毛囊密度、毛发密度、毳毛率比较差异无统计学意义(P>0.05);治疗12周后,两组毛囊密度、毛发密度上升,毳毛率下降,差异有统计学意义(P<0.05);且观察组毛囊密度、毛发密度高于对照组,毳毛率低于对照组,差异有统计学意义(P<0.05)。见表3。两组典型病例见图1~2。
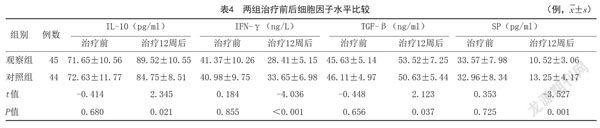
2.3 两组治疗前后细胞因子水平比较:治疗前,两组IL-10、IFN-γ、TGF-β、SP水平比较差异无统计学意义(P>0.05);治疗12周后,两组IL-10、TGF-β上升,IFN-γ、SP降低,差异有统计学意义(P<0.05);且观察组IL-10、TGF-β高于对照组,IFN-γ、SP低于对照组,差异有统计学意义(P<0.05)。见表4。
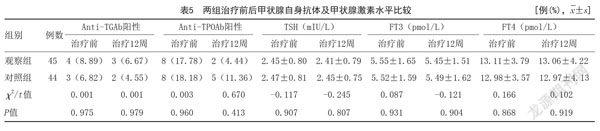
2.4 两组治疗前后甲状腺自身抗体及甲状腺激素水平比较:两组治疗前后Anti-TGAb阳性率及TSH、FT3、FT4水平比较差异无统计学意义(P>0.05);治疗12周后,观察组Anti-TPOAb阳性率降低,与同组治疗前比较差异有统计学意义(χ2=4.050,P=0.044<0.05),略低于对照组治疗后,但组间比较差异无统计学意义(P>0.05)。见表5。
2.5 两组治疗不良反应发生率及随访6个月复发率比较:两组治疗不良反应发生率比较差异无统计学意义(P>0.05);观察组随访6个月斑秃复发率低于对照组,差异有统计学意义(P<0.05)。见表6。
3 讨论
普遍认为斑秃与遗传、神经内分泌及环境因素有关,多将其归于自身免疫性疾病范畴[10]。以往常使用血管舒张药物治疗斑秃,以促进皮损处毛细血管扩张,刺激毛发生长[11]。米诺地尔酊存在上述类似血管扩张功效,早期试验发现可引起多毛现象[12]。动物研究证实,米诺地尔酊该药主要成分可促进毛发生长[13]。本研究发现,5%米诺地尔酊局部外用后对照组斑秃患者毛囊密度、毛发密度均上升,毳毛率下降,支撑以上试验结果,推测米诺地尔酊对治疗斑秃有肯定的效果。分析机制可能为:米诺地尔酊可直接刺激毛囊上皮细胞增殖及分化;且存在血管舒张作用,可改善局部血供,促进毛囊由休止期向生长期转化,增加毛乳头血流量,促进毛发生长。但本研究发现,单独应用米诺地尔酊的对照组患者整体效果不及加用复方甘草酸苷片的观察组,对照组毛囊密度、毛发密度较观察组低,毳毛率较观察组高,推测在此基础上加用复方甘草酸苷存在增益效果,更能改善斑秃病情,促进毛发生长,这与盛宏等[14]研究结论相似。复方甘草酸苷主要成分为β-甘草酸、甘氨酸及半胱氨酸等,甘草酸苷经口服后在体内可分解为甘草次酸,具有强效、抗炎抗补体及抗免疫活性,同时可拮抗机体变态反应,存在近似类固醇激素作用,与肝脏类固醇代谢酶还原酶亲和力强,可促进醛固酮灭活,但无激素类副作用。研究证实,β-甘草酸存在调控机体免疫功效,可强化巨噬细胞吞噬活性,促进胸腺外T细胞分化,抑制白三烯、肥大细胞颗粒等炎症释放[15]。本研究结果亦显示,观察组治疗12周炎症因子IFN-γ、SP水平下降,生长刺激因子TGF-β及抑炎因子IL-10均上升,较对照组更明显,提示加用复方甘草酸苷片抗炎作用更显著,推测加用复方甘草酸苷强化斑秃疗效的机制可能为:外用米诺地尔酊可刺激毛囊上皮細胞增殖、分化,促血管生成,提升毛囊密度、毛发密度;在此基础上加用复方甘草酸苷发挥抗炎、抗过敏及免疫调节作用,平衡辅助性T细胞功能,抑制自身免疫反应,控制激素样皮炎及刺激性皮炎,减轻斑秃局部炎症反应,进一步改善病情。
近期也有观点表示,斑秃可能与自身免疫性甲状腺疾病共病[16]。何迅[17]发现斑秃,尤其重型斑秃患者Anti-TPOAb阳性率较正常人高。本研究发现,治疗前,两组Anti-TGAb与上述报道内正常对照接近,而Anti-TPOAb阳性率略高,提示斑秃可能与自身免疫性甲状腺疾病相关。考虑自身免疫性甲状腺功能减退对机体代谢产生影响,从静止期毛发增多转变为生长期毛发生长速度减缓,甚至无法转化,导致脱发。但并非所有斑秃患者均出现抗甲状腺自身抗体改变,可能存在人群、种族及地区差异[18]。但对斑秃与自身免疫性甲状腺疾病共病的关系仍需引起关注。而对于斑秃与甲状腺功能之间的关系,本研究尚未发现斑秃治疗前后TSH、FT3、FT4有明显改变,同时治疗前后上述因子水平均处于正常范围内,考虑Anti-TPOAb作为反映甲状腺功能的标志性抗体,其改变多发生于甲状腺功能受损前,此时甲状腺功能可能并未出现明显受损,故甲状腺激素变化不明显。本研究还发现,治疗12周后,两组Anti-TPOAb阳性率略有下降,观察组略低于对照组,提示加用复方甘草酸苷片可通过调控机体免疫,预防甲状腺功能受损。但组间数据比较未呈现统计学差异,可能与样本量较少及观察时间较短有关,后续需扩充样本量进一步论证。此外,本研究发现,两组不良反应发生率接近,提示加用复方甘草酸苷片安全有效。同时随访6个月,观察组斑秃复发率较对照组低,支撑万慧颖等[19]结论,证实联合用药可进一步巩固疗效,提高斑秃控制效果,避免其反复发作,近期作用肯定。
综上,对斑秃患者建议采用复方甘草酸苷片联合米诺地尔酊外用治疗,较单独应用米诺地尔酊疗效更高,更能减轻机体炎症反应,调节甲状腺自身抗体水平,促进毛囊及毛发生长,改善脱发症状,且安全性高,近期复发率低。但本研究样本量少、观察时间短,对联合治疗的远期价值及甲状腺自身抗体在斑秃发病中的确切机制尚有待进一步研究论证。
[参考文献]
[1]Strazzulla LC,Wang EHC,Avila L,et al.Alopecia areata: Disease characteristics, clinical evaluation, and new perspectives on pathogenesis[J].J Am Acad Dermatol,2018,78(1):1-12.
[2]Salem SA,Asaad MK,Elsayed SB,et al.Evaluation of macrophage migration inhibitory factor (MIF) levels in serum and lesional skin of patients with alopecia areata[J].Int J Dermatol,2016,55(12):1357-1361.
[3]Phan K,Ramachandran V,Sebaratnam DF.Methotrexate for alopecia areata: A systematic review and meta-analysis[J].J Am Acad Dermatol,2019,80(1):120-127.
[4]吴桥芳,范卫新.米诺地尔治疗雄激素性秃发的机制和剂型研究进展[J].临床皮肤科杂志,2018,47(2):128-131.
[5]曾熙,胡鹏飞.益肾生发丸联合复方甘草酸苷胶囊治疗斑秃的临床研究[J].现代药物与临床,2019,34(5):1449-1453.
[6]梁占捧,李敬,李舒,等.复方甘草酸苷片联合米诺地尔液治疗斑秃34例临床分析[J].中华实用诊断与治疗杂志,2018,32(12):1216-1218.
[7]中华医学会皮肤性病学分会毛发学组.中国斑秃诊疗指南(2019)[J].临床皮肤科杂志,2020,49(2):69-72.
[8]Olsen EA,Canfield D.SALT Ⅱ: A new take on the Severity of Alopecia Tool (SALT) for determining percentage scalp hair loss[J].J Am Acad Dermatol,2016,75(6):1268-1270.
[9]Carol Soutor,MariaK Hordinsky.临床皮肤病学[M].北京:北京大学医学出版社,2014:32.
[10]谭欢,兰雪梅,杨希川.皮肤科医师关于斑秃治疗的问卷调查[J].临床皮肤科杂志,2017,46(10):682-686.
[11]Bayart CB,Deniro KL,Brichta L,et al.Topical janus kinase inhibitors for the treatment of pediatric alopecia areata[J].J Am Acad Dermatol,2017,77(1):167-170.
[12]吴晓瑜,许敏鸿.外用米诺地尔溶液致儿童多毛症一例[J].中华皮肤科杂志,2018,51(2):154.
[13]邢飞.米诺地尔外用对化疗后脱发小鼠血和毛囊局部粘附分子ICAM-1和ELAM-1的影响[D].武汉:华中科技大学,2011.
[14]盛宏,潘龙,王建华.脉管复康片联合复方甘草酸苷和米诺地尔外用治疗斑秃疗效观察[J].中国中西医结合皮肤性病学杂志,2016,15(4):236-237.
[15]刘莉,韩刚.不同构型的甘草酸对葛根素在大鼠體内的药代动力学影响[J].中国临床药理学杂志,2019,35(19):2377-2380.
[16]杨莹,徐艳艳,陈晓红,等.斑秃患者血清中甲状腺自身抗体、促甲状腺素及甲状腺激素水平的测定与分析[J].临床皮肤科杂志,2018,47(3):145-149.
[17]何迅.斑秃患者甲状腺激素水平及甲状腺自身抗体的测定及分析[J].临床皮肤科杂志,2017,46(2):107-109.
[18]彭雅雯,雷铁池.关于斑秃治疗的新进展[J].医学综述,2020,26(5):
940-944.
[19]万慧颖,周敏,刘杨英.白芍总苷联合复方甘草酸苷对斑秃患者血清IL-17A、IL-17F和TGF-β1的影响[J].四川医学,2017,38(10):1198-1201.
[收稿日期]2020-07-28
本文引用格式:杨今言,杨敏,陈赵慧,等.复方甘草酸苷片配合米诺地尔酊治疗斑秃的效果及对血清细胞因子Anti-TPOAb和Anti-TGAb水平的影响[J].中国美容医学,2021,30(12):93-97.
