后路短节段内固定治疗胸腰段骨折取出内固定后再发后凸的危险因素分析
2017-09-26孙祥耀张希诺海涌
孙祥耀 张希诺 海涌
后路短节段内固定治疗胸腰段骨折取出内固定后再发后凸的危险因素分析
孙祥耀 张希诺 海涌
目的探讨后路短节段经伤椎椎弓根螺钉内固定术 ( short-segment pedicle instrumentation with screw insertion in the fractured vertebra,SSPI-f ) 治疗的胸腰段爆裂骨折患者内固定取出后再发后凸的危险因素及预测指标。方法收集 2006 年 1 月至 2013 年 1 月,于我院行 SSPI-f 治疗胸腰段爆裂骨折患者骨折节段后凸 Cobb’s 角、骨折节段局部 Cobb’s 角 ( regional angle,RA )、伤椎上位椎间盘角 ( upper intervertebral angle,UIVA )、伤椎下位椎间盘角 ( lower intervertebral angle,LIVA )、伤椎椎体楔形角 ( vertebral wedge angle,VWA )、伤椎椎体前缘高度比值 ( the anterior vertebra height ratio,AVH% )、伤椎椎体后缘高度比值 ( the posterior vertebra height ratio,PVH% )、伤椎椎体前后缘比值 ( anteroposterior ratio,A / P )、AVH%<50% 患者例数、伤椎上位终板损伤患者例数、载荷评分 ( load-sharing classification,LSC )、疼痛视觉模拟评分 ( visual analogue scale,VAS )、体质量指数 ( body mass index,BMI )。按照取出内固定后有无再发后凸将患者分为两组进行统计学比较。结果再发后凸组年龄 ( P<0.001 )、女性例数 ( P<0.001 )、BMI ( P<0.001 )、术前 UIVA ( P=0.002 ) 大于无再发后凸组,术前 A / P 比值 ( P=0.038 )、术前 AVH% ( P=0.003 ) 小于再发后凸组。其它指标组间差异均无统计学意义。Logistic 回归分析显示女性 ( R2=0.324,B=2.618,P<0.001 )、年龄 ( R2=0.509,B=0.728,P<0.001 )、BMI ( R2=0.509,B=0.728,P<0.001 )、术前 UIVA ( R2=0.160,B=0.282,P=0.004 ) 为再发后凸的危险因素。而术前 A / P 比值 ( R2=0.072,B=-0.049,P=0.043 )、术前 AVH% ( R2=0.143,B=-0.066,P<0.006 ) 为保护性因素。ROC 曲线结果显示年龄临界值为 49 岁 ( 曲线下面积=0.816 ),BMI 临界值为 25 ( 曲线下面积=0.871 ),术前 UIVA 临界值为 -4.5° ( 曲线下面积=0.667 ),其临界值有指导意义 ( 曲线下面积>0.5 )。而术前 AVH% ( 曲线下面积=0.317 )、术前 A / P 比值 ( 曲线下面积=0.386 ) 无指导意义 ( 曲线下面积<0.5 )。结论年龄、女性、BMI、术前 AVH%、术前 UIVA、术前 A / P 比值为内固定取出后再发后凸的影响因素。而 BMI 相对于其它因素更有指导意义。年龄>49 岁、BMI>25、术前 UIVA<-4.5° 为预测取出内固定后再发后凸风险的理想指标。
脊柱骨折;骨折固定术,内;脊柱后凸;危险因素
胸腰段 ( T10~L2) 为脊柱最容易发生创伤性骨折的节段;其处于活动度较小的胸椎与活动度较大的腰椎的交界处,因此比其它节段承受更多的应力[1-2]。超过 50% 的胸腰椎爆裂骨折最终导致后凸畸形伴发神经功能障碍[3]。虽然手术治疗方式的选择尚有争议,及时的治疗仍然十分必要。胸腰椎骨折可采用前路、后路或前后路联合的方法进行治疗[1-2]。手术治疗目的为进行椎管减压、恢复椎体高度,矫正脊柱后凸畸形,为早期复位提供稳定的支撑结构[4-5]。目前,后路短节段椎弓根螺钉内固定术( short-segment pedicle instrumentation,SSPI ) 已经得到广泛应用,其具有出血量少、后凸矫正度高、并发症少以及操作过程简单等优点[4,6]。然而采用固定伤椎上位及下位椎体的跨伤椎固定术治疗胸腰段爆裂骨折的治疗效果仍然难以达到预期效果[7-9]。
既往研究指出,手术治疗胸腰段骨折后再发后凸以及矫正度丢失主要由椎间盘塌陷引起,并且主要与上位椎间盘的塌陷有关[10-11]。后路短节段经伤椎椎弓根螺钉内固定术 ( short-segment pedicle instrumentation with screw insertion in the fractured vertebra,SSPI-f ) 通过对骨折椎体置钉,增加了内固定的强度从而降低内固定失败的发生率[12-13]。如果胸腰段爆裂骨折采用 SSPI-f 治疗时,术后再发后凸的发生能通过术前指标进行预测,将对临床治疗有重要的指导意义。对 2006 年 1 月至 2013 年 1 月,于我院接受 SSPI-f 治疗的 84 例胸腰段爆裂骨折患者的影像学及临床指标进行分析,探讨内固定取出后再发后凸的危险因素及预测指标,指导临床认识、治疗胸腰段爆裂骨折和判断预后。
资料与方法
一、纳入与排除标准
1. 纳入标准:( 1 ) 在伤后 3 天内进行手术治疗的患者;( 2 ) 内固定于术后 12 个月后取出,并随访12 个月以上的患者;( 3 ) 胸腰椎损伤分类及损伤程度评分 ( thoracolumbar injury classification and severity,TLICS ) >4 分的患者。
2. 排除标准:( 1 ) 多发性骨折;( 2 ) 病理性骨折;( 3 ) 术中采用后方以及侧后方植骨融合的患者。
二、一般资料
本研究共纳入 84 例,其中男 45 例,女 39 例,年龄 24~66 岁,平均 ( 48.4±11.0 ) 岁,随访时间25~30 个月,平均 ( 27.5±1.7 ) 个月。术前骨折节段后凸 Cobb’s 角 ( 24.8±2.9 ) °,内固定取出后骨折节段后凸 Cobb’s 角 ( 15.4±8.9 ) °,手术治疗后骨折节段后凸明显改善 ( P<0.001 )。取出内固定后末次随访矫正度为 ( 9.8±7.2 ) °,矫正度丢失 ( 7.5± 4.4 ) °。无一例出现其它内固定相关并发症。
三、分组方法
通过测量术后立位 X 线片中伤椎上位椎体上终板和下位椎体下终板之间的 Cobb’s 角,取得骨折节段术后 Cobb’s 角。根据取出内固定后末次随访矫正度丢失是否>5°,将患者分为再发后凸组和无再发后凸组[14]。其中再发后凸组共纳入 57 例,无再发后凸组共纳入 27 例。
四、测量指标与方法
1. 影像学评估:椎体骨折通过使用立位 X 线片以及仰卧位 CT 检查进行评估;通过 CT 检查确定上终板骨折。拍摄取钉前、取钉后的术后立位X 线片。通过测量术后立位 X 线片中伤椎上位椎体上终板和下位椎体下终板之间的 Cobb’s 角,取得骨折节段后凸 Cobb’s 角[14]。上位椎间盘角 ( upper intervertebral angle,UIVA ) 为伤椎上终板与上位椎体下终板之间的角度。下位椎间盘角 ( lower intervertebral angle,LIVA ) 为伤椎下终板与下位椎体上终板之间的角度。局部 Cobb’s 角 ( regional angle,RA ) 为伤椎上位椎体的下终板与下位椎体的上终板之间的角度。椎体楔形角 ( vertebral wedge angle,VWA ) 是骨折椎体上终板与下终板的连线,反映了后凸畸形的程度。前方与后方的角度。对伤椎前缘 ( anterior vertebra height,AVH0 ) 与后缘 ( posterior vertebra height,PVH0 ) 的椎体高度进行测量。伤椎椎体前缘高度比值 ( the anterior vertebra height ratio,AVH% )被定义为 AVH0 与上位椎体以及下位椎体高度平均值 [ average anterior height of upper and lower adjacent vertebra,( AVH1+AVH2 ) / 2 ] 的百分比。伤椎椎体后缘高度比值 ( the posterior vertebra height ratio,PVH% ) 被定义为 PVH0 与上位椎体以及下位椎体高度平均值 [ average posterior height of upper and lower adjacent vertebra,( PVH1+PVH2 ) / 2 ] 的百分比。伤椎椎体前后缘比值 ( anteroposterior ratio,A / P ) 为AVH0 与 PVH0 的百分比。分别统计 AVH%<50%以及伤椎上位终板损伤的患者例数。
2. 临床评估:TLICS 评分包括形态学、神经功能以及后方韧带完整性 3 个部分,通常用于评估损伤的严重程度。载荷评分 ( load-sharing classification,LSC ) 对椎体的粉碎程度、骨折块的移位程度以及后凸畸形需要矫正的程度对损伤的严重程度进行评分。疼痛视觉模拟评分 ( visual analogue scale,VAS ) 用于评估疼痛以及麻木。体质量指数( body mass index,BMI ) 用于评估患者体型特点。
五、统计学处理
采用 SPSS 17.0 软件进行统计学分析。计量资料使用±s 表示,计数资料用百分比表示。使用Kolmogorov-Smirnov 检验连续性变量是否符合正态分布,符合正态分布的变量使用 F 检验进行多重比较,偏态分布变量采用 Kruskal-Walllist 检验进行分析。非连续变量使用 χ2检验进行比较。采用 Logistic回归分析比较术后再发后凸与各评估指标的相互关系。采用 ROC 曲线估计危险因素临界值。P<0.05为差异有统计学意义。
结 果
一、组间各项指标比较
两组年龄、性别、术前 UIVA、术前 A / P 比值、术前 AVH%、术前 BMI 差异有统计学意义 ( P<0.05 ) ( 表1 );其余各指标差异无统计学意义 ( P>0.05 ) ( 表1 )。

表1 再发后凸组与非再发后凸组各项指标结果比较Tab.1 Comparison of measuring results between 2 groups
二、再发后凸危险因素 Logistic 回归分析
对有明显组间差异的指标进行单因素 Logistic 回归分析以确定取出内固定后再发后凸的危险因素。结果显示女性 ( R2=0.324,B=2.618,P<0.001 )、年龄( R2=0.509,B=0.728,P<0.001 )、BMI ( R2=0.509,B=0.728,P<0.001 )、术前 UIVA ( R2=0.160,B=0.282,P=0.004 ) 为再发后凸的危险因素。而术前A / P 比值 ( R2=0.072,B=-0.049,P=0.043 )、术前AVH% ( R2=0.143,B=-0.066,P=0.006 ) 为保护性因素。与其它指标相比,BMI 在 Logistic 回归模型中匹配程度较高,提示其预测性更强 ( 表2 )。
三、再发后凸危险因素 ROC 曲线分析
采用 ROC 曲线分析对危险因素中的连续性变量进行分析,以确定其临界值。结果显示,年龄临界值为 49 岁 ( 曲线下面积=0.816 ),BMI 临界值为 25 ( 曲线下面积=0.871 ),术前 UIVA 临界值为 -4.5°( 曲线下面积=0.667 ),其临界值有指导意义 ( 曲线下面积>0.5 )。而术前 AVH% ( 曲线下面积=0.317 )、术前 A / P 比值 ( 曲线下面积=0.386 ) 无指导意义 ( 曲线下面积<0.5 ) ( 表3,图1 )。

表2 再发后凸危险因素 Logistic 回归分析结果Tab.2 Results of Logistic regression analyzing risk factors of kyphosis recurrence
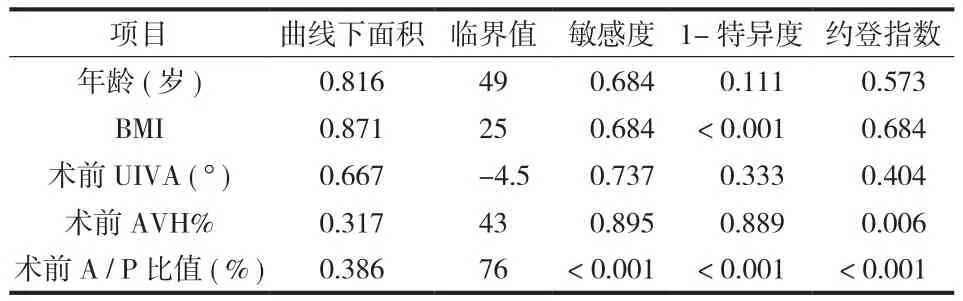
表3 再发后凸危险因素 ROC 曲线分析结果Tab.3 Results of ROC curve analyzing risk factors of kyphosis recurrence
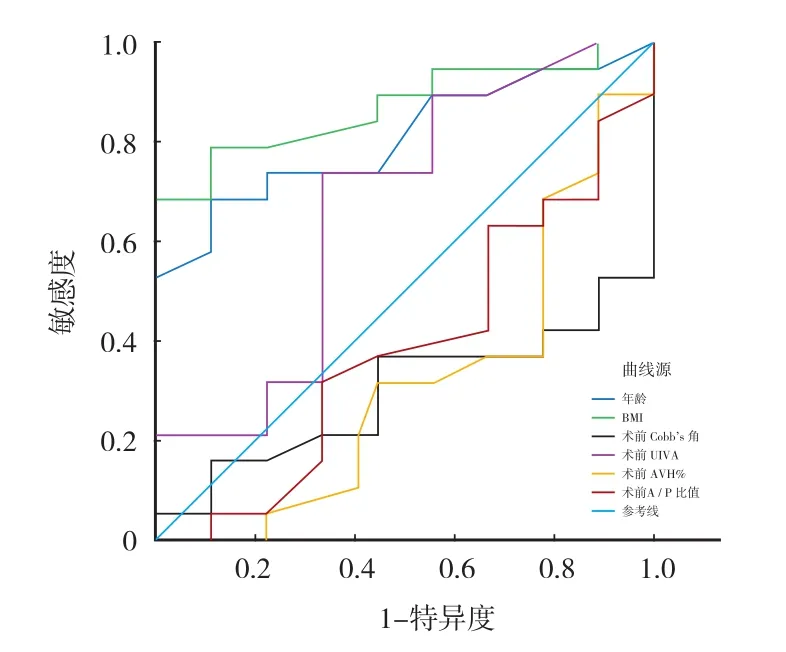
图1 再发后凸危险因素 ROC 曲线Fig.1 ROC curve of risk factors of kyphosis recurrence
讨 论
胸腰段骨折会引起脊柱稳定性破坏、后凸畸形、神经损伤甚至引起瘫痪[1-3]。保守治疗通常用于无神经损伤的稳定骨折[15]。然而,保守治疗并不总是达到预期的治疗效果[16-17]。脊柱骨折的手术治疗包括后路、前路、前后路联合手术,并在临床上均得到了广泛的应用。Roy-Camille 等[18]首先采用SSPI 治疗胸腰椎骨折。SSPI 具有减少手术出血、减少固定节段、缩短手术时间以及减少肌肉萎缩范围的特点[1,4,6]。传统 SSPI 仅固定伤椎上位及下位椎体,会出现再发后凸、内固定失败等不良时间,影响临床疗效[7-9]。SSPI-f 与传统 SSPI 相比更加安全可靠,其能够有效支撑前柱结构,提高内固定结构强度,降低内固定失败的发生率[12,19]。研究结果证实了 SSPI-f 在治疗胸腰段压缩爆裂骨折的有效性。除此之外,结果还提示年龄、术前 UIVA、术前 A / P、术前 AVH%、术前 BMI 与内固定取出后再发后凸有关。
以往研究指出,采用 SSPI-f 平均能够矫正 15°的后凸[12];其矫正度大于传统 SSPI[12]。本研究后凸 Cobb’s 角矫正度较小为 ( 9.8±7.2 ) °,可能与压缩程度较轻有关。胸腰段爆裂骨折的患者在采用传统 SSPI 治疗后,随访中出现矫正度丢失发生率较高[20-21]。McNamara 等[22]报道传统 SSPI 治疗胸腰段爆裂骨折术后矫正度丢失平均为 9°。本研究中SSPI-f 治疗胸腰段爆裂骨折内固定取出后末次随访矫正度丢失平均 ( 7.5±4.4 ) °;其矫正度丢失与上述传统 SSPI 相比明显下降。
既往关于再发后凸原因的研究指出,椎间盘塌陷是术后再发后凸的主要原因[10]。本研究结果表明,内固定取出后矫正度丢失与椎体塌陷无关;这是因为 VWA 与 AVH 在随访过程中无明显变化,而UIVA 矫正度丢失为再发后凸的主要原因[23]。目前仍然缺乏理想的分类系统对终板损伤进行评估。由于椎间盘和终板的解剖特点,终板血管破坏是椎间盘退变的主要原因,损伤的椎板很难修复[24]。有研究指出,椎间盘塌陷是对终板骨折后形态改变的适应性改变[8,25]。但是,本研究表明再发后凸与终板骨折无关。其可能原因为轻微的终板损伤不足以导致严重的终板形态变化、终板血管损伤、终板中央破坏以及椎间盘的吸收。既往研究表明椎间盘损伤多发生于椎体严重粉碎的胸腰段爆裂骨折[6]。椎间盘的结构特点使其具有一定弹性,与椎体相比能够更好地耐受损伤时瞬间增大的载荷[26]。因此,椎间盘损伤在轻度骨折中并不多见。本研究中 LSC 评分为( 5.9±1.1 ) 分,表明骨折程度较轻[7,27]。并且在 MRI检查提示椎间盘完整时,往往不采用椎间盘切除、椎体间植骨融合术治疗[1-2,26]。此外,本研究已经排除采用椎体间植骨融合术治疗的患者。综上所述,矫正度丢失主要由椎间盘退变加速引起,而并非椎间盘损伤引起。
本研究中,AVH% 下降会增加再发后凸的发生率;术前 A / P 和 AVH% 与再发后凸有关。通常AVH 下降往往表明椎体间稳定性下降;当 AVH%<50% 时,往往需采用手术治疗[28]。胸腰段爆裂骨折往往由屈曲应力联合轴向应力或伴有旋转应力引起;当 AVH% 明显下降时,椎体中松质骨压缩严重;尽管 SSPI-f 能够有效恢复椎体高度、稳定骨折节段,由于骨松质尚未修复,椎体内会遗留骨缺损区;椎间盘会因终板中部损伤而被缓慢挤压入椎体中骨缺损区,从而引起再发后凸[9-10]。在本研究中,术前 A / P 和 AVH% 为内固定取出后再发后凸的危险因素;然而 AVH%<50% 的患者例数无组间差异,其可能原因为本研究中纳入患者骨折严重程度较低,进一步提示再发后凸危险因素的界值并非固定值,具有特异性。
LSC 评分被广泛应用于指导胸腰段骨折的治疗[7]。本评分系统用于评估骨折椎体粉碎程度、骨折块移位程度以及骨折节段后凸的矫正程度[7,29]。Parker 等[27]指出胸腰段骨折 LSC 评分≤6 分时可以采用传统 SSPI 治疗,而 LSC 评分为 7 分时需要重建前柱结构。Dai 等[30]研究发现对于 LSC 评分<6 分的胸腰椎骨折患者,未采用后外侧植骨融合的传统 SSPI能够有效提高脊柱稳定性。Pellise 等[6]报道内固定取出前矫正度丢失与 LSC 评分有关,并指出椎间盘退变与椎体粉碎程度有关,粉碎程度越严重,矫正度丢失越严重。本研究中 LSC 评分与矫正度丢失无关。其原因可能为,LSC 评分主要反映椎体粉碎程度而与终板损伤情况无关;终板严重损伤时才可能损伤椎间盘营养供应,引起椎间盘退变[24]。因此,LSC 评分并不是预测再发后凸的可靠指标。TLICS 评分主要是根据患者骨折形态学特点、后韧带复合体的完整性以及神经功能状态等,对患者进行综合评估,从而指导治疗方式的选择[31-32]。本研究中发现TLICS 评分组间差异无统计学意义,其原因可能为TLICS 评分无法准确反映椎间盘受累情况,其评分受其它因素影响,不适用于预测再发后凸风险[33]。
本研究结果提示再发后凸与患者年龄相关,其原因可能为年龄越大,胸腰段结构功能下降越严重;女性发生再发后凸风险高于男性,其原因可能为随着年龄增加,女性发生退变疾病以及骨质疏松的发病率显著增加[34-36]。既往研究指出后凸矫正程度与疼痛程度以及功能改善无关;疼痛产生的原因为胸腰段后凸需要过度的腰前凸维持,这会造成肌肉的疲劳,从而引起疼痛;关节突关节的反常运动也会引起关节及周围组织损伤,从而引起疼痛[37-38]。本研究中术前 VAS 评分组间差异无统计学意义,提示术前 VAS 评分并非再发后凸的危险因素。肥胖对骨质疏松性骨折有明显影响,并且其随着年龄的增加而发生变化。既往研究通过 BMI 对肥胖与骨折的关系进行研究,但是两者之间的关系尚有争议[39-41]。Ong 等[42]指出 BMI 较高者骨密度较高。有研究指出 BMI 较高为脊柱内固定术后邻近节段退变的危险因素[43-44]。本研究发现 BMI 较高者发生再发后凸风险更高,其原因可能为 BMI 较高者对胸腰段结构产生的压力更大,影响内固定结构的稳定;虽然 BMI 较高者骨密度较高,然而术后矫正度丢失主要由椎间盘角度变化引起,与骨性结构无关,骨密度较高者在降低再发后凸方面无明显优势;BMI 较高者对椎间盘产生更高的压力,椎间盘结构会因为终板中部损伤而被缓慢挤压入椎体中骨缺损区造成再发后凸;BMI 较高者使椎间盘高度下降,缓冲能力降低,退变加速[36,42-44]。
Chen 等[23]在研究中指出年龄、A / P 比值以及AVH%<50% 与矫正度丢失有关,然而其未对各危险因素进行 Logistic 分析,未提出用于预测再发后凸风险的危险因素界值,影响其研究结果的参考价值。本研究中 Logistic 回归分析结果表明虽然年龄、女性、BMI、术前 AVH%、术前 UIVA、术前 A / P比值作为危险因素差异有统计学意义。然而 R2结果表明,BMI 与 Logistic 回归模型匹配程度较好,较其它因素更有指导意义。对再发后凸危险因素 ROC 曲线分析结果表明,年龄、BMI、术前 UIVA 的曲线下面积均>0.5,因此年龄>49 岁、BMI>25、术前UIVA<-4.5° 为较为理想的取出内固定后再发后凸的预测指标;而术前 AVH%、术前 A / P 比值因曲线下面积<0.5,因此并非理想预测指标。
本研究尚存在不足:首先本研究为单中心回顾性研究,存在选择偏倚;其次样本量较少。因此,需要多中心前瞻性随机对照试验对再发后凸的危险因素进行进一步研究。
综上所述,SSPI-f 是胸腰段爆裂骨折的有效治疗方法。年龄、女性、BMI、术前 AVH%、术前UIVA、术前 A / P 比值为内固定取出后再发后凸的危险因素。而 BMI 相对于其它因素更有指导意义。年龄>49 岁、BMI>25、术前 UIVA<-4.5° 为预测取出内固定后再发后凸风险的理想指标。
[1] Wood KB, Li W, Lebl DR, et al. Management of thoracolumbar spine fractures[J]. Spine J, 2014, 14(1):145-164.
[2] Rajasekaran S, Kanna RM, Shetty AP. Management of thoracolumbar spine trauma: An overview[J]. Indian J Orthop, 2015, 49(1):72-82.
[3] Wilcox RK, Boerger TO, Allen DJ, et al. A dynamic study of thoracolumbar burst fractures[J]. J Bone Joint Surg Am, 2003, 85-A(11):2184-2189.
[4] Xu BS, Tang TS, Yang HL. Long-term results of thoracolumbar and lumbar burst fractures after short-segment pedicle instrumentation, with special reference to implant failure and correction loss[J]. Orthop Surg, 2009, 1(2):85-93.
[5] 伍骥, 郑超, 黄蓉蓉. 重新认识胸腰段脊柱骨折的诊断和治疗[J]. 中国骨与关节杂志, 2016, 5(6):401-404.
[6] Pellise F, Barastegui D, Hernandez-Fernandez A, et al. Viability and long-term survival of short-segment posterior fixation in thoracolumbar burst fractures[J]. Spine J, 2015, 15(8): 1796-1803.
[7] McCormack T, Karaikovic E, Gaines RW. The load sharing classification of spine fractures[J]. Spine, 1994, 19(15): 1741-1744.
[8] Speth MJ, Oner FC, Kadic MA, et al. Recurrent kyphosis after posterior stabilization of thoracolumbar fractures. 24 cases treated with a Dick internal fixator followed for 1.5-4 years[J]. Acta Orthop Scand, 1995, 66(5):406-410.
[9] Alanay A, Acaroglu E, Yazici M, et al. Short-segment pedicle instrumentation of thoracolumbar burst fractures: does transpedicular intracorporeal grafting prevent early failure[J]? Spine, 2001, 26(2):213-217.
[10] Wang XY, Dai LY, Xu HZ, et al. Kyphosis recurrence after posterior short-segment fixation in thoracolumbar burst fractures[J]. J Neurosurg Spine, 2008, 8(3):246-254.
[11] Kim GW, Jang JW, Hur H, et al. Predictive factors for a kyphosis recurrence following short-segment pedicle screw fixation including fractured vertebral body in unstable thoracolumbar burst fractures[J]. J Korean Neurosurg Soc, 2014, 56(3):230-236.
[12] Mahar A, Kim C, Wedemeyer M, et al. Short-segment fixation of lumbar burst fractures using pedicle fixation at the level of the fracture[J]. Spine, 2007, 32(14):1503-1507.
[13] 吕豪珍, 林红, 张绍昆, 等. 经伤椎椎弓根置钉技术在胸腰段骨折中的应用[J]. 中国组织工程研究, 2012, 16(9): 1680-1683.
[14] Lee MC, Solomito M, Patel A. Supine magnetic resonance imaging Cobb measurements for idiopathic scoliosis are linearly related to measurements from standing plain radiographs[J]. Spine, 2013, 38(11):E656-661.
[15] Mumford J, Weinstein JN, Spratt KF, et al. Thoracolumbar burst fractures. The clinical efficacy and outcome of nonoperative management[J]. Spine, 1993, 18(8):955-970.
[16] Hitchon PW, Abode-Iyamah K, Dahdaleh NS, et al. Nonoperative management in neurologically intact thoracolumbar burst fractures: clinical and radiographic outcomes[J]. Spine, 2016, 41(6):483-489.
[17] Denis F, Armstrong GW, Searls K, et al. Acute thoracolumbar burst fractures in the absence of neurologic deficit. A comparison between operative and nonoperative treatment[J]. Clin Orthop Relat Res, 1984, (189):142-149.
[18] Roy-Camille R, Saillant G, Mazel C. Plating of thoracic, thoracolumbar, and lumbar injuries with pedicle screw plates[J]. Orthop Clin North Am, 1986, 17(1):147-159.
[19] 何建华, 冯大雄. 后路内固定融合术治疗不同分型胸腰椎骨折的临床疗效[J]. 中国脊柱脊髓杂志, 2016, 26(7):596-601.
[20] Carl L, Tromanhauser SG, Roger DJ. Pedicle screw instrumentation for thoracolumbar burst fractures and fracturedislocations[J]. Spine, 1992, 17(8 Suppl):S317-324.
[21] Cho DY, Lee WY, Sheu PC. Treatment of thoracolumbar burst fractures with polymethyl methacrylate vertebroplasty and short-segment pedicle screw fixation[J]. Neurosurgery, 2003, 53(6):1354-1361.
[22] McNamara MJ, Stephens GC, Spengler DM. Transpedicular short-segment fusions for treatment of lumbar burst fractures[J]. J Spinal Disord, 1992, 5(2):183-187.
[23] Chen JX, Xu DL, Sheng SR, et al. Risk factors of kyphosis recurrence after implant removal in thoracolumbar burst fractures following posterior short-segment fixation[J]. Int Orthop, 2016, 40(6):1253-1260.
[24] Kerttula LI, Serlo WS, Tervonen OA, et al. Post-traumatic findings of the spine after earlier vertebral fracture in young patients: clinical and MRI study[J]. Spine, 2000, 25(9): 1104-1108.
[25] Oner FC, van Gils AP, Faber JA, et al. Some complications of common treatment schemes of thoracolumbar spine fractures can be predicted with magnetic resonance imaging: prospective study of 53 patients with 71 fractures[J]. Spine, 2002, 27(6): 629-636.
[26] Furderer S, Wenda K, Thiem N, et al. Traumatic intervertebral disc lesion--magnetic resonance imaging as a criterion for or against intervertebral fusion[J]. Eur Spine J, 2001, 10(2): 154-163.
[27] Parker JW, Lane JR, Karaikovic EE, et al. Successful shortsegment instrumentation and fusion for thoracolumbar spine fractures: a consecutive 41/2-year series[J]. Spine, 2000, 25(9):1157-1170.
[28] Cantor JB, Lebwohl NH, Garvey T, et al. Nonoperative management of stable thoracolumbar burst fractures with early ambulation and bracing[J]. Spine, 1993, 18(8):971-976.
[29] Wang XY, Dai LY, Xu HZ, et al. The load-sharing classification of thoracolumbar fractures: an in vitro biomechanical validation[J]. Spine, 2007, 32(11):1214-1219.
[30] Dai LY, Jiang LS, Jiang SD. Posterior short-segment fixation with or without fusion for thoracolumbar burst fractures. a five to seven-year prospective randomized study[J]. J Bone Joint Surg Am, 2009, 91(5):1033-1041.
[31] Rihn JA, Anderson DT, Harris E, et al. A review of the TLICS system: a novel, user-friendly thoracolumbar trauma classification system[J]. Acta Orthop, 2008, 79(4):461-466.
[32] 张阳, 张志成, 李放, 等. 后方韧带复合体损伤在胸腰段骨折患者评估中的意义[J]. 中国骨与关节杂志, 2016, 5(6): 425-428.
[33] Kaul R, Chhabra HS, Vaccaro AR, et al. Reliability assessment of AOSpine thoracolumbar spine injury classification system and Thoracolumbar Injury Classification and Severity Score (TLICS) for thoracolumbar spine injuries: results of a multicentre study[J]. Eur Spine J, 2017, 26(5):1470-1476.
[34] Banks LM, Lees B, MacSweeney JE, et al. Effect of degenerative spinal and aortic calcification on bone density measurements in post-menopausal women: links between osteoporosis and cardiovascular disease[J]? Eur J Clin Invest, 1994, 24(12):813-817.
[35] Yu W, Gluer CC, Fuerst T, et al. Influence of degenerative joint disease on spinal bone mineral measurements in postmenopausal women[J]. Calcif Tissue Int, 1995, 57(3):169-174.
[36] Kim JY, Ryu DS, Paik HK, et al. Paraspinal muscle, facet joint, and disc problems: risk factors for adjacent segment degeneration after lumbar fusion[J]. Spine J, 2016, 16(7): 867-875.
[37] Wood KB, Bohn D, Mehbod A. Anterior versus posterior treatment of stable thoracolumbar burst fractures without neurologic deficit: a prospective, randomized study[J]. J Spinal Disord Tech, 2005, 18(Suppl):S15-23.
[38] Verlaan JJ, Oner FC. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit[J]. J Bone Joint Surg Am, 2004, 86-A(3):649-651.
[39] Skrzek A, Koziel S, Ignasiak Z. The optimal value of BMI for the lowest risk of osteoporosis in postmenopausal women aged 40-88 years[J]. Homo, 2014, 65(3):232-239.
[40] Oldroyd A, Mitchell K, Bukhari M. The prevalence of osteoporosis in an older population with very high body mass index: evidence for an association[J]. Int J Clin Pract, 2014, 68(6):771-774.
[41] De Laet C, Kanis JA, Oden A, et al. Body mass index as a predictor of fracture risk: a meta-analysis[J]. Osteoporos Int, 2005, 16(11):1330-1338.
[42] Ong T, Sahota O, Tan W, et al. A United Kingdom perspective on the relationship between body mass index (BMI) and bone health: a cross sectional analysis of data from the nottingham fracture liaison service[J]. Bone, 2014, 59:207-210.
[43] Liang J, Dong Y, Zhao H. Risk factors for predicting symptomatic adjacent segment degeneration requiring surgery in patients after posterior lumbar fusion[J]. J Orthop Surg Res, 2014, 9:97.
[44] Ou CY, Lee TC, Lee TH, et al. Impact of body mass index on adjacent segment disease after lumbar fusion for degenerative spine disease[J]. Neurosurgery, 2015, 76(4):396-402.
( 本文编辑:王萌 )
本刊被美国化学文摘数据库收录公告
本刊现为中国科技论文统计源期刊。2013 年 1 月,本刊经美国化学文摘 ( Chemical Abstracts,CA ) 数据库审理委员会审核通过,并从 2013 年第 1 期开始,正式被美国化学文摘数据库收录。特此公告!
CA 只收录本刊论著,其它文章不收录。
查询本刊请使用拼音:Zhongguo Gu Yu Guanjie Zazhi或本刊标准国际刊号 ( ISSN ):2095-252X,查询网址:http://cassi.cas.org/search.jsp。
《中国骨与关节杂志》编辑委员会
Risk factors of kyphosis recurrence after implant removal in the treatment of thoracolumbar burst fractures with posterior short-segment fixation
SUN Xiang-yao, ZHANG Xi-nuo, HAI Yong. Department of Orthopedics, Beijing Chaoyang Hospital, Capital Medical University, Beijing, 100020, China
ObjectiveTo evaluate the curative effects of short-segment pedicle instrumentation with screw insertion in the fracture level and find risk factors predicting kyphosis recurrence in thoracolumbar burst fractures.MethodsPatients with thoracolumbar burst fractures who underwent short-segment posterior pedicle screw instrumentation in the department of orthopedics, Beijing Chao Yang Hospital from January 2006 to January 2013 were carefully reviewed. Cobb’s angle of the fractured segment, RA ( regional angle ), UIVA ( upper intervertebral angle ), LIVA ( lower intervertebral angle ), VWA ( vertebral wedge angle ), AVH% ( the anterior vertebra height ratio ), PVH% ( the posterior vertebra height ratio ), the number of patient with AVH% < 50%, the number of patients with upper end plate injury, LSC ( load-sharing classification ), VAS ( visual analogue scale ), BMI ( body mass index ) were collected. The patients were divided into two groups according to if kyphosis occurred or not.ResultsAge ( P < 0.001 ), number of females ( P < 0.001 ), BMI ( P < 0.001 ), preoperative UIVA ( P = 0.002 ) in thegroup with kyphosis occurrence was larger than the group without kyphosis occurrence. Preoperative A / P ratio ( P = 0.038 ), preoperative AVH% ( P = 0.003 ) in the group with kyphosis occurrence was less than the group without kyphosis occurrence. No between-group differences were found in other parameters. Results of logistic regression analysis showed female ( R2= 0.324, B = 2.618, P < 0.001), age ( R2= 0.509, B = 0.728, P < 0.001 ), BMI ( R2= 0.509, B = 0.728, P < 0.001 ), preoperative UIVA ( R2= 0.160, B = 0.282, P = 0.004 ) were all risk factors of kyphosis recurrence. However, preoperative A / P ratio ( R2= 0.072, B = -0.049, P = 0.043 ), preoperative AVH% ( R2= 0.143, B = -0.066, P = 0.006 ) were protective factors. Results of ROC curve analysis showed the cut-off values of age, BMI, preoperative UIVA were 49 years old ( area under the curve = 0.816 ), 25 ( area under the curve = 0.871 ), -4.5 ( area under the curve = 0.667 ). However, preoperative AVH% ( area under the curve = 0.317 ) and preoperative A / P ratio ( area under the curve = 0.386 ) were of less guiding significance ( area under the curve < 0.5 ).ConclusionsAge, female, BMI, preoperative AVH%, preoperative UIVA, preoperative A / P ratio are impact factors of the kyphosis recurrence after the instrumentation removal. However, BMI seems to be better than other impact factors. Age > 49 years old, BMI > 25, preoperative UIVA < -4.5° are optimal predictive factors of the kyphosis recurrence after the instrumentation removal.
Spinal fractures; Fracture fixation, internal; Kyphosis; Risk factors
HAI Yong, Email: spinesurgeon@163.com
10.3969/j.issn.2095-252X.2017.09.013
R683.2
100020 北京,首都医科大学附属北京朝阳医院骨科
海涌,Email: spinesurgeon@163.com
2016-10-12 )