全髋关节置换术局部应用氨甲环酸安全性及有效性的 Meta 分析
2017-09-26尚义美刘明廷徐闯王建明任强李健杜长岭
尚义美 刘明廷 徐闯 王建明 任强 李健 杜长岭
. Mata 分析 Meta-analysis .
全髋关节置换术局部应用氨甲环酸安全性及有效性的 Meta 分析
尚义美 刘明廷 徐闯 王建明 任强 李健 杜长岭
目的用 Meta 分析的方法,探讨全髋关节置换术 ( total hip arthroplasty,THA ) 局部应用氨甲环酸 ( tranexamic acid,TXA ) 的安全性及有效性。方法计算机检索数据库 PubMed、BSCO、The Cochrane Library、中国知网、万方数据库,检索内容为关于局部应用 TXA 减少 THA 出血量的临床随机对照试验( randomized controlled trial,RCT ),检索时限为 1999 年 1 月至 2016 年 10 月。按纳入、排除标准进行随机对照试验筛查和质量评估,应用 RevMan 5.2 软件进行 Meta 分析。结果共纳入 11 篇文献,报告 1072 例,TXA组 569 例,对照组 503 例。局部应用 TXA 可以显著减少患者的总失血量 [ WMD=-419.51,95% CI ( -507.64,-331.38 ),P<0.00001 ]、输血率 [ RR=0.26,95% CI ( 0.18,0.36 ),P<0.00001 ];血栓栓塞事件发生率两组差异无统计学意义 [ RR=1.50,95% CI ( 0.42,5.40 ),P=0.54 ]。结论局部应用 TXA 可有效减少 THA 的总失血量和输血率,且不增加术后血栓栓塞并发症发生率。
氨甲环酸;投药,局部;关节成形术,置换术,髋;Meta 分析;有效性研究
全髋关节置换术 ( total hip arthroplasty,THA ) 是目前临床上先天性髋关节发育不良、髋关节退行性关节炎、股骨颈骨折、股骨头缺血性坏死的疗效确切治疗方法。但是,THA 围手术期大量失血导致患者术后需要输注异体血液纠正失血性贫血[1-2]。输血可能导致各种继发性并发症,如不良的免疫反应、血管内溶血、输血相关急性肺损伤、传染性疾病传播、输血引起的凝血功能障碍、肾功能衰竭、甚至增加死亡率[3-5]。
静脉输注氨甲环酸 ( tranexamic acid,TXA ) 应用于全膝关节置换术的效果已经得到了肯定,傅德杰等[6]的系统评价及 Meta 分析证明了 TXA 于全膝关节置换术可显著减少手术出血及术后输血,且不增加深静脉血栓形成的风险。然而,在 THA 这一失血量较多的髋部大手术中,考虑到静脉给药可能导致血栓栓塞并发症的风险,越来越多的学者已经开始把注意力及焦点转移到局部关节腔注射使用 TXA焦点上,髋关节腔局部使用 TXA 的应用一直存在争议,即局部应用 TXA 是否能有效减少手术出血、术后输血,其是否增加双下肢深静脉血栓及致死性肺栓塞等血栓栓塞并发症,很多学者针对这一问题已进行了大量的研究[7-8]。据相关研究推测,与静脉使用 TXA 相比,局部应用 TXA 在出血部位可提供TXA 的最大浓度,并且全身吸收 TXA 的量很少。需要注意的是,Benoni 及 Imai、Engel 等[9-11]研究均提示在 THA 手术结束及术后无论以何种方式给予( 包括局部关节腔注射 ) TXA,均不能显著降低 THA围手术期失血量,从而也就无法实现降低输血量的目的。
TXA 局部关节腔注射使用这一用药方法在 THA中的有效性与安全性目前尚未达成共识[12-14]。目前相关前瞻性研究所包括的病例数在 50~200 例左右不等,鉴于各研究的纳入标准与排除标准不尽相同,所使用假体类别 ( 骨水泥或非骨水泥) 不完全相同。因此,本研究采用随机对照试验的 Meta 研究,全面检索相关文献至 2016 年 10 月,纳入高质量RCT ( Jadad 评分>3 分 ),探讨关节腔注射 TXA 减少初次行 THA 患者总失血量和输血率的有效性,及是否增加血栓栓塞并发症的安全性。
资料与方法
一、纳入标准与排除标准
1. 纳入标准:( 1 ) 研究类型:所有在 THA 中局部应用 TXA 的临床随机对照试验 ( randomized controlled trial,RCT );( 2 ) 研究对象:接受 THA 治疗的患者,试验组和对照组的基线情况基本一致( 患者年龄、性别、病程、假体种类、手术方式 ),具有可比性;( 3 ) 干预措施:试验组局部应用TXA,对照组使用安慰剂;( 4 ) 记录指标:主要指标包括局部应用 TXA 组和安慰剂组术后总失血量、输血率及血栓栓塞并发症。
2. 排除标准:( 1 ) 不符合纳入标准,病例对照试验、临床非随机对照试验及低质量的随机对照试验,干预措施不在上述类型内,结局指标不包含上述主要指标;( 2 ) 重要资料报道不全;( 3 ) 无法获取全文;( 4 ) 同期行双侧 THA。
二、文献检索范围及策略
计算机检索数据库:PubMed、EBSCO、The Cochrane Library、中国知网、万方数据库。查阅所有检出文献和相关综述的参考文献作为补充文献,截止至 2016 年 10 月。英文检索词为“tranexamic acid”、“TXA”、“total hip arthroplasty”、“total hip replacement”、“THA”、“randomized controlled tria”、“RCT”;中文检索词为“氨甲环酸”、“全髋关节置换术”、“随机对照试验”。
三、文献筛选与质量评价
所有文献是否纳入由 2 名评价员共同决定,若有分歧第 3 位评价员介入,并通过讨论达成一致,决定最终是否纳入该文献。
纳人研究的方法学质量采用 Cochrane Handbook for Systematic Reviews of Interventions 5.1 中关于 RCT的质量评价标准进行评估:( 1 ) 是否采用正确的随机方法;( 2 ) 盲法的应用与否;( 3 ) 分配隐藏的应用与否;( 4 ) 失访或退出是否记录;( 5 ) 基线是否一致。同时根据 Jadad 评分量表进行评分,满分为 5 分,低质量研究为≤2 分,高质量研究为≥3 分。
四、资料提取及统计学处理
制订评价指标提取的表格,2 名研究者按照表格内容对文献中的数据进行提取。采用加权均数差( WMD ) 评价局部应用 TXA 组与安慰剂组总失血量,以 95% 可信区间 ( CI ) 表示;采用相对危险度( RR ) 评价输血率、血栓栓塞事件发生率,以 95% CI 表示。分析研究间的异质性,若 P<0.05 或 I2>50%,则认为多个研究结果异质性明显;若 P>0.05或 I2<50%,则认为多个同类研究无异质性。
结 果
一、检索结果
根据检索策略,通过数据库检索和其它资源检索获得相关文献 102 篇,剔除重复发表的 63 篇,经过阅读文章题目或摘要排除非随机对照试验 24 篇,进一步阅读全文剔除 2 篇研究干预措施分别为静脉滴注 TXA 与局部应用相比较,2 篇研究 Jadad 评分<3 的文献,最终纳入 11 篇高质量文献,共计 1072 例患者 ( 图1 )。
二、纳入文献的基本特征
纳入研究的特征见表1。
三、质量评价及发表偏倚的评价
按照 Cochrane 系统 5.1.0 评价手册推荐的偏倚风险评估标准评价最终纳入研究的 11 篇高质量文献,均有不同水平的偏倚 ( 图2,3 )。根据漏斗图显示发表偏倚分布,无严重不对称及不完整,表明发表偏倚小 ( 图4 )。
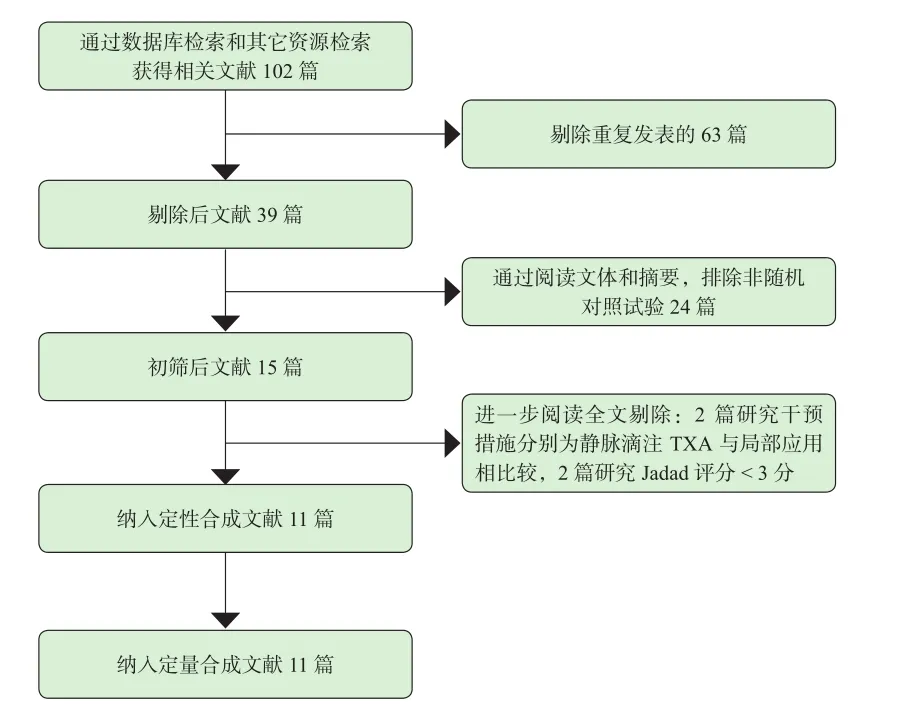
图1 文献筛选流程及结果Fig.1 Flow chart of study screening
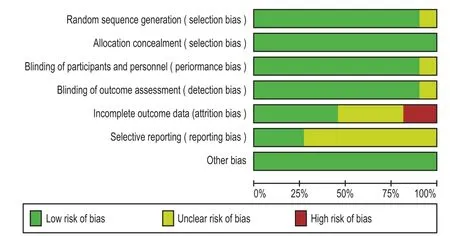
图2 偏倚风险图:判断纳入研究产生偏倚风险的项目所占百分比Fig.2 Bias risk items included in the study
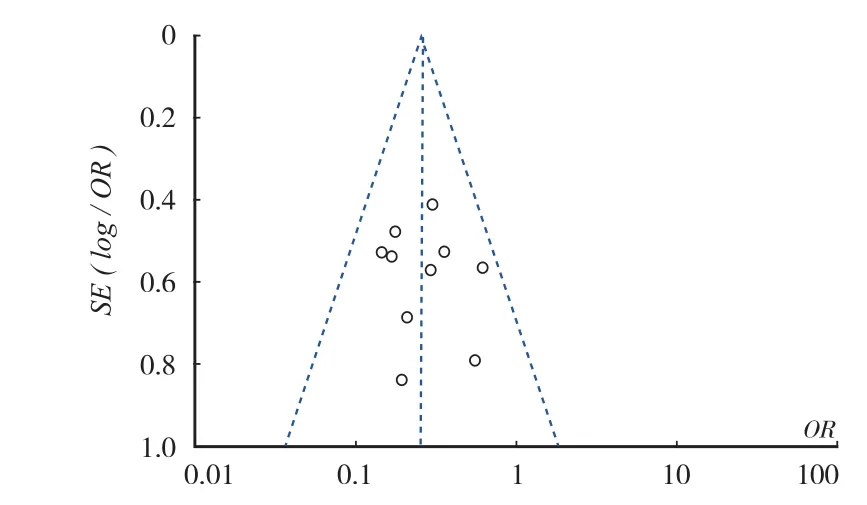
图4 纳入文献输血率漏斗图Fig.4 Funnel plot of transfusion rate in the study
四、总失血量
共纳入 11 篇文献,其中 6 篇文献报道了 THA总失血量,各研究之间存在异质性 ( χ2=13.60,I2=63%,P=0.02 ),采用随机效应模型,结果显示:局部应用 TXA 组的总失血量小于对照组,差异有统计学意义 WMD=-419.51,95% CI ( -507.64,-331.38 ),P<0.00001 ( 图5 )。
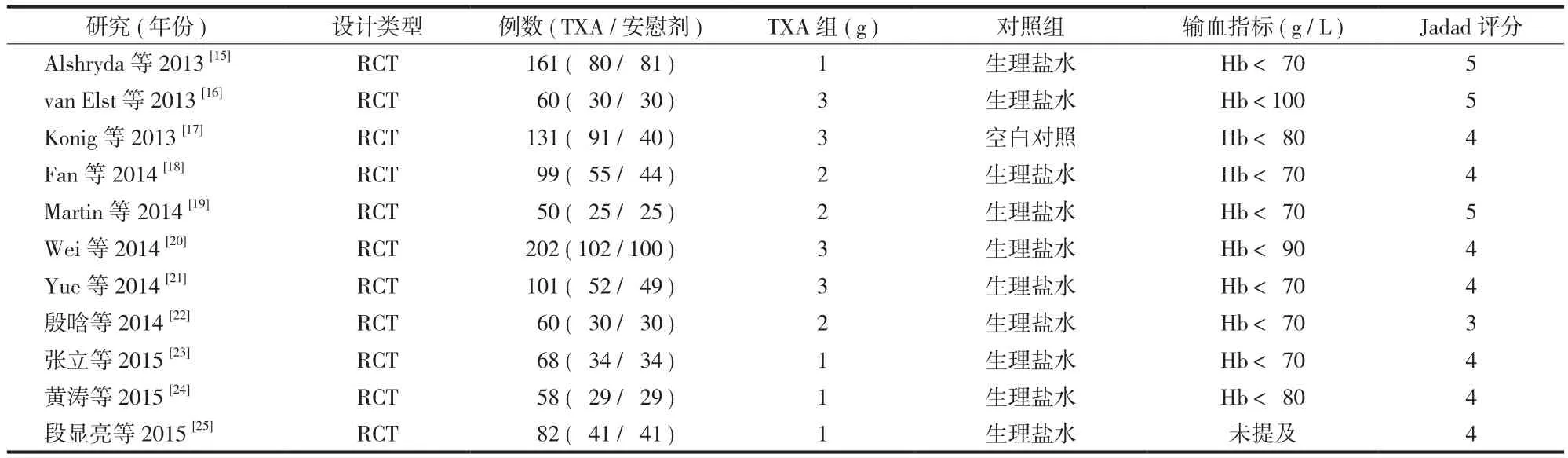
表1 纳入文献的基本特征Tab.1 Characteristics of included studies
五、输血率
其中 10 篇文献报道了 THA 术后输血率,各研究之间无统计学异质性 ( χ2=6.46,I2=0%,P=0.69 ),采用固定效应模型,结果显示:局部应用 TXA 组的输血率少于对照组,差异有统计学意义 RR=0.26,95% CI ( 0.18,0.36 ),P<0.00001 ( 图6 )。
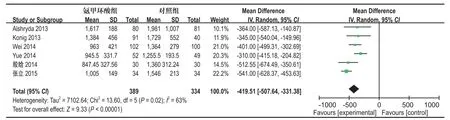
图5 两组患者术后总失血量比较的森林图Fig.5 The forest plot of relationship between total blood loss of 2 groups
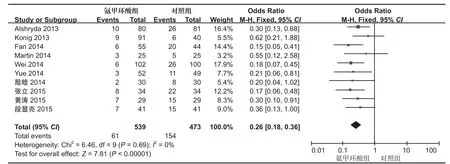
图6 两组患者术后输血率比较的森林图Fig.6 The forest plot of relationship between transfusion rates of 2 groups
六、THA 术后血栓栓塞发生率
其中 10 篇文献报道了 THA 术后血栓栓塞的发生率,各研究之间无异质性 ( χ2=0.56,I2=0%,P=0.91 ),采用固定效应模型,结果显示:局部应用TXA 组的血栓栓塞发生率与对照组差异无统计学意义 RR=1.50,95% CI ( 0.42,5.40 ),P=0.54 ( 图7 )。
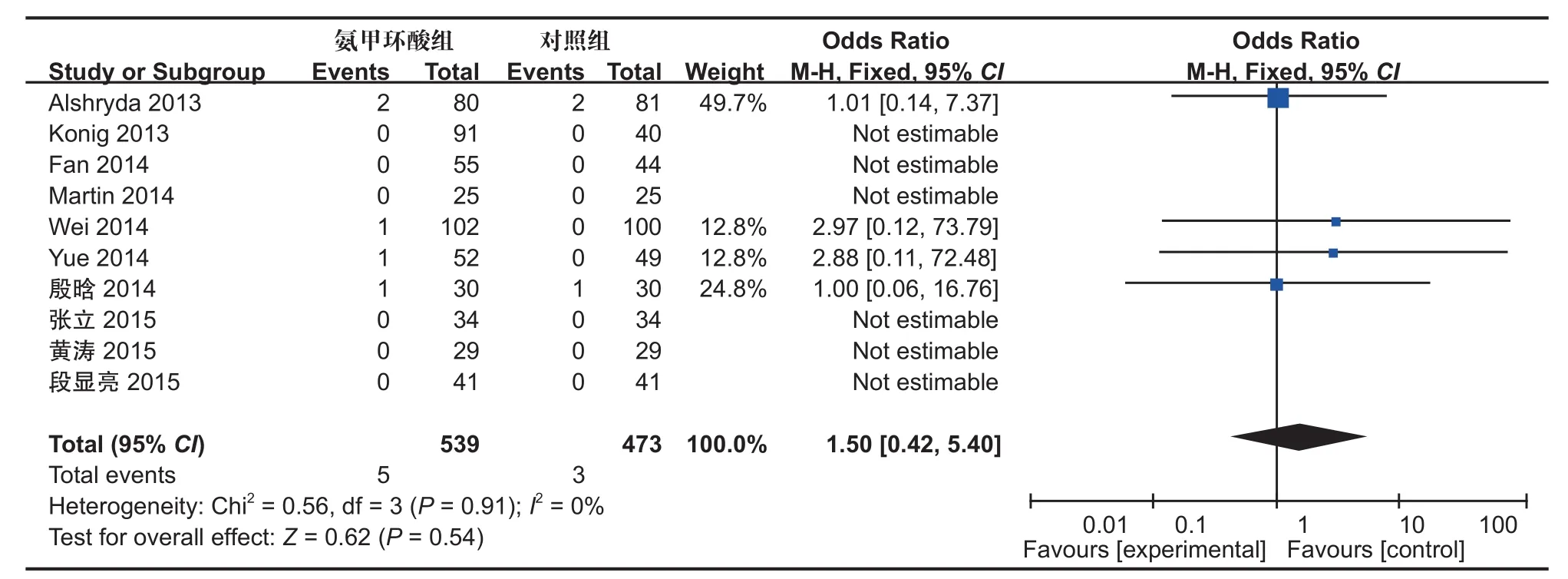
图7 两组患者术后静脉血栓栓塞并发症比较的森林图Fig.7 The forest plot of relationship between the incidence of thromboembolic complications of 2 groups
讨 论
目前,已有多种减少 THA 出血的技术应用于临床,其中包括了铁剂的治疗、自体血回输及抗纤溶药物的应用等[26]。TXA 实质上为赖氨酸的合成衍生物,能可逆地阻止纤溶酶原上的赖氨酸结合位点,从而起抗纤维蛋白溶解作用,理论上说 TXA 能在一定程度上减少 TKA 术中及术后失血[27-28]。目前,TXA 已经广泛应用于外科学多个领域,如心血管外科、胃肠道出血、产后出血、肝移植、髋关节和膝关节置换术[29-32]。静脉注射 TXA 已降低初次 THA失血[33-35]。然而,关于 TXA 最显著的问题是全身血栓栓塞并发症发生的风险。
孙程等[36]指出 TXA 可安全有效地降低 THA 术中、术后显性失血量及隐形失血量,且不增加 DVT及 PE 的风险,同时在减少住院时间、缩短术后恢复时间等方面也表现出确切的临床效果。TXA 局部使用可直接快速达到有效止血作用,并且其被吸收入血液循环的毒性浓度较低,相关文献报道 TXA局部使用的血液浓度是相同剂量静脉使用浓度的70%[37],能有效降低肾脏损害、VTE、心脑血管疾病等全身并发症。
本研究结果显示,TXA 局部使用与对照组相比可显著降低 THA 围手术期总失血量及输血率,在输血率方面差异无统计学意义。但在总失血量方面各研究之间存在异质性,分析原因可能与患者基线水平、假体型号、麻醉方式、TXA 的剂量和使用等原因有关。Konig 等[17]发现在单侧非骨水泥 THA 中局部使用 3 g TXA,可有效减少总失血 345 ml,输血率从 15% 降至 1%。Martin 等[19]也发现局部使用 2 g TXA 可降低单侧 THA 术后 Hb 下降程度,用药组患者平均输血量较对照组少,但差异无统计学意义。有随机对照试验结果发现 TXA 局部使用可降低输血风险,减少术后出血[15]。
本研究结果 Meta 显示,两组血栓栓塞发生率差异无统计学意义。骨科医生最大的顾虑是 TXA 局部应用是否增加 THA 术后静脉血栓事件发生率,本研究纳入的高质量文献研究显示 TXA 的局部使用不会增加术后静脉血栓发生率,而肺栓塞的发生更是少见[15-25]。仅少数文献报道有 DVT 及 PE 的发生,但差异并无统计学意义,且作者分析与局部使用 TXA无关[38]。
本研究存在的局限性为:( 1 ) 目前的前瞻性随机对照研究样本例数较少,只有 1072 例患者;( 2 ) TXA 的使用时间、剂量,假体的类型及手术技术等均可影响结果。
总结,TXA 局部关节腔注射这种使用方法可减少THA 总失血量和输血率,具有有效性;同时其不增加THA 术后血栓栓塞并发症发生率,具有安全性。
[1] Zhao J, Li J, Zheng W, et al. Low body mass index and blood loss in primary total hip arthroplasty: results from 236 consecutive ankylosing spondylitis patients[J]. Bio Med Res Int, 2014, 2014:742393.
[2] Bruce W, Campbell D, Daly D, et al. Practical recommendations for patient blood management and the reduction of perioperative transfusion in joint replacement surgery[J]. ANZ J Surg, 2013, 83(4):222-229.
[3] Madjdpour C, Spahn DR. Allogeneic red blood cell transfusions: efficacy, risks, alternatives and indications[J]. Br J Anaesth, 2005, 95(1):33-42.
[4] Wang W, Liao Q, Wu X, et al. Potential risk of blood transfusion-transmitted brucellosis in an endemic area of China[J]. Transfusion, 2015, 55(3):586-592.
[5] Malhotra S, Dhawan HK, Jain A, et al. Acute hemolytic transfusion reaction in a patient with Bombay phenotype: Implications for ABO grouping[J]. Indian J Hematol Blood Transfus, 2014, 30(1):108-110.
[6] 傅德杰, 陈凯宁, 杨柳. 氨甲环酸对全膝关节置换术失血量影响的系统评价[J]. 中国矫形外科杂志, 2012, 20(13): 1172-1173.
[7] Chang CH, Chang Y, Chen DW, et al. Topical tranexamic acid reduces blood loss and transfusion rates associated with primary total hip arthroplasty[J]. Clin Orthop Relat Res, 2014, 472(5):1552-1557.
[8] Gilbody J, Dhotar HS, Perruccio AV, et al. Topical tranexamic acid reduces transfusion rates in total hip and knee arthroplasty[J]. J Arthroplasty, 2014, 29(4):681-684.
[9] Benoni G, Lethagen S, Nilsson P, et al. Tranexamic acid, given at the end of the operation, does not reduce postoperative blood loss in hip arthroplasty[J]. Acta Orthop Scand, 2000, 71(3): 250-254.
[10] Imai N, Dohmae Y, Suda K, et al. Tranexamic acid for reduction of blood loss during total hip arthroplasty[J]. J Arthroplasty, 2012, 27(10):1838-1843.
[11] Engel JM, Hohaus T, Ruwoldt R, et al. Regional hemostatic status and blood requirements after total knee arthroplasty with and without tranexamic acid or aprotinin[J]. Anesth Analg, 2001, 92(3):775-780.
[12] Tuttle JR, Ritterman SA, Cassidy DB, et al. Cost benefitanalysis of topical tranexamic acid in primary total hip and knee arthroplasty[J]. J Arthroplasty, 2014, 29(8):1512-1515.
[13] Wind TC, Barfield WR, Moskal JT. The effect of tranexamic acid on transfusion rate in primary total hip arthroplasty[J]. J Arthroplasty, 2014, 29(2):387-389.
[14] 谢锦伟, 岳辰, 裴福兴. 氨甲环酸在全髋关节置换术中的有效性与安全性研究进展[J]. 中国矫形外科杂志, 2014, 22(20): 1856-1860.
[15] Alshryda S, Mason J, Vaghela M, et al. Topical (intra-articular) tranexamic acid reduces blood loss and transfusion rates following total knee replacement[J]. J Bone Joint Surg, 2013, 95(21):1961-1968.
[16] Van Elst CE, Vanbiervliet J, Simon JP, et al. The Effect of Topical Application of Tranexamic Acid in Total Hip Arthroplasty through the Direct Anterior Approach[J]. American Academy of Orthopaedic Surgeons Annual Meeting, March, 2013.
[17] Konig G, Hamlin BR, Waters JH. Topical tranexamic acid reduces blood loss and transfusion rates in total hip and total knee arthroplasty[J]. J Arthroplasty, 2013, 28(9):1473-1476.
[18] Fan FC, Gui BJ. Tranexamic acid injection through articular cavity and discontinuous clip pipe after total hip arthroplasty: changes in bleeding amount[J]. Chin J Tissue Eng Res, 2014, 18(40):6397-402.
[19] Martin JG, Cassatt KB, Kincaid-Cinnamon KA, et al. Topical administration of tranexamic acid in primary total hip and total knee arthroplasty[J]. J Arthroplasty, 2014, 29(5):889-894.
[20] Wei W, Wei B. Comparison of topical and intravenous tranexamic acid on blood loss and transfusion rates in total hip arthroplasty[J]. J Arthroplasty, 2014, 29(11):2113-2116.
[21] Yue C, Kang P, Yang P, et al. Topical application of tranexamic acid in primary total hip arthroplasty: a randomized doubleblind controlled trial[J]. J Arthroplasty, 2014, 29(12):2452-2456.
[22] 殷晗, 王大伟, 马文谱, 等. 经引流管逆行注入氨甲环酸降低初次全髋置换术后失血量的有效性及近期安全性评估[J].中华关节外科杂志 (电子版), 2014, 8(5):84-87.
[23] 张立, 王代荣, 赵国平, 等. 氨甲环酸静脉联合局部应用在全髋关节置换术中的疗效评价[J]. 实用医学杂志, 2015, 31(20): 3358-3360.
[24] 黄涛, 刘世清. 全髋关节置换术关节内注射氨甲环酸预防术后失血的效果[J]. 临床骨科杂志, 2015, 18(4):440-442.
[25] 段显亮, 孙波, 程维, 等. 氨甲环酸在全髋关节置换术中局部应用的安全性和有效性研究[J]. 北华大学学报 (自然科学版), 2015, 16(5):627-630.
[26] 岳辰, 康鹏德, 沈彬, 等. 氨甲环酸用于首次髋关节置换术的系统评价和 Meta 分析[J]. 中国矫形外科杂志, 2013, 21(12): 1167-1172.
[27] Xu Q, Yang Y, Shi P, et al. Repeated doses of intravenous tranexamic acid are effective and safe at reducing perioperative blood loss in total knee arthroplasty[J]. Biosci Trends, 2014, 8(3):169-175.
[28] Hoylaerts M, Lijnen HR, Collen D. Studies on the mechanism of the antifibrinolytic action of tranexamic acid[J]. Biochim Biophys Acta, 1981, 673(1):75-85.
[29] Wang H, Shen B, Zeng Y. Comparison of topical versus intravenous tranexamic acid in primary total knee arthroplasty: A Meta-analysis of randomized controlled and prospective cohort trials[J]. Knee, 2014, 21(6):987-993.
[30] Clavé A, Fazilleau F, Dumser D, et al. Efficacy of tranexamic acid on blood loss after primary cementless total hip replacement with rivaroxaban thromboprophylaxis: a casecontrol study in 70 patients[J]. Orthop Traumat: Surg Res, 2012, 98(5):484-490.
[31] Dalmau A, Sabaté A, Acosta F, et al. Tranexamic acid reduces red cell transfusion better than ε-aminocaproic acid or placebo in liver transplantation[J]. Anesth Analg, 2000, 91(1):29-34.
[32] Aoki A, Suezawa T, Yamamoto S, et al. Effect of antifibrinolytic therapy with tranexamic acid on abdominal aortic aneurysm shrinkageafter endovascular repair[J]. J Vasc Surg, 2014, 59(5):1203-1208.
[33] Sukeik M, Alshryda S, Haddad FS, et al. Systematic review and Meta-analysis of the use of tranexamic acid in total hip replacement[J]. J Bone Joint Surg Br, 2011, 93(1):39-46.
[34] Rajesparan K, Biant LC, Ahmad M, et al. The effect of an intravenous bolus of tranexamic acid on blood loss in total hip replacement[J]. J Bone Joint Surg Br, 2009, 91(6):776-783.
[35] Oremus K, Sostaric S, Trkulja V, et al. Influence of tranexamic acid on postoperative autologous blood retransfusion in primary total hip and knee arthroplasty: a randomized controlled trial[J]. Transfusion, 2014, 54(1):31-41.
[36] 孙程, 陆海明, 吕杰, 等. 氨甲环酸在初次全髋关节置换术中的应用[J]. 中国矫形外科杂志, 2015, 23(2):139-143.
[37] Wong J, Abrishami A, El Beheiry H, et al. Topical application of tranexamic acid reduces postoperative blood loss in total knee arthroplasty[J]. J Bone Joint Surg Am, 2010, 92(15): 2503-2513.
[38] Garneti N, Field J. Bone bleeding during total hip arthroplasty after administration of tranexamic acid[J]. Arthroplasty, 2004, 19(4):488-492.
Effectiveness and safety of topical tranexamic acid in total hip arthroplasty: a meta-analysis
SHANG Yi-mei, LIU Ming-ting, XU Chuang, WANG Jian-ming, REN Qiang, LI Jian, DU Chang-ling. Department of Bone and Joint Surgery, Binzhou Medical College affiliated Hospital, Binzhou, Shandong, 256600, China
ObjectiveTo explore the effectiveness and safety of topical tranexamic acid in total hip arthroplasty.MethodsThe criteria for inclusion and exclusion were formulated. Following databases were searched, PubMed, EBSCO, The Cochrane Library, WanFang database and China National Knowledge Infrastructure ( CNKI ), from Jan. 1999 to Oct. 2016. A Meta-analysis for screening and quality estimation were conducted with Review Manager 5.2.ResultsEleven eligible studies involving 1072 participants ( 569 topical TXA and 503 control ) were included in this meta-analysis. Topical tranexamic acid significantly reduced the total blood loss [ WMD = -419.51, 95% CI ( -507.64, -331.38 ), P < 0.00001 ], and the proportion of patients requiring blood transfusion [ RR = 0.26, 95% CI ( 0.18, 0.36 ), P < 0.00001 ], without increased thromboembolic complications [ RR = 1.50, 95% CI ( 0.42, 5.40 ), P = 0.54 ).ConclusionsTopical tranexamic acid is effective in reducing total blood volume and transfusion rate of total hip arthroplasty; in the meantime, it is safe and will not increase the incidence of thromboembolic complications.
Tranexamic acid; Administration, topical; Arthroplasty, replacement, hip; Meta-analysis; Validation studies
GU Xin-feng, Email: guxinfengshuguang@163.com
10.3969/j.issn.2095-252X.2017.09.010
R687.4
山东省自然科学基金 ( ZR2015PH006 )
256600 山东,滨州医学院附属医院骨关节外科
刘明廷,Email: 18865675365@163.com
2016-11-14 )
( 本文编辑:李贵存 )