阿霉素脂质体与传统制剂治疗晚期乳腺癌效果及毒性的meta分析
2017-11-07罗英豪王思雄
冯 佳 罗英豪 王思雄
(宜宾市第二人民医院乳腺甲状腺科,四川 宜宾 644000)
1 重庆市肿瘤研究所/医院、癌症中心
阿霉素脂质体与传统制剂治疗晚期乳腺癌效果及毒性的meta分析
冯 佳 罗英豪1王思雄1
(宜宾市第二人民医院乳腺甲状腺科,四川 宜宾 644000)
目的比较阿霉素脂质体与阿霉素传统制剂治疗晚期乳腺癌时效果和毒性。方法搜索Pubmed数据库截止2015年5月发表的关于阿霉素脂质体化疗对比阿霉素传统制剂治疗晚期乳腺癌效果和毒性的文章并按照纳入排除标准进行筛选。采用Cochrane协作网推荐的RevMan5.3软件进行Meta分析。结果纳入10篇随机对照研究的2 889例乳腺癌患者,经过分析发现相比传统阿霉素治疗,阿霉素脂质体化疗可以显著降低心脏毒性的风险(OR=0.46,95%CI0.23~0.92,P=0.03),并且显著提高总缓解率(ORR)(OR=1.25,95%CI1.02~1.52,P=0.03)。阿霉素脂质体化疗并不能提高患者无进展生存(PFS)率(HR=1.14,95%CI0.96~1.34,P=0.12)。对总生存(OS)率分析发现两种治疗方案无统计学差异(HR=1.00,95%CI0.91~1.10,P=0.93)。结论相比传统阿霉素剂型,使用阿霉素脂质体治疗可以显著提高晚期乳腺癌患者ORR及降低心脏毒性,应为临床首选。
阿霉素;脂质体;化疗;乳腺癌;Meta分析
乳腺癌死亡率仅次于肺癌,位居全球第二〔1〕。目前包括复发和转移性乳腺癌在内的晚期乳腺癌仍然是无法治愈的,现有的治疗目标是减轻症状、延缓癌症进展、延长患者生存时间。蒽环霉素是一种对早期和晚期乳腺癌都有效的药物〔2〕。然而,由于累积剂量的原因,传统蒽环类药物的潜在效益被其心脏毒性所限制〔3~5〕。随后,阿霉素脂质体药物被开发出来在保留其抗肿瘤活性的同时降低了其心脏毒性的副作用〔6〕。多项研究结果显示:在治疗其他已使用过蒽环类药物或转移能力未成熟的乳腺癌患者时,阿霉素脂质体单独使用或联合其他抗癌药物都有不错的疗效〔7~9〕。还有一些研究证实相比传统蒽环类药物,阿霉素脂质体在治疗乳腺癌时不仅降低了其心脏毒性,而且具有和传统药物相似的抗肿瘤疗效〔10,11〕。也有研究显示阿霉素脂质体与非蒽环类药物合并治疗乳腺癌时并未增加心脏毒性〔12〕。然而有报道指出阿霉素脂质体相比传统蒽环类药物,其具有同样的心脏毒性,但其抗肿瘤效果更好〔13〕。本研究荟萃分析阿霉素脂质体与传统制剂治疗晚期乳腺癌的心脏毒性、治疗应答、无进展生存(PFS)率及总生存(OS)率。
1 材料与方法
1.1检索策略 检索数据库包括Pubmed、中国知网期刊数据库、维普中文期刊数据库。检索的英文关键词包括:“doxorubicin”、“Liposomal”、“breast tumor”和“mammary carcinoma”。检索的中文关键词包括:“阿霉素”、“阿霉素脂质体”、“阿霉素传统制剂”及“乳腺癌”。关键词以逻辑“与”和“或”的方式进行组合检索。按照荟萃分析推荐检索项目(PRISMA)的规定进行文献筛选。见图1。
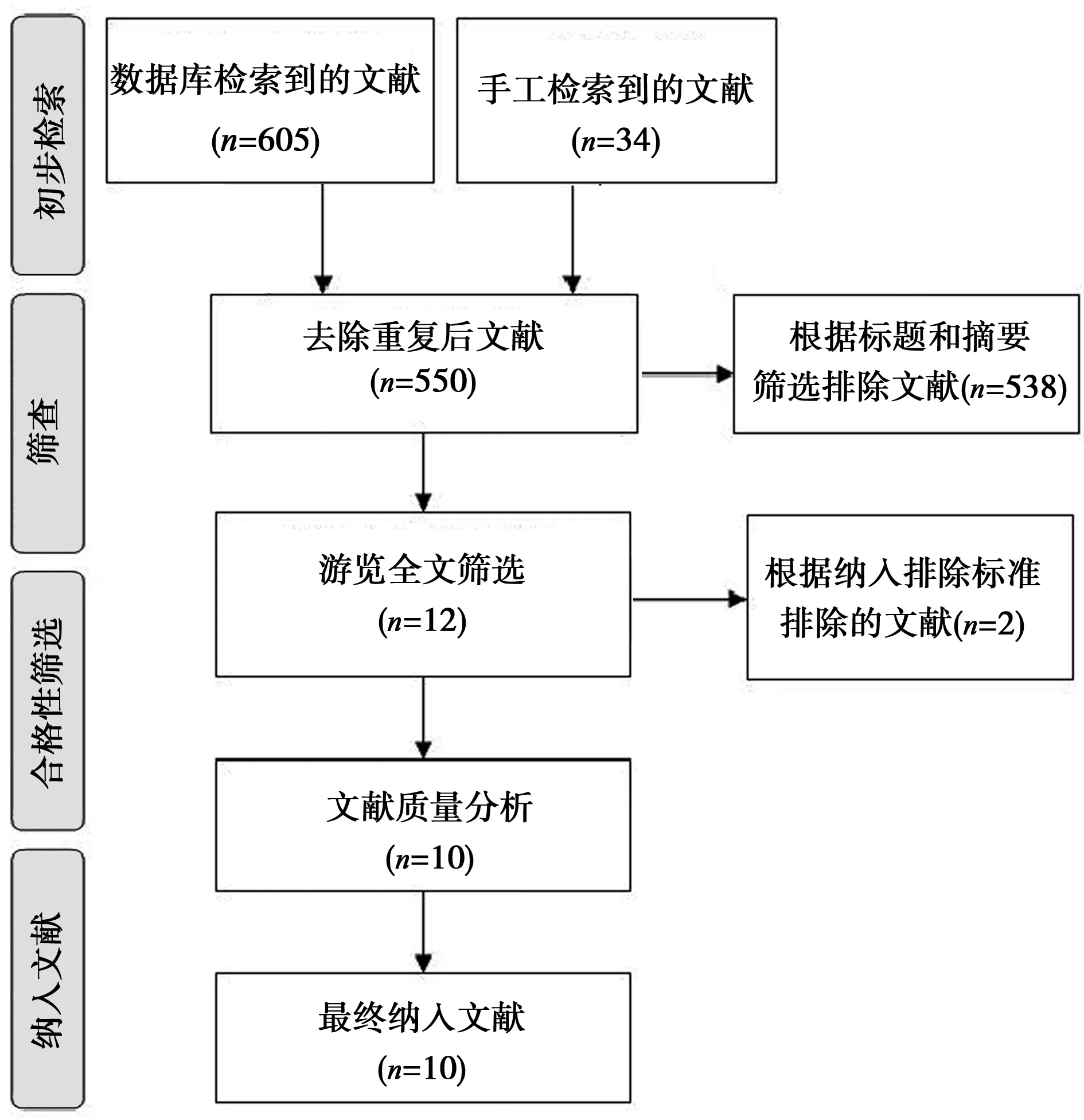
图1 文献筛选流程(DAB,×400)
1.2数据提取 两名研究者根据预先制定的数据收集表进行,所提取的数据包括:第一作者、发表年份、临床试验类型、治疗阶段、样本量和包括心脏毒性在内的主要副反应及总缓解率(ORR)、OS和PFS。某些数据原始文献的文字描述和表格中未给出,已通过对结果图的分析中获得。同时还尝试联系文字的作者以获得更为准确的数据。数据提取产生分歧时,第三位研究者将加入共同讨论确定。使用Jadad量表进行评分,从文献来源、受试者选择、数据可比性进行质量评价〔14〕。
1.3统计学方法 采用RevMan 5.3软件进行χ2、I2检验评估文献异质性。使用逆方差法对HR值进行分析。根据Parmar等〔15〕报道的方法从生存曲线中提取HR值。当I2≤25%时为低度异质性,>25%且≤50%为重度异质性,>50%则为高度异质性。因此,当I2<50%时使用固定效应模型进行数据合并,否则使用随机效应模型。
2 结 果
2.1文献检索结果及质量评价 见图1和表1。
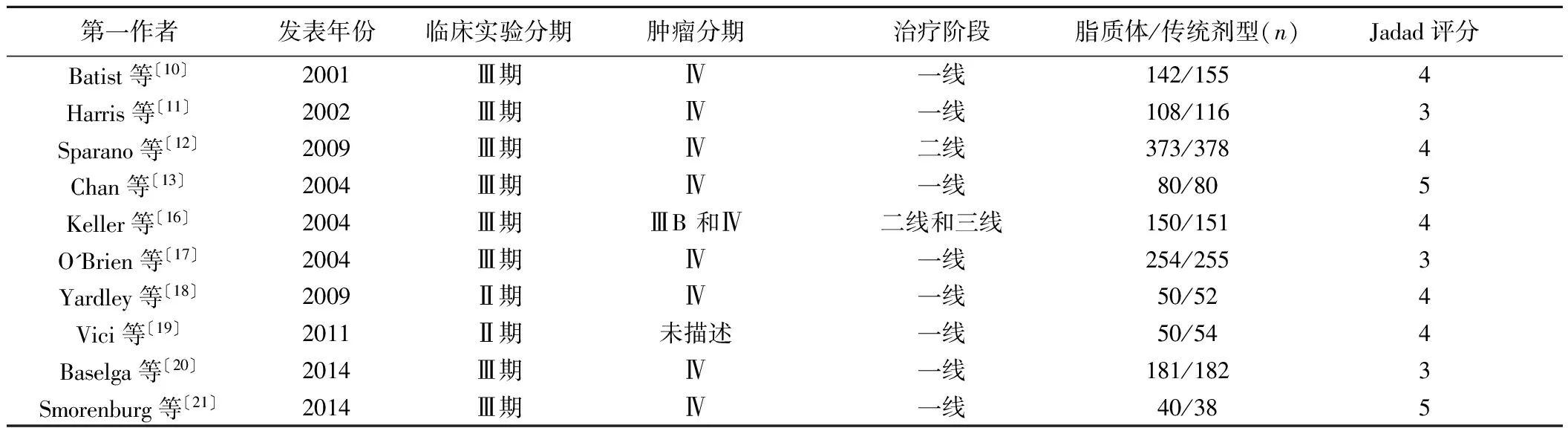
表1 纳入文献的质量评价
2.2心脏毒性的比较 6篇〔10~13,17,19〕关于两种阿霉素制剂治疗后的乳腺癌患者心脏毒性发生率的随机对照研究,P=0.002;I2=74%,相比阿霉素传统制剂,阿霉素脂质体在治疗晚期乳腺癌患者时能明显降低心脏毒性(OR=0.46,95%CI0.23~0.92;P=0.03),见图2。
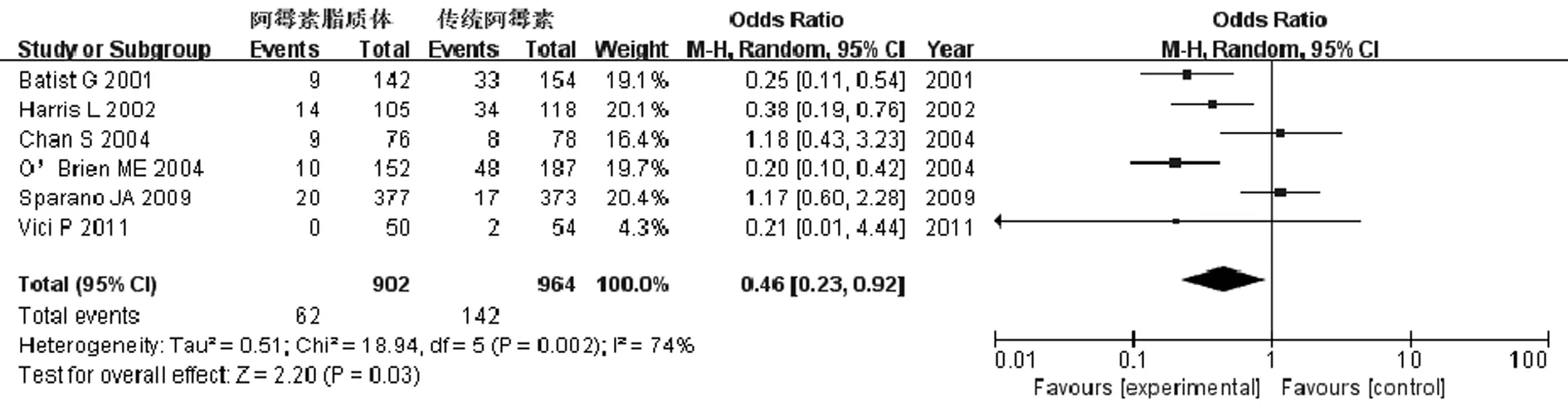
图2 乳腺癌患者心脏毒性发生率的比较
2.3治疗应答的比较 7篇〔10,11,13,16,18,19,21〕关于两种阿霉素制剂治疗后的患者ORR的随机对照研究,P=0.50;I2=0%,相比阿霉素传统制剂,阿霉素脂质体治疗晚期乳腺癌患者时能明显提高ORR(OR=1.25,95%CI1.02~1.52;P=0.03),见图3。
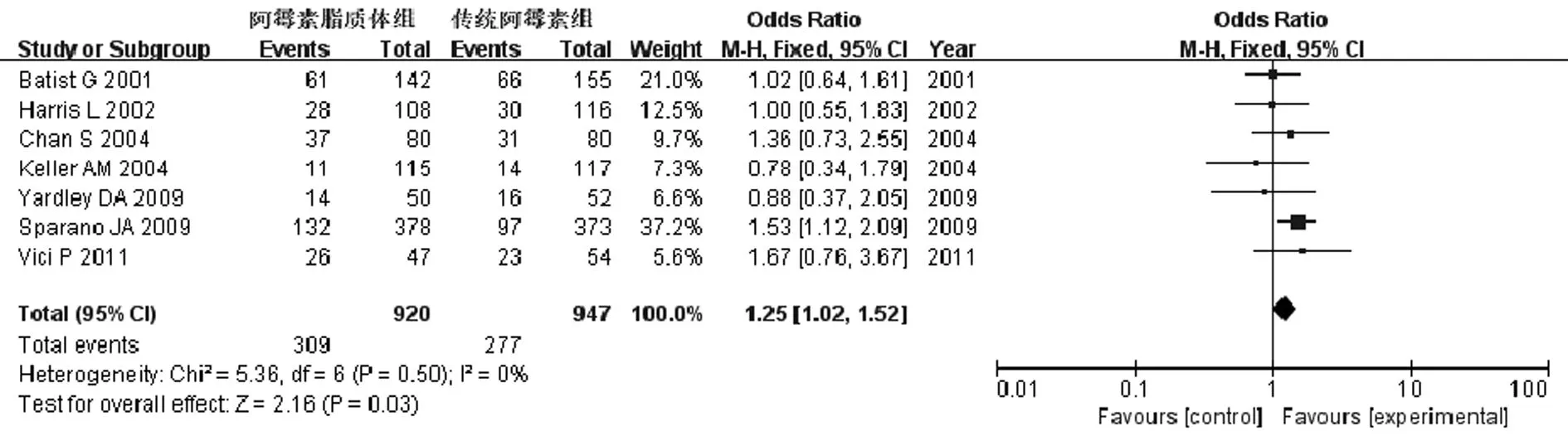
图3 乳腺癌患者ORR的比较
2.4PFS率的比较 8篇〔10~13,16,17,20,21〕关于两种阿霉素制剂
治疗后的患者PFS率的随机对照研究:P=0.002;I2=69%,阿霉素传统制剂和脂质体治疗晚期乳腺癌患者PFS率没有统计学差异(OR=1.14,95%CI0.96~1.34;P=0.12),见图4。
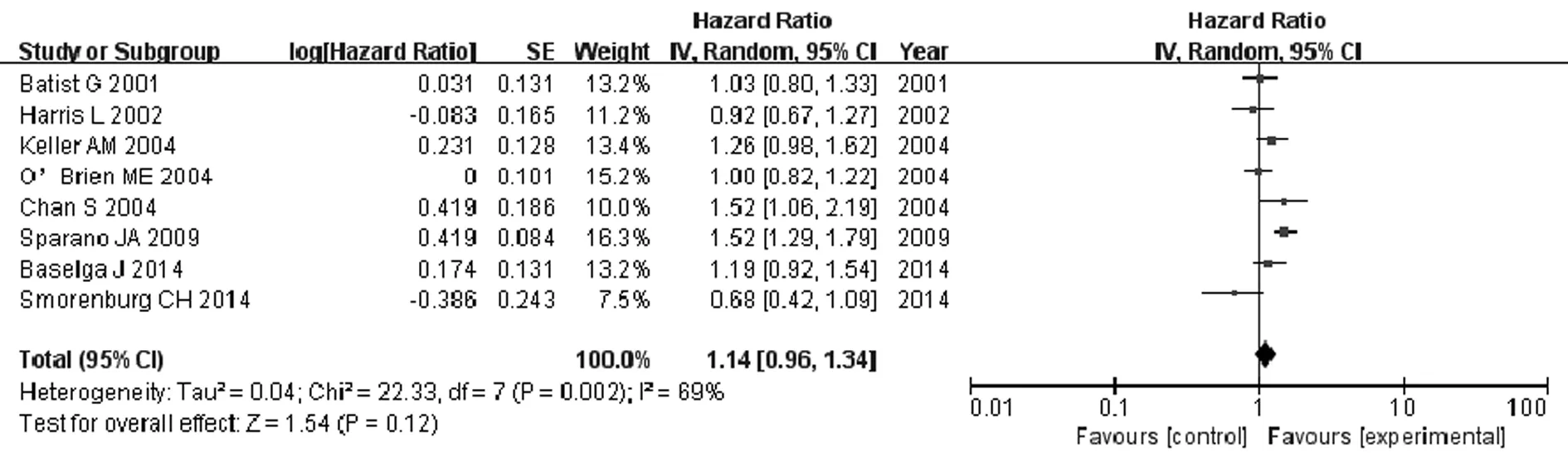
图4 乳腺癌患者PFS率的比较
2.5OS率的比较 8篇〔10~13,16,17,20,21〕关于两种阿霉素制剂治疗后的患者OS率的随机对照研究,P=0.37;I2=7%,阿霉素传统制剂和脂质体治疗晚期乳腺癌患者OS率无统计学差异(OR=1.00,95%CI0.91~1.10;P=0.93),见图5。
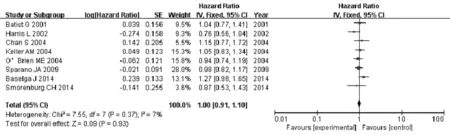
图5 乳腺癌患者OS率的比较
2.6发表性偏倚 全部漏斗图的图形呈对称,说明纳入文献的发表性偏倚较小,见图6。

图6 阿霉素脂质体和传统制剂治疗乳腺癌发表性偏倚漏斗图
3 讨 论
化疗是乳腺癌晚期病人主要的治疗方式。由于晚期乳腺癌是无法通过化疗完全治愈的,因此化疗药物对疾病的控制作用和其产生的副作用之间的平衡考虑就显得尤为重要。
阿霉素是一种传统的蒽环类抗生素,它对于乳腺癌的化疗效果显著〔22〕。然而,阿霉素显著的毒副作用,尤其是心脏毒性限制了其应用于乳腺癌〔23〕。为克服该药物的毒副作用,研究者们开发出了阿霉素脂质体,以期降低阿霉素的毒副作用并保留其抗肿瘤的活性〔6〕。多项动物实验发现同剂量的阿霉素脂质体与传统制剂相比心脏毒性显著降低〔24〕。同时,后续有多项临床研究证明了阿霉素脂质体较高的抗肿瘤活性和较低的心脏毒性〔16,17,25〕。本文结果发现阿霉素脂质体治疗晚期乳腺癌的总应答率显著高于传统制剂。而在PFS方面阿霉素脂质体为主的化疗较传统制剂为主的化疗有优势,但并无统计学差异。这种情况可能是纳入研究的随访时间较短所致。晚期乳腺癌相比其他癌症而言拥有更长的生存期,而且在一线、二线化疗方案失败后患者仍可接受其他综合治疗方式。这种情况可能会对研究结果的OS产生影响。虽然,之前也有一些综述对阿霉素脂质体和传统制剂进行了比较,分析了两者的优缺点。但是由于缺乏严格的文献纳入和排除标准及相应的统计学处理,其说服力有限。
综上,以阿霉素脂质体为主的化疗方案比传统制剂为主的化疗方案对治疗晚期乳腺癌拥有更好的疗效和更低的副反应。
1Ban KA,Godellas CV.Epidemiology of breast cancer〔J〕.Surg Oncol Clin N Am,2014;23(3):409-22.
2Early Breast Cancer Trialists'Collaborative Group(EBCTCG).Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival:an overview of the randomised trials〔J〕.Lancet,2005;365(9472):1687-717.
3Shan K,Lincoff AM,Young JB.Anthracycline-induced cardiotoxicity〔J〕.Ann Intern Med,1996;125(1):47-58.
4Swain SM,Whaley FS,Ewer MS.Congestive heart failure in patients treated with doxorubicin:a retrospective analysis of three trials〔J〕.Cancer,2003;97(11):2869-79.
5Bria E,Cuppone F,Fornier M,etal.Cardiotoxicity and incidence of brain metastases after adjuvant trastuzumab for early breast cancer:the dark side of the moon?A meta-analysis of the randomized trials〔J〕.Breast Cancer Res Treat,2008;109(2):231-9.
6Lao J,Madani J,Puertolas T,etal.Liposomal doxorubicin in the treatment of breast cancer patients:a review〔J〕.J Drug Deliv,2013;2013:456409.
7Schmid P,Krocker J,Kreienberg R,etal.Non-pegylated liposomal doxorubicin and docetaxel in metastatic breast cancer:final results of a phase Ⅱ trial〔J〕.Cancer Chemother Pharmacol,2009;64(2):401-6.
8Rosati MS,Raimondi C,Baciarello G,etal.Weekly combination of non-pegylated liposomal doxorubicin and taxane in first-line breast cancer:wALT trial(phase Ⅰ-Ⅱ)〔J〕.Ann Oncol,2011;22(2):315-20.
9Rochlitz C,Ruhstaller T,Lerch S,etal.Combination of bevacizumab and 2-weekly pegylated liposomal doxorubicin as first-line therapy for locally recurrent or metastatic breast cancer.A multicenter,single-arm phase Ⅱ trial(SAKK 24/06)〔J〕.Ann Oncol,2011;22(1):80-5.
10Batist G,Ramakrishnan G,Rao CS,etal.Reduced cardiotoxicity and preserved antitumor efficacy of liposome-encapsulated doxorubicin and cyclophosphamide compared with conventional doxorubicin and cyclophosphamide in a randomized,multicenter trial of metastatic breast cancer〔J〕.J Clin Oncol,2001;19(5):1444-54.
11Harris L,Batist G,Belt R,etal.Liposome-encapsulated doxorubicin compared with conventional doxorubicin in a randomized multicenter trial as first-line therapy of metastatic breast carcinoma〔J〕.Cancer,2002;94(1):25-36.
12Sparano JA,Makhson AN,Semiglazov VF,etal.Pegylated liposomal doxorubicin plus docetaxel significantly improves time to progression without additive cardiotoxicity compared with docetaxel monotherapy in patients with advanced breast cancer previously treated with neoadjuvant-adjuvant anthracycline therapy:results from a randomized phase Ⅲ study〔J〕.J Clin Oncol,2009;27(27):4522-9.
13Chan S,Davidson N,Juozaityte E,etal.Phase Ⅲ trial of liposomal doxorubicin and cyclophosphamide compared with epirubicin and cyclophosphamide as first-line therapy for metastatic breast cancer〔J〕.Ann Oncol,2004;15(10):1527-34.
14Jadad AR,Moore RA,Carroll D,etal.Assessing the quality of reports of randomized clinical trials:is blinding necessary〔J〕?Control Clin Trials,1996;17(1):1-12.
15Parmar MK,Torri V,Stewart L.Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints〔J〕.Stat Med,1998;17(24):2815-34.
16Keller AM,Mennel RG,Georgoulias VA,etal.Randomized phase Ⅲ trial of pegylated liposomal doxorubicin versus vinorelbine or mitomycin C plus vinblastine in women with taxane-refractory advanced breast cancer〔J〕.J Clin Oncol,2004;22(19):3893-901.
17O'Brien ME,Wigler N,Inbar M,etal.Reduced cardiotoxicity and comparable efficacy in a phase Ⅲ trial of pegylated liposomal doxorubicin HCl(CAELYX/Doxil) versus conventional doxorubicin for first-line treatment of metastatic breast cancer〔J〕.Ann Oncol,2004;15(3):440-9.
18Yardley DA,Burris HR,Spigel DR,etal.A phase Ⅱ randomized crossover study of liposomal doxorubicin versus weekly docetaxel in the first-line treatment of women with metastatic breast cancer〔J〕.Clin Breast Cancer,2009;9(4):247-52.
19Vici P,Colucci G,Giotta F,etal.A multicenter prospective phase Ⅱ randomized trial of epirubicin/vinorelbine versus pegylated liposomal doxorubicin/vinorelbine as first-line treatment in advanced breast cancer.A GOIM study〔J〕.J Exp Clin Cancer Res,2011;30:39.
20Baselga J,Manikhas A,Cortes J,etal.Phase Ⅲ trial of nonpegylated liposomal doxorubicin in combination with trastuzumab and paclitaxel in HER2-positive metastatic breast cancer〔J〕.Ann Oncol,2014;25(3):592-8.
21Smorenburg CH,de Groot SM,van Leeuwen-Stok AE,etal.A randomized phase Ⅲ study comparing pegylated liposomal doxorubicin with capecitabine as first-line chemotherapy in elderly patients with metastatic breast cancer:results of the OMEGA study of the Dutch Breast Cancer Research Group BOOG〔J〕.Ann Oncol,2014;25(3):599-605.
22Levine MN,Whelan T.Adjuvant chemotherapy for breast cancer--30 years later〔J〕.N Engl J Med,2006;355(18):1920-2.
23Minotti G,Menna P,Salvatorelli E,etal.Anthracyclines:molecular advances and pharmacologic developments in antitumor activity and cardiotoxicity〔J〕.Pharmacol Rev,2004;56(2):185-229.
24Kanter PM,Bullard GA,Pilkiewicz FG,etal.Preclinical toxicology study of liposome encapsulated doxorubicin(TLC D-99):comparison with doxorubicin and empty liposomes in mice and dogs〔J〕.In Vivo,1993;7(1):85-95.
25Crivellari D,Gray KP,Dellapasqua S,etal.Adjuvant pegylated liposomal doxorubicin for older women with endocrine nonresponsive breast cancer who are NOT suitable for a “standard chemotherapy regimen”:the CASA randomized trial〔J〕.Breast,2013;22(2):130-7.
王思雄(1973-),男,博士,主治医师,主要从事肿瘤学研究。
冯 佳(1982-),女,主治医师,主要从事乳腺疾病研究。
R737.9
A
1005-9202(2017)20-5074-04;
10.3969/j.issn.1005-9202.2017.20.054
〔2016-07-11修回〕
(编辑 苑云杰)
