生存资料的二次研究系列之六:多元Meta分析模型在重复测量结局Meta分析中的应用
2016-08-22孟详喻田国祥周新雨孙竹李胜曾宪涛
孟详喻,田国祥,周新雨,孙竹,李胜,曾宪涛
·循证理论与实践·
生存资料的二次研究系列之六:多元Meta分析模型在重复测量结局Meta分析中的应用
孟详喻1,2,田国祥3,周新雨4,孙竹5,李胜1,2,曾宪涛1,2
目的 重复测量资料是医学研究尤其是预后相关研究中重要的资料类型之一。不同时间点重复测量值之间存在相关性,若在二次研究如Meta分析中分开分析的结果可能存在偏倚,采用多元Meta分析模型能够有效避免因分开分析而导致的偏倚。本文介绍使用多元Meta分析模型合并多个二分类重复测量结局的方法,并通过实例分析演示如何在R软件中实现。
多元Meta分析模型;重复测量结局;Meta分析;预后
预后指标是医学研究及临床实践中非常重要的一类指标,预后研究的系统评价/Meta分析是预后相关研究资料汇总及循证实践的基础[1,2]。在预后相关的医学研究中,除了时间-事件资料(time-to-event,TTE)之外还有一类重要的研究资料类型,即重复测量资料(例如:术后1个月、3个月与6个月时某手术并发症的发生率,治疗开始后1周、4周与8周时某药物相关不良事件的发生率)。这类重复测量资料又称纵向数据,不同于TTE资料,一般没有长期的定期随访,而是在某些特定时间点对样本进行测量与数据收集,一般没有大量的删失。另一方面,由于各时点的测量值基于同一样本,故其相互之间存在关联,若分开进行Meta分析则会造成信息的重复利用而使合并结果出现偏倚[3-6]。在本系列的上一篇文章中,我们介绍了以三级Meta分析模型合并多个非独立TTE结局的方法[7]。本文介绍以多元Meta分析模型合并多个二分类重复测量结局的方法,并通过实例分析演示如何利用R软件实现。
1 多元Meta分析模型简介
在多个结局指标存在关联的情况下,以传统Meta分析方法分开合并可能造成结果偏倚。在结局间关联信息可知的情况下,即结局间抽样协方差矩阵可知的情况下,以多元Meta分析模型进行合并能避免上述问题[3-6]。
鉴于固定效应模型是随机效应模型的降维,故在此以多元随机效应模型为例进行介绍。多元随机效应Meta分析模型可以表示为:

2 二分类重复测量结局的效应量与抽样协方差矩阵的估计
以多元Meta分析模型进行分析前要求各结局指标的效应量与抽样协方差矩阵已知[3-6]。接下来,以二分类重复测量结局为例,以某试验组样本为对象进行具体说明。因结局类型为二分类重复测量结局,分析对象为单个试验组样本,则对数几率为首选效应量。假设试验组内事件的发生服从强度函数为λ(t)的非齐次泊松过程。假设大规模人群中事件的发生服从泊松分布,起始时刻λ(t0)=λ0,起始样本为N0,时刻t前已累积发生事件数为Ct,时刻t后某极小时间段△t内,有:

假定该组受试者样本总量恒定为N,时间点tn(n≥1)所对应的累积事件数为Cn,则时间点tn相应的对数几率为:

根据delta法[8],其抽样方差近似为:

则任意两测量时间点tm与tn(1≤m<n)相应的对数几率log odds tm与log odds tn的抽样协方差为:

因Cm、Cn(1≤m<n)为泊松随机变量,令c为任意常数,根据delta法,结合(2.1),有:

综合(2.4)、(2.5)、(2.6)、(2.7)与(2.8),则有:

综合(2.3)、(2.9)不难推导出抽样协方差矩阵。因篇幅有限,在此不做进一步说明。
上述公式推导基于样本总量N保持恒定这一假设,即没有出现受试者失访、退出研究等情形。但在实际的重复测量研究过程中,随访期内样本量因受试者失访、退出研究等因素而出现减少的情况十分常见。若文献报告了不同时间点的样本量信息,记时间点tm与tn(1≤m<n)所对应的样本量分别为Nm与Nn(Nn≤Nm≤N),则有:
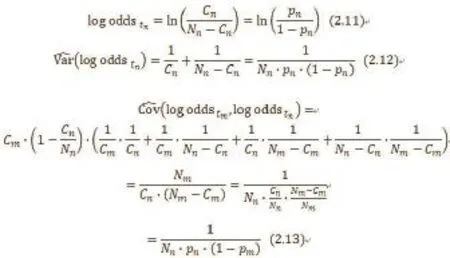
根据(2.11)、(2.12)与(2.13)可以计算得出相应的效应量与协方差矩阵。若文献没有对不同时间点的样本量进行报告,在失访率很低的情况下因Nn≈Nm≈N,则可以利用(2.2)、(2.3)与(2.10)进行估算;若失访率较高,则需联系原始研究作者获取不同时间点的样本量信息,若无法获取则建议通过其他方式进行估算或放弃多元Meta分析合并。
3 实例分析
3.1数据来源及原始数据表 实例分析的数据来自一篇比较开放式(RRP)、腹腔镜(LRP)与机器人辅助(RARP)前列腺癌根治术后功能结局的Meta分析[9]。本实例节选术后6个月与12个月尿控恢复的结局指标,原始数据表中的部分数据如表1所示。共纳入33项研究的数据[10-42],完整的Excel数据表请读者自行前往武汉大学中南医院循证与转化医学中心官网(http://www.whuzncebtm. com/)的“资料下载”一栏进行下载。根据(2.11)、(2.12)与(2.13),以试验组为单位将原始数据转化为效应量即术后6个月与12个月的对数几率、二者的抽样方差及协方差(部分研究存在事件数等于总人数的情况,将事件数减0.5作连续性校正),部分数据如表2所示,完整的Excel数据表请读者自行前往武汉大学中南医院循证与转化医学中心官网的“资料下载”一栏进行下载。表中的“study_id”、“author”、“treatment”为研究编号、第一作者姓与手术方案,“y1”、“v_y1”、“y2”、“v_y2”分别为6个月尿控恢复与12个月尿控恢复结局的对数几率与抽样方差,“cov_y1_y2”为两结局指标的抽样协方差。
3.2多元Meta分析 首先以对比RRP与LRP的研究为例进行分析说明。分析所用软件为R软件和metaSEM程序包。
涉及RRP与LRP直接比较的研究共14项[10-23]。将该部分数据读入R软件存入对象“dat1”,之后输入如下命令进行分析与结果展示(#后为命令释义):

表1 实例分析的部分原始数据表

表2 转化后的部分原始数据表

library(metaSEM) #载入metaSEM程序包x1<-as.numeric(dat1$treatment)-1#构建哑变量x1,RRP赋值1,LRP赋值0;summary(meta(y=cbind(y1, y2),v=cbind(v_y1, cov_y1_y2, v_y2),x=x1, data=dat1, RE.startvalues = 0.5))#进行多元meta分析并显示结果,结果中“Intercept1”与“Intercept2”分别为LRP组术后6个月与12个月尿控恢复率的对数几率,“Slope1_1”与“Slope2_1”则为RRP组比LRP组的对数几率比即log OR;summary(meta(y=cbind(y1, y2),v=cbind(v_y1, cov_y1_y2, v_y2),x=x2, data=dat1, RE.startvalues = 0.5))#进行多元meta分析并显示结果,结果中“Intercept1”与“Intercept2”分别为RRP组术后6个月与12个月尿控恢复的对数几率,“Slope1_1”与“Slope2_1”则为LRP组比RRP组的对数几率比即log OR;
根据分析结果,可得出LRP组术后6个月尿控恢复的几率及其95%置信区间(95%CI)为1.71(1.09,2.70),术后12个月尿控恢复几率及其95%CI为4.34(2.44,7.71);RRP组术后6个月尿控恢复的几率及其95%CI为2.09(1.32,3.31),术后12个月则为4.43(2.49,7.91);LRP组比RRP的尿控恢复的几率比OR及其95%CI在术后6个月为0.82(0.43,1.56),术后12个月为0.98 (0.43,2.22)。异质性方面,LRP组术后6个月与12个月尿控恢复几率Meta分析的I2分别为0.9285与0.9449,RRP组I2为0.8774与0.8900,两组比较OR的I2分别为0.7342 与0.7709。异质性Q检验的P值均小于0.001。
接着以类似的操作对比较RRP与RARP的9项研究进行分析[24-32]。结果显示,RARP组术后6个月尿控恢复的几率及其95%CI为7.48(4.21,13.29),12个月为14.00(8.05,24.37);RRP组术后6个月尿控恢复的几率及其95%CI为4.28 (2.51,7.30),12个月为6.71(4.08,11.01)。RARP组相比RRP组的OR及其95%CI在6个月及12个月分别为1.75(0.80,3.83)及2.09(0.99,4.39)。
接下来以类似的操作对比较LRP与RARP的11项研究进行分析[28,33-42]。结果显示,LRP组术后6个月尿控恢复的几率及其95%CI为2.40(1.64,3.50),12个月为4.76(2.77,8.19);RARP组术后6个月尿控恢复的几率及其95%CI为5.37 (3.60,8.01)与9.03(5.14,15.88);RARP组相比LRP组的OR及其95%CI在6个月及12个月分别为2.24(1.30,3.87)及1.90(0.90,4.04)。
3.3扩展分析 在上述分析过程中,我们以多元Meta分析模型对RRP、LRP与RARP进行了头对头Meta分析。为深入比较三种手术的优劣,接下来以两种完全不同的方法进行后续拓展分析,并将扩展分析的结果汇总整理为森林图。
3.3.1直接比较与间接比较数据的合并 研究内不同手术组相互独立,不同研究间相互独立,则LRP组比RRP组对数OR的间接比较数据等于RARP组比RRP组的对数OR值减去RARP组比LRP组的对数OR,而抽样方差与协方差则为二者之和。其他组的间接比较数据求法与之相同。将直接比较合并结果与间接比较合并结果整理成表,如表3所示。Meta分析结果森林图见图1。异质性I2=0.01,Q检验P=0.8576,说明各直接与间接合并结果的同质性好。术后6个月与12个月指标研究间随机效应的相关系数为0.9666,说明二者高度正相关。
3.3.2三级Meta分析模型全局分析
构建三个哑变量x1、x2与x3,所用三级meta模型的基本形式如下:
第一级:yij=θij+eij
第二级:θij= fj+ u(2)ij
第三级:fj= β1·x1+β2·x2+β3·x3+u(3)j
其中fj代表研究j的整合了6个月与12个月指标(尿控恢复对数几率)的综合结局。分别令LRP、RARP与RRP对应的哑变量取值为向量(1,0,0)、(0,1,0)与(0,0,1),则β1、β2与β3分别对应LRP组、RARP组与RRP组的综合结局的合并值。以33项纳入研究的全体数据进行上述三级Meta分析[10-42],具体操作方法请参见本系列上一篇文献[7]。分析结果显示,Q检验P=0,τ2(2)与τ2(3)分别为0.32与0.42。β1、β2与β3的点估计分别为1.29、2.17与1.41,β1、β2与β3的协方差矩阵如表4所示。基于上述参数的点估计与协方差矩阵计算两两比较的对数OR及其标准误,以LRP比RRP为例,算式如下:
最后在(3.3.2.1)与(3.3.2.2)的基础上计算出相应的OR及其95%CI,结果森林图如图1所示。
4 结语
由于重复测量结局间存在相关性,如果以传统方式分开进行Meta分析会因信息的重复利用而导致结果出现偏倚。多元Meta分析模型避免了信息的重复利用因而能对这一偏倚进行校正。除了TTE资料之外,重复测量资料在预后相关研究中占有重要地位。建议广大二次研究者在针对重复测量结局指标进行Meta分析时尽可能使用多元Meta分析模型。由于三级Meta分析模型属于多元Meta分析模型的近似与特例,在结局指标间协方差矩阵无法获取情况下建议使用三级Meta模型。
[1] 孟详喻,田国祥,仇成凤,等. 生存资料的二次研究系列之三: 预后相关的二次研究的基本概念介绍[J]. 中国循证心血管医学杂志,2016,18(3):in press.
[2] 孟详喻,方程,田国祥,等. 生存资料的二次研究系列之四: 预后相关系统评价/Meta分析的文献计量学研究[J]. 中国循证心血管医学杂志,2016,18(4): in press.
[3] Tinsley HEA,Brown ED. Handbook of applied multivariate statistics and mathematical modeling[M]. Orlando: Academic Press,2000.
[4] Berkey CS,Anderson JJ,Hoaglin DC. Multiple-outcome meta-analysis of clinical trials[J]. Stat Med,1996,15(5):537-57.
[5] Arends LR,Vokó Z,Stijnen T. Combining multiple outcome measures in a meta-analysis: an application[J]. Stat Med,2003,22(8):1335-53.
[6] Berkey CS,Hoaglin DC,Antczak-Bouckoms A,et al. Meta-analysis of multiple outcomes by regression with random effects[J]. Stat Med,1998,17(22):2537-50.
[7] 孟详喻,周新雨,李胜,等. 生存资料的二次研究系列之五: 三级随机效应Meta分析模型在预后相关Meta分析中的应用[J]. 中国循证心血管医学杂志,2016,18(5): in press.
[8] Agresti A. Categorical Data Analysis, (2nd edn)[M]. New York:John Wiley & Sons,2002.
[9] Shi MJ,Yang J,Meng XY,et al. Comparison of functional outcomes after retropubic, laparoscopic and robot-assisted radical prostatectomy: A meta-analysis[J]. World J Meta-Anal, 2014,2(3):107-26.
[10] Anastasiadis AG,Salomon L,Katz R,et al. Radical retropubic versus laparoscopic prostatectomy:a prospective comparison of functional outcome[J]. Urology,2003,62(2): 292-7.
[11] Roumeguere T,Bollens R,VandenBossche M,et al. Radical prostatectomy: a prospective comparison of oncological and functional results between open and laparoscopic approaches[J]. World J Urol,2003,20(6):360-6.
[12] Remzi M,Klingler HC,Tinzl MV,et al. Morbidity of laparoscopic extraperitoneal versus transperitoneal radical prostatectomy verus open retropubic radical prostatectomy[J]. Eur Urol, 2005,48(1):83-9.
[13] Wagner AA,Link RE,Trock BJ,et al. Comparison of open and laparoscopic radical prostatectomy outcomes from a surgeon's early experience[J]. Urology,2007,70(4):667-71.
[14] Touijer K,Eastham JA,Secin FP,et al. Comprehensive prospective comparative analysis of outcomes between open and laparoscopic radical prostatectomy conducted in 2003 to 2005[J]. J Urol,2008,179(5):1811-7.
[15] Greco F,Wagner S,Hoda MR,et al. Laparoscopic vs open retropubicintrafascial nerve-sparing radical prostatectomy:surgical and functional outcomes in 300 patients[J]. BJU Int,2010, 106(4):543-7.
[16] Dahl DM,Barry MJ,McGovern FJ,et al. A prospective study of symptom distress and return to baseline function after open versus laparoscopic radical prostatectomy[J]. J Urol,2009,182(3): 956-65.
[17] Egawa S,Kuruma H,Suyama K,et al. Delayed recovery of urinary continence after laparoscopic radical prostatectomy[J]. Int J Urol,2003,10(4):207-12.
[18] Artibani W,Grosso G,Novara G,et al. Is laparoscopic radical prostatectomy better than traditional retropubic radical prostatectomy?An analysis of peri-operative morbidity in two contemporary series in Italy[J]. Eur Urol,2003,44(4):401-6.
[19] Ghavamian R,Knoll A,Boczko J,et al. Comparison of operative and functional outcomes of laparoscopic radical prostatectomy and radical retropubic prostatectomy: single surgeon experience[J]. Urology,2006,67(6):1241-6.
[20] Takenaka A,Soga H,Kurahashi T,et al. Early recovery of urinary continence after laparoscopic versus retropubic radical prostatectomy:evaluation of preoperative erectile function and nerve-sparing procedure as predictors[J]. Int Urol Nephrol,2009,41(3):587-93.
[21] Simforoosh N,Javaherforooshzadeh A,Aminsharifi A,et al. Early continence after open and laparoscopic radical prostatectomy with suturelessvesicourethralalignment:an alternative technique, 8 years' experience[J]. Urol J,2009,6(3):163-9.
[22] Springer C,Inferrera A,Pini G,et al. Laparoscopic versus open bilateral intrafascial nerve-sparing radical prostatectomy after TUR-P for incidental prostate cancer: surgical outcomes and effect on postoperative urinary continence and sexual potency[J]. World J Urol,2013,31(6):1505-10.
[23] Magheli A,Busch J,Leva N,et al. Comparison of surgical technique (open vs. laparoscopic) on pathological and long term functional outcomes following radical prostatectomy[J]. BMC Urol,2014,14(2):18.
[24] Krambeck AE,DiMarco DS,Rangel LJ,et al. Radical prostatectomy for prostatic adenocarcinoma: a matched comparison of open retropubic and robot-assisted techniques[J]. BJU Int,2009,103(4):448-53.
[25] Ficarra V,Novara G,Fracalanza S,et al. A prospective, nonrandomized trial comparing robot-assisted laparoscopic and retropubic radical prostatectomy in one European institution[J]. BJU Int,2009,104(4):534-9.
[26] Ham WS,Park SY,Kim WT,et al. Open versus robotic radical prostatectomy: a prospective analysis based on a single surgeon's experience[J]. J Robotic Surg,2008,2(4):235-41.
[27] Geraerts I,Van Poppel H,Devoogdt N,et al. Prospective evaluation of urinary incontinence, voiding symptoms and quality of life after open and robot-assisted radical prostatectomy[J]. BJU Int,2013,112(7):936-43.
[28] Caballero Romeu JP,Palacios Ramos J,Pereira Arias JG,et al. Radical prostatectomy: evaluation of learning curve outcomes laparoscopic and robotic-assisted laparoscopic techniques with radical retropubic prostatectomy[J]. Actas Urol Esp,2008,32(10):968-75.
[29] Rocco B,Matei DV,Melegari S,et al. Robotic vs open prostatectomy in a laparoscopically naive centre: a matched-pair analysis[J]. BJU Int,2009,104(7):991-5.
[30] Ou YC,Yang CR,Wang J,et al. Comparison of robotic-assisted versus retropubic radical prostatectomy performed by a single surgeon[J]. Anticancer Res,2009,29(5):1637-42.
[31] Choo MS,Choi WS,Cho SY,et al. Impact of prostate volume on oncological and functional outcomes after radical prostatectomy:robot-assisted laparoscopic versus open retropubic[J]. Korean J Urol,2013,54(1):15-21.
[32] Son SJ,Lee SC,Jeong CW,et al. Comparison of Continence Recovery Between Robot-Assisted Laparoscopic Prostatectomy and Open Radical Retropubic Prostatectomy: A Single Surgeon Experience[J]. Korean J Urol,2013,54(9):598-602.
[33] Asimakopoulos AD,Pereira Fraga CT,AnninoF,et al. Randomized comparison between laparoscopic and robot-assisted nerve-sparing radical prostatectomy[J]. J Sex Med,2011,8(5): 1503-12.
[34] Porpiglia F,Morra I,LucciChiarissi M,et al. Randomised controlled trial comparing laparoscopic and robot-assisted radical prostatectomy[J]. Eur Urol,2013,63(4):606-14.
[35] Ploussard G,de la Taille A,Moulin M,et al. Comparisons of the perioperative,functional, and oncologic outcomes after robot-assisted versus pure extraperitoneal laparoscopic radical prostatectomy[J]. Eur Urol,2014,65(3):610-9.
[36] Joseph JV,Vicente I,Madeb R,et al. Robotassistedvs pure laparoscopic radical prostatectomy: are there any differences?[J]. BJU Int,2005,96(1):39-42.
[37] Lee HW,Lee HM,Seo SI. Comparison of initial surgical outcomes between laparoscopic radical prostatectomy and robot-assisted laparoscopic radical prostatectomy performed by a single surgeon[J]. Korean J Urol,2009,50(5):468-74.
[38] Cho JW,Kim TH,Sung GT. Laparoscopic radical prostatectomy versus robot-assisted laparoscopic radical prostatectomy: a single surgeon's experience[J]. Korean J Urol,2009, 50(12):1198-202.
[39] Hakimi AA,Blitstein J,Feder M,et al. Direct comparison of surgical and functional outcomes of robotic-assisted versus pure laparoscopic radical prostatectomy:single-surgeon experience[J]. Urology,2009,73 (1):119-23.
[40] Trabulsi EJ,Zola JC,Gomella LG,et al. Transition from pure laparoscopic to robotic-assisted radical prostatectomy: a single surgeon institutional evolution[J]. Urol Oncol,2011,28(1):81-5.
[41] Park JW,Won Lee H,Kim W,et al. Comparative assessment of a single surgeon's series of laparoscopic radical prostatectomy: conventional versus robot-assisted[J]. J Endourol,2011, 25(4):597-602.
[42] Park B,Kim W,Jeong BC,et al. Comparison of oncological and functional outcomes of pure versus robotic-assisted laparoscopic radical prostatectomy performed by a single surgeon[J]. Scand J Urol,2013,47(1):10-8.
本文编辑:姚雪莉
Application of multivariate Meta-analytical model in Meta-analysis of repeated measures outcomes
MENG Xiang-yu*, TIAN Guo-xiang, ZHOU Xin-yu, SUN Zhu, LI Sheng, ZENG Xian-tao. *Center for Evidence-Based and Translational Medicine, Zhongnan Hospital, Wuhan University, Wuhan 430071, China.
ZENG Xian-tao, E-mail: zengxiantao1128@163.com
Repeated measures data are one of major data types in medical studies, especially in those related to prognosis. Correlation exists among multiple measures values corresponding to different time points, thus separate analyses for single outcome in secondary studies, e.g. Meta-analysis, should be avoided since bias might be introduced and the multivariate Meta-analysis model which well manages dependence across effect sizes is recommended. In this article, a multivariate Meta-analytical model was presented to merge multiple binary repeated measures outcomes, as well as actualized in R software through example analysis.
Multivariate Meta-analytical model; Repeated measures outcomes; Meta-analysis; Prognosis
R4
A
1674-4055(2016)06-0647-05
1430071 武汉,武汉大学中南医院循证与转化医学中心;2430071 武汉,武汉大学循证与转化医学中心;3100700 北京,陆军总医院干四科;4400016 重庆,重庆医科大学第一附属医院神经内科;5100700 北京,陆军总医院心血管病研究所
曾宪涛,E-mail:zengxiantao1128@163.com.
10.3969/j.issn.1674-4055.2016.06.03
由于存在不同研究的结局指标报道不尽相同的情况,以X与Z两个选择矩阵过滤缺失的结局指标信息。y、u与e分别为各结局指标效应量、随机效应和抽样误差组成的向量。对任一研究i,其随机效应向量ui~N(0,T2),其中T2为p×p非负定矩阵。多元Meta分析模型的理论较为复杂,在此不进一步展开讨论。有兴趣的读者请自行参阅相关文献[3-6]。
