改良肠道准备法在便秘患者肠镜检查中的应用
2017-08-22卢乐孟小芬屈平敏白育花李华徐心
卢乐,孟小芬,屈平敏,白育花,李华,徐心
(西安交通大学第二附属医院 普通外科,陕西 西安 710004)
改良肠道准备法在便秘患者肠镜检查中的应用
卢乐,孟小芬,屈平敏,白育花,李华,徐心
(西安交通大学第二附属医院 普通外科,陕西 西安 710004)
目的 评价改良肠道准备法复方聚乙二醇电解质散(SF-PEG,舒泰清)联合硫酸镁在便秘患者结肠镜检查肠道准备的效果。方法取行结肠镜肠道准备的轻中度便秘患者60例,随机分为两组:A组,常规剂量SF-PEG(438.4 g,4 L),30例;B组,续服贯用SF-PEG(219.2 g,2 L)和硫酸镁(50.00% 50 ml,再口服250 ml温开水),30例。Boston肠道准备量表(BBPS)、肠腔内气泡评分和结肠镜检查时间由同一内镜医师单盲记录,药物耐受性、再次肠道准备接受率和不良反应采用患者问卷调查。结果所有患者均完成肠道准备和结肠镜检查。B组结肠镜检查时间短于A组(P <0.05);B组BBPS总分高于A组(P <0.05);B组肠腔内气泡评分明显低于A组(P <0.05);B组再次肠道准备接受率明显高于A组(P <0.05)。A、B两组口感和总体不良反应发生情况评分无明显差异(P >0.05)。结论应用SF-PEG联合硫酸镁法,对轻中度便秘患者行结肠镜检查,具有耐受性好、清洁度高、镜检效果好和安全可靠等优点,推荐临床应用。
复方聚乙二醇电解质散;硫酸镁;便秘;结肠镜检查;肠道准备
便秘患者常伴有肠道运动异常和排空能力差,故行肠道准备比较困难[1]。目前国内外常用的肠道准备方式是口服复方聚乙二醇电解质散(polyethylene glycol electrolyte powder,SF-PEG),对便秘患者行肠道准备有许多缺点,如口感差、服量大、肠道清洁度低和耗时长,更重要的是易漏检微小病变[2-3]。国内常用50.00%的硫酸镁100 ml口服行肠道准备[4]。为此,本研究采用SF-PEG联合硫酸镁对便秘患者行肠道准备,克服了单用SF-PEG方案的诸多缺点,提高患者的依从性,达到肠道清洁的效果。
1 资料与方法
1.1 一般资料
选取2014年10月7日-2016年10月31日在西安交通大学第二附属医院普通外科拟行结肠镜检查的轻中度便秘患者60例(男26例,女34例),年龄21~83岁,平均年龄(49.1±12.9)岁。纳入标准:符合罗马Ⅲ便秘诊断标准[5],无严重呼吸循环系统疾病,无肠炎病史,无放疗化疗病史。排除标准:①重度便秘患者;②存在胃肠道梗阻、出血、穿孔、扭转和严重肠炎等;③肝肾功能不全;④大量腹水;⑤妊娠期患者;⑤水电解质紊乱;⑥对本研究药物过敏;⑦近2年内有肠道手术。
本研究经西安交通大学第二附属医院伦理委员会审查并批准,所有患者均已签署知情同意书。入组前后禁服用其他泻药。
根据纳入和排除标准,共纳入60例患者,A和B组各30例,均完成肠道准备和全结肠镜检查,满足肠镜检查需要。两组间性别、年龄、体重和腹泻便秘交替史等一般情况差异无统计学意义(P >0.05)。见表1。

表 1 两组患者一般情况Table 1 Baseline demographic variables and clinical characteristics between the two groups
1.2 方法
1.2.1 改良肠道准备方案 符合标准的患者随机分为A、B两组。A组:按说明将SF-PEG(商品名:舒泰清,舒泰神<北京>生物制药股份有限公司,164.4 g/盒)438.4 g配成4 L溶液,4 h内服完。
B组:SF-PEG 219.2 g配成2 L溶液,2 h内服完,检查前2 h服用硫酸镁(先口服50.00%硫酸镁50 ml,再口服250 ml温水),至排出液似清水样便后行结肠镜检查。
两组患者检查前1 d均进少渣饮食,于结肠镜检查前6 h开始服用不同方案溶液,当天禁食至检查完毕。
1.2.2 肠道准备有效性评价 采用单盲法,由同一内镜医师记录。按Boston肠道准备评估量表(boston bowel preparation scale,BBPS)[6]将结直肠分为3段:回盲部至升结肠、横结肠至降结肠和乙状结肠至直肠,每段结肠评分为3分,总计9分。3分:肠道准备良好,视野清晰,不影响进镜操作和观察;2分:肠道准备较好,视野尚清,负压吸引后不影响观察;1分:肠道准备欠佳,视野模糊,不能顺利进镜和观察肠壁;0分:肠道准备不佳,肠壁积满糊状便或粪水。总评分在0~4分为肠道准备质量差,5~9分为肠道准备质量优良。肠腔内气泡:0分,无;1分,少量;2分,较多;3分,大量。
1.2.3 耐受性和不良反应评价 耐受性用患者问卷调查评价,并且记录再次肠道准备接受率,其中前者包括肠道准备过程感受(0分,无不适;1分,轻度不适;2分,可耐受;3分,不能耐受)。医师记录肠道准备过程中一般情况(出冷汗、饥饿感、头晕、乏力、心悸),胃肠道不适(恶心、呕吐、腹胀和腹痛等)等不良反应发生情况,对总体不良反应进行评分(0分,无;1分,轻度;2分,中度;3分,重度)。
1.3 统计学方法
数据分析采用SPSS 16.0软件,计量资料采用均数±标准差(±s)描述,行t检验;计数资料采用例(%)描述,行χ2检验。P <0.05为差异具有统计学意义。
2 结果
2.1 肠道准备有效性
结肠镜检查由同一内镜医师操作,肠镜检查时间、BBPS总分和肠腔内气泡评分也均由同一医师完成记录。可见B组结肠镜检查时间(7.25±2.17)短于A组(9.00±3.50),两组间差异有统计学意义(P <0.05);B组BBPS总分(7.85±1.00)高于A组(6.35±1.25),两组间差异有统计学意义(P <0.05);B组肠腔内气泡评分(0.25±0.55)明显低于A组(0.75±0.50),两组间差异有统计学意义(P <0.05)。可见B组肠道准备的有效性明显高于A组。见表2。
2.2 两组耐受性和安全性
从评价耐受性和安全性看,B组口感和肠道接受率略低于A组,两组间差异无统计学意义(P >0.05),考虑与B组肠道准备较A组程序多时间长有关;B组(27例,90.00%)再次肠道准备接受率显著高于A组(22例,73.33%),两组间差异有统计学意义(P <0.05)。两组间服药前后血压和心率差值差异无统计学意义(P >0.05),仅1例B组69岁患者服用SF-PEG时出现持续约5 min心慌气短,给予对症处理后,不影响肠镜检查。两组服药前后血常规、电解质(血钠、血钙、血磷、尿素氮和肌酐)等指标均无明显变化。A和B组间总体不良反应发生情况评分差异无统计学意义(P >0.05)。见表 3。
表 2 两组患者肠道准备有效性比较 (±s)Table 2 Comparison of efficacy of bowel preparation between the two groups (±s)
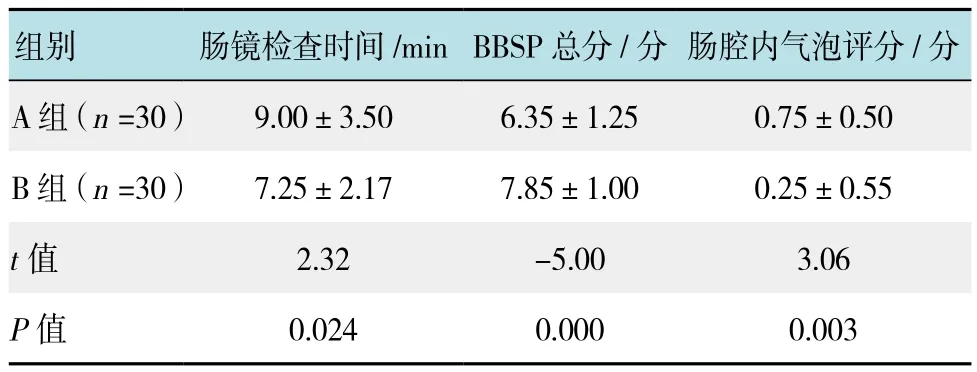
表 2 两组患者肠道准备有效性比较 (±s)Table 2 Comparison of efficacy of bowel preparation between the two groups (±s)
组别 肠镜检查时间/minBBSP总分/分 肠腔内气泡评分/分A组(n =30) 9.00±3.50 6.35±1.25 0.75±0.50 B组(n =30) 7.25±2.17 7.85±1.00 0.25±0.55 t值 2.32 -5.00 3.06 P值 0.024 0.000 0.003

表 3 两组患者耐受性和安全性比较Table 3 Comparison of tolerance and safety between the two groups
3 讨论
根据《中国慢性便秘诊治指南(2013,武汉)》统计[7],我国社区成人慢性便秘的患病率为4.00%~6.00%,随年龄增长而升高,60岁以上人群慢性便秘患病率可高达22.00%。对于存在便秘的患者,进行肠镜检查的肠道准备较非便秘患者要求高,更不容易达到《中国消化内镜诊疗相关肠道准备指南(草案)(2014)》肠道准备的理想标准[8]:①能在短时间内排空结肠内粪便;②不引起结肠黏膜改变;③不会引起患者不适,依从性好;④不导致水电解质紊乱;⑤价格适中。截止目前,对便秘患者无任何一种药物或药物组合能完全符合上述要求。FANG等[9]报告在420例行肠镜检查中,有29.00%的患者存在慢性便秘,得出慢性便秘是肠道准备不良的预测因素之一。说明有近1/3患者存在慢性便秘,探讨便秘患者有效的肠道准备尤为重要。
SF-PEG是一种不吸收性电解质溶液,具有患者耐受性较好、肠道准备速度较快和引起水电解质紊乱少等优点,被认为是清洁结肠的首选药物。但最大缺点为服用溶液量大,因而易出现恶心、呕吐、腹胀和腹痛。ROTONDANO等[10]报道一项多中心前瞻性研究,分析3 276结肠镜检查的数据(2 178例门诊患者,1098例住院患者)用聚乙二醇(polyethylene glycol,PEG)4~6 L行肠道准备,仍因清洁不充分而导致的不能完成结肠镜检查的有369例患者,占11.26%。
50.00 %硫酸镁用于肠道准备,其机制为高渗的硫酸镁溶液通过渗透压差别将水分从肠壁组织间隙吸入肠腔,刺激肠蠕动加速肠排空。因其价格低廉、服液量小和依从性好,在SF-PEG上市前,国内较为普遍应用。其最大缺点为肠道刺激大,易发生水电解质紊乱,故单用硫酸镁肠道准备现已少用。为克服PEG和硫酸镁的缺点,国内外研究尝试不同种组合方法,如PEG联合枸橼酸镁、乳果糖、硫酸镁等可使PEG溶液摄入量从4 L减至2 L,在不影响肠道清洁度前提下,增加患者耐受性[1,11-12]。对于便秘患者,国内外也有文献报道,PEG联合伊托必利[13]、莫沙必利[14-15]、乳果糖[1,16]、四磨汤[17]和肠道水疗[18]等均能不同程度克服其缺点,取得较好的疗效。用PEG联合硫酸镁对便秘患者行肠道准备已有报道,但侧重于比较PEG联合硫酸镁效果与单用硫酸镁疗效的比较[19],而与PEG疗效的比较未见报道。LU等[1]报道90例便秘患者,用乳果糖联合PEG行肠道准备,优于单纯用PEG。为此本课题组在既往研究采用最佳时间进行肠道准备基础上[20],用SF-PEG联合硫酸镁对便秘患者行肠道准备,取得了良好的效果。
本研究发现以轻中度便秘患者SF-PEG常规剂量为对照组(A组),评估了低剂量SF-PEG联合硫酸镁方案(B组)在结肠镜检查前肠道准备中的效果,结果显示B组摄入液体量较A组减少约1 700 ml,与相关文献报道效果相当[12,15-16]。从患者肠镜检查时间、口感和再次肠道准备接受率等看,联合用药具有明显优势,而从安全性和不良反应发生情况看,安全可靠。推测SF-PEG可使便秘患者软化大便,促进排便后,小量硫酸镁适当刺激肠蠕动,加速排便,加快肠道准备。克服了常规剂量口感较差、服药大和耗时较长等弊端,使多数患者肠腔气泡快速消除,避免了肠镜操作过程中反复吸引和冲洗肠壁,易于发现微小或平坦、凹陷型病变,易于细致观察。
综上所述,应用SF-PEG联合硫酸镁法,对轻中度便秘患者行结肠镜检查,具有耐受性好、清洁度高、镜检效果好和安全可靠等优点,推荐临床应用。本研究的不足之处在于样本量偏小、未涉及前瞻性研究、未对纳入样本进行如年龄等亚组研究等,后续研究应及时跟进并完善。
[1]LU J, CAO Q, WANG X, et al. Application of oral lactulose in combination with polyethylene glycol electrolyte powder for colonoscopy bowel preparation in patients with constipation[J].Am J Ther, 2015, 23 (4): e1020-e1024.
[2]BELSEY J, CROSTA C, EPSTEIN O, et al. Meta-analysis: the relative efficacy of oral bowel preparations for colonoscopy 1985-2010[J]. Aliment Pharmacol Ther, 2012, 35(2): 222-237.
[3]胡祥鹏, 谢菁, 杨姣, 等. 聚乙二醇电解质散对不同结肠段清肠效果比较[J]. 中国内镜杂志, 2015, 21(2): 193-195.
[3]HU X P, XIE J, YANG J, et al. Comparison of cleaning quality of polyethylene glycol electrolyte solution for different colon segment[J]. China Journal of Endoscopy, 2015, 21(2): 193-195.Chinese
[4]阳凤, 班春景, 杨李荣, 等. 结肠镜检查肠道准备研究现状[J].安徽卫生职业技术学院学报, 2015, 14(5): 57-59.
[4]YANG F, BAN C J, YANG L R, et al. Research status of coloscope in bowel preparation[J]. Journal of Anhui Health Vocational &Thechnical College, 2015, 14(5): 57-59. Chinese
[5]ROME F. Guidelines—Rome III diagnostic criteria for functional gastrointestinal disorders[J]. J Gastrointestin Liver Dis, 2006, 15(3): 307-312.
[6]CALDERWOOD A H, SCHROY P C, LIEBERMAN D A, et al.Boston Bowel Preparation Scale scores provide a standardized definition of adequate for describing bowel cleanliness[J].Gastrointest Endosc, 2014, 80(2): 269-276.
[7]中华医学会消化病学分会胃肠动力学组, 中华医学会外科学分会结直肠肛门外科学组. 中国慢性便秘诊治指南(2013,武汉)[J]. 胃肠病学, 2013, 18(10): 605-612.
[7]Gastrointestinal Dynamics Group, Chinese Society of Gastroenterology,Chinese Medical Association; Colorectum and Anus Surgery Group, Chinese Society of Surgery, Chinese Medical Association.Guidelines for the diagnosis and treatment of chronic constipation in China (2013, Wuhan)[J]. Chin J Gastroenterol, 2013, 18(10):605-612. Chinese
[8]中华医学会消化内镜学分会. 中国消化内镜诊疗相关肠道准备指南(草案)[J]. 胃肠病学, 2014, 19(6): 354-356.
[8]Digestive Endoscopy Society of Chinese Medical Association.Guidelines for the diagnosis and treatment of digestive endoscopic bowel preparation (draft)[J]. Chin J Gastroenterol, 2014, 19(6):354-356. Chinese
[9]FANG J, FU H Y, MA D, et al. Constipation, fiber intake and non-compliance contribute to inadequate colonoscopy bowel preparation: a prospective cohort study[J]. J Dig Dis, 2016, 17(7):458-463.
[10]ROTONDANO G, RISPO A, BOTTIGLIERI M E, et al. Quality of bowel cleansing in hospitalized patients undergoing colonoscopy:A multicentre prospective regional study[J]. Dig Liver Dis, 2015,47(8): 669-674.
[11]SHARMA V K, CHOCKALINGHAM S K, UGHEOKE E A, et al. Prospective, randomized, controlled comparison of the use of polyethylene glycol electrolyte lavage solution in four-liter versus two-liter volumes and pretreatment with either magnesium citrate or bisacodyl for colonoscopy preparation[J]. Gastrointest Endosc,1998, 47(2): 167-171.
[12]林炜炜, 顾立扬, 任玲, 等. 低剂量聚乙二醇联合硫酸镁用于肠道准备的效果评价 [J]. 胃肠病学, 2012, 17(1): 10-13.
[12]LIN W W, GU L Y, REN L, et al. Evaluation of low-dose polyethylene glycol combined with magnesium sulfate in bowel preparation[J]. Chin J Gastroenterol, 2012, 17(1): 10-13. Chinese
[13]谢飚, 李瑜元, 吴琼, 等. 伊托必利联合聚乙二醇在便秘患者结肠镜肠道准备中的效果[J]. 广州医学院学报, 2014, 43(3):80-83.
[13]XIE B, LI Y Y, WU Q, et al. Combined use of itopride and polyethylene glycol for colonoscopy preparation before endoscopy examination in constipated patients[J]. Academic Journal of Guangzhou Medical College, 2014, 43(3): 80-83.Chinese
[14]郭雪艳, 牛建平, 廉小延, 等. 复方聚乙二醇电解质散联合莫沙必利在便秘患者行结肠镜检查前肠道准备中应用观察[J].陕西医学杂志, 2013, 42 (3): 370-371.
[14]GUO X Y, NIU J P, LIAN X Y, et al. Combined use of mosapride and polyethylene glycol for colonoscopy preparation before endoscopy examination in constipated patients[J]. Shaanxi Medical Journal, 2013, 42 (3): 370-371. Chinese
[15]丁祥武, 莫慧琴, 杨雨, 等. 莫沙必利对聚乙二醇电解质散溶液用于结肠清洁的影响[J]. 中国内镜杂志, 2011, 17(10):1019-1023.
[15]DING X W, MO H Q, YANG Y, et al. The effects of mosapride on polyethylene glycol electrolyte solution for colonic cleansing[J].China Journal of Endoscopy, 2011, 17(10):1019-1023. Chinese
[16]陆娟, 曹勤, 王晓春, 等. 乳果糖口服液联合聚乙二醇电解质散剂在便秘患者行结肠镜检查前肠道准备中的应用研究[J].现代生物医学进展, 2015, 15(20): 3920-3922.
[16]LU J, CAO Q, WANG X C, et al. Application of lactulose oral solution combined with polyethylene glycol electrolyte powder to bowel preparation of patients with constipation before colonoscopy[J]. Progress in Modern Biomedicine, 2015, 15(20):3920-3922. Chinese
[17]黄衔, 钟志旭, 林少斌. 四磨汤联合聚乙二醇在便秘患者结肠镜前肠道准备的效果观察[J]. 现代消化及介入诊疗, 2016,21(2): 258-260.
[17]HANG X, ZHONG Z X, LIN S B. Application of Simotang oral solution combined with polyethylene glycol electrolyte powder to bowel preparation of patients with constipation before colonoscopy[J]. Modern Digestion & Intervention, 2016, 21(2):258-260. Chinese
[18]赵素平, 姚溪, 张健, 等. 肠道水疗联合复方聚乙二醇电解质散在慢性便秘患者结肠镜检查前肠道准备中的临床疗效[J].中国医学前沿杂志:电子版, 2016, 8(9): 129-132.
[18]ZHAO S P, YAO X, ZHANG J, et al. The efficacy of colon hydrotherapy combined with compound polyethylene glycol electrolyte in bowel preparation of patients with chronic constipation colonscopy[J]. Chin J Front Med Sci: Electronic Edition, 2016, 8(9): 129-132. Chinese
[19]阿秀梅, 严秀莲. 聚乙二醇电解质散剂联合硫酸镁行便秘病人肠道准备效果观察[J]. 实用医学杂志, 2007, 23(11): 1731-1732.
[19]A X M, YAN X L. Evaluation of polyethylene glycol combined with magnesium sulfate in bowel preparation[J]. The Journal of Practical Medicine, 2007, 23(11): 1731-1732. Chinese
[20]孟小芬, 陈熹, 杨屹, 等. 服药时间对结肠镜检查肠道准备效果的影响[J]. 中国内镜杂志, 2016, 22(11): 21-23.
[20]MENG X F, CHEN X, YANG Y, et al. Impact of timing of medicine-taking on bowel preparation for colonoscopy[J]. China Journal of Endoscopy, 2016, 22(11): 21-23. Chinese
(彭薇 编辑)
Effect of modified bowel preparation in patients with constipation undergoing colonoscopy
Le Lu, Xiao-fen Meng, Ping-min Qu, Yu-hua Bai, Hua Li, Xin Xu
(Department of General Surgery, the Second Affiliated Hospital of Xi’an Jiaotong University,Xi’an, Shaanxi 710004, China)
ObjectiveTo evaluate the effect of modified bowel preparation-Polyethylene Glycol Electrolytes Powder (SF-PEG, Shu Taiqing) in combination with magnesium sulfate in patients with constipation undergoing colonoscopy.MethodsSixty cases from mild to moderate constipation were randomly divided into two groups:Group A: SF-PEG (438.4 g, 4 L), 30 cases; Group B:
low-dose SF-PEG (219.2 g, 2 L) and 50.00%magnesium sulfate 50 ml, and then 250 ml water, 30 cases. Boston Bowel Preparation Scale scores (BBPS) and bubbles in bowel lumen score were assessed by the same endoscopist blindly to the preparation regimen, and the time of colonoscopy and the tolerability was recorded.ResultsAll patients underwent completely the bowel preparation and colonoscopy. The time of colonoscopy of group B was shorter than that of group A (P < 0.05).The BBPS score of group B was higher than that of group A (P < 0.05). The bubbles in bowel lumen were less in Group B than in Group A (P < 0.05). The willingness to retake in Group B were superior to those in Group A(P < 0.05). No significant difference was found in score of total adverse effects and taste score between the two groups (P > 0.05).ConclusionSF-PEG in combination with magnesium sulfate in patients with constipation for colonoscopy can improve tolerance to bowel preparation, cleanliness and effects of examination. It’s safe to be recommended in clinical practice.
polyethylene glycol electrolytes powder; magnesium sulfate; constipation; colonoscopy; bowel preparation
R656.9
A
10.3969/j.issn.1007-1989.2017.07.007
1007-1989(2017)07-0030-05
2017-01-09
孟小芬,E-mail:Meng6810@126.com;Tel:13488465698
