盐酸美金刚联合盐酸多奈哌齐对中重度阿尔茨海默病患者精神行为症状的疗效观察
2013-04-18杨华郭忠伟李霞张江涛冯斌
杨华 郭忠伟 李霞 张江涛 冯斌
盐酸美金刚联合盐酸多奈哌齐对中重度阿尔茨海默病患者精神行为症状的疗效观察
杨华 郭忠伟 李霞 张江涛 冯斌
目的 评价盐酸美金刚联合盐酸多奈哌齐对阿尔茨海默病(AD)伴发精神行为症状(BPSD)的疗效及安全性。 方法 将符合标准的80例AD患者随机分为研究组和对照组,每组40例,治疗组患者服用盐酸美金刚和盐酸多奈哌齐,对照组患者单用盐酸多奈哌齐。盐酸美金刚起始剂量为5mg/d,每周递增5mg,4周末增至20mg/d;盐酸多奈哌齐起始剂量为5mg/d,4周末增至10mg/d;观察12周。治疗前及治疗12周末,分别采用痴呆行为量表(BEHAVE-AD)评价精神行为症状、日常生活能力量表(ADL)判定患者日常生活活动能力、临床总体印象量表(CGI)评定患者总体变化情况。 结果 治疗12周末,研究组BEHAVE-AD减分较对照组更显著(8.1±3.30, 9.2±2.80,t=-3.317,P<0.01),ADL减分更显著(28.1±2.35,29.3±2.63,t=2.097,P<0.05),CGI评分分别为(3.43±0.82和4.37± 0.85),差异有统计学意义(t=-5.413,P<0.01)。 结论 盐酸美金刚联合盐酸多奈哌齐治疗BPSD的疗效优于单用盐酸多奈哌齐。
阿尔茨海默病 精神和行为症状 盐酸多奈哌齐 盐酸美金刚
痴呆的行为和心理症状(Behavioral and psychological symptoms of dementia,BPSD)决定着患者及照料者的生活质量,同时也构成了照料者的主要应激来源,也是患者住院的主要原因[1],由于典型或非典型抗精神病药物可大大增加阿尔茨海默病(Alzheimer Disease,AD)患者的心血管事件风险[2],故限制了其在临床上的应用。盐酸多奈哌齐为乙酰胆碱酯酶抑制剂(acetylcholinesterase inhibitor,AChEI),可逆性抑制脑中乙酰胆碱酯酶的活性而增加神经递质乙酰胆碱的浓度,一定程度上控制BPSD[3]。盐酸美金刚是N-甲基-D-天冬氨酸(N-methyl-D-aspartic acid receptor,NMDA)受体拮抗剂,通过非竞争性阻断NMDA受体,降低谷氨酸引起的NMDA受体过度兴奋,对妄想、激越、易激惹有较好疗效[4]。本文旨在观察两药联用治疗BPSD疗效。
1 资料和方法
1.1 一般资料 2009至2011年入住我院老年科的AD患者80例。入组标准:(1)符合美国神经病学会、语言障碍和卒中-老年性痴呆和相关疾病学会(The Alzheimer’s Disease and Related DisordersAssociation,NINCDS/ ADRDA)制定的AD“可能”诊断标准[5];(2)年龄65~80岁;(3)简易精神状态检查(Mini-mental state examination,MMSE):5~12分;(3)Hachinski缺血量表(Hachinski Inchemic Score,HIS)评分≤4分;(4)痴呆行为量表(BEHAVE-AD)评分≥8分[6];(5)头颅CT或MR示脑萎缩;(6)入组前4周未服用盐酸多奈哌齐(商品名:安理申,日本卫材(中国)药业有限公司)和盐酸美金刚(商品名:易倍申,丹麦灵北公司)。排除标准:(1)伴有严重的躯体疾病,合并心、肝、肾和造血系统等严重原发性疾病;(2)过敏体质及对胆碱类药物、盐酸美金刚过敏者;(3)其他疾病引起的痴呆。组间性别构成、年龄、病程以及受教育程度等差异均无统计学意义。80例患者采用随机数字表法分为服用盐酸美金刚联合盐酸多奈哌齐组(治疗组)与盐酸多奈哌齐组(对照组)。两组患者一般情况比较见表1。

表1 两组患者一般情况比较
由表1可见,两组患者一般情况差异均无统计学意义(均P>0.05)。
1.2 方法
1.2.1 服药方法 盐酸美金刚第1周为每天5mg(晨服),第2周每天10mg(每次5mg,2次/d),第3周每天15mg(早上10mg,下午5mg),第4周开始以后服用维持剂量每天20mg(每次10mg,2次/d);盐酸多奈哌齐起始剂量为5mg/d,4周末增至10mg/d。观察时间为12周。
1.2.2 评定方法 分别于治疗前与治疗后第12周末采用痴呆行为量表(BEHAVE-AD)评价精神行为。BEHAVE-AD共有25项条目,包含偏执和妄想观念、幻觉、行为紊乱、攻击行为、日夜节律紊乱、情感障碍、焦虑和恐惧7个分量表,每项条目按症状严重程度为0~3分,4级评分。另外,还有一项总评条目,按总体印象为0~3分,4级评分)。日常生活能力量表(Activies of daily living,ADL)用于判定患者日常生活活动能力。临床总体印象量表(Clinical Global Impression,CGI)评定患者总体变化情况。每周对药物不良反应采用药物不良反应作用量表(Treatment Emergent Symptom Scale,TESS)评价。治疗前及治疗后每2周复查血常规、生化常规和心电图。由2位不知分组治疗情况的评定者分别作评定。1.2.3 统计学处理 采用SPSS15.0软件处理。计量资料用表示,组间比较采用t检验。
2 结果
2.1 两组AD患者治疗前后BEHAVE-AD评分比较见表2。
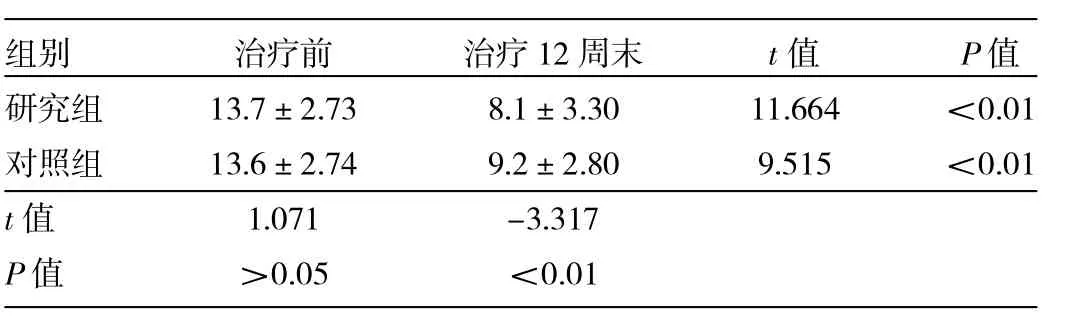
表2 两组AD患者治疗前后BEHAVE-AD评分比较
由表2可见,治疗后两组AD患者BEHAVE-AD评分均有明显下降,但研究组下降更明显。
2.3 两组AD患者治疗前后ADL评分比较 见表3。
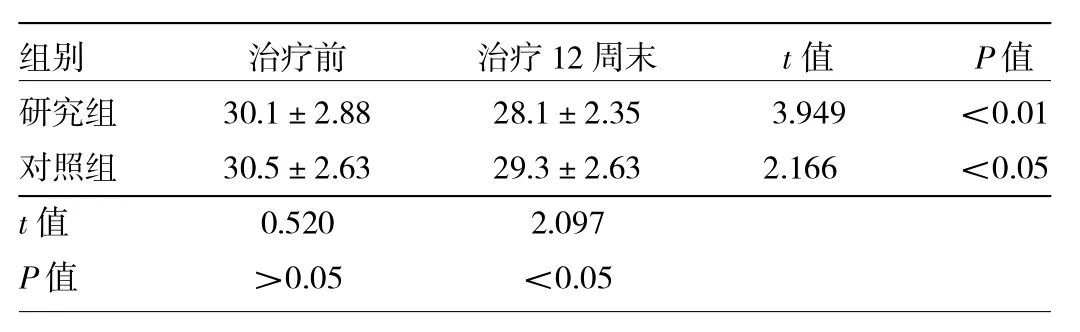
表3 两组AD患者治疗前后ADL评分比较
由表3可见,治疗后两组AD患者ADL评分均有明显下降,但研究组下降更明显。
2.4 两组AD患者治疗12周末CGI评分比较 治疗12周末研究组和对照组CGI评分分别为3.43±0.82和4.37±0.85,差异有统计学意义(t=-5.413,P<0.01)。
2.5 两组AD患者不良反应比较 两组发生不良发生率相近,症状均轻微,差异无统计学意义(P>0.05),见表4。

表4 两组AD患者不良反应比较(例)
3 讨论
BPSD的发病机制复杂,与病前性格、不同脑区脑结构改变、代谢异常和神经递质失调有关[7-8]。临床对BPSD药物治疗分为病因与对症治疗。研究显示,AChEI和NMDA能在一定程度上改善BPSD症状[9-10],但是,AChEI和NMDA在改善BPSD具体临床症状方面各有自己的优势。Gauthier等[11]为了明确盐酸多奈哌齐对中重度痴呆患者精神行为症状的疗效,进行了一项为期24周随机、双盲、安慰剂对照研究,尽管NPI评分降低,但主要体现在抑郁、焦虑、情感淡漠因子,对激越症状没有改善[12]。Gauthier等[13]在一项汇总分析中,发现盐酸美金刚治疗中重度痴呆患者的精神和行为症状,在治疗12、24、48周后,NPI评分明显降低,与安慰剂组比较有统计学差异,尤其是幻觉、妄想、激越、易激惹亚量表评分改善更明显。Wilcock等[14]报道盐酸美金刚对伴有激惹、幻觉或妄想的中重度老年性痴呆患者治疗观察,与安慰剂对照,观察12周、24周、48周,应用美金刚12周末,有55.3%患者症状缓解,24周末有61.0%患者症状缓解,而安慰剂组缓解率分别为44.4%和44.8%,且治疗组激越、幻觉、妄想亚量表评分较安慰剂组有统计学差异。
那么,美金刚联合盐酸多奈哌齐干预BPSD是否有更好临床疗效?本文观察结果显示,治疗12周末,研究组和对照组BEHAVE-AD评分均有明显下降,但研究组下降更明显,与对照组比较差异有统计学意义(P<0.01);CGI评分差异有统计学意义(P<0.01);研究组对ADL改善较对照组更显著(P<0.01)。这说明盐酸多奈哌齐联合盐酸美金刚能进一步改善患者的精神行为症状,提高日常生活能力。分析原因可能如下:(1)盐酸多奈哌齐和盐酸美金刚对BPSD亚症状疗效各有针对性,联合使用后,治疗效果叠加;(2)BPSD是在认知功能障碍背景下大脑功能失调的结果[1]。最近研究显示激越症状与工作记忆密切相关[16],因此改善认知在一定程度上可改善BPSD。研究显示美金刚联合盐酸多奈哌齐较单一应用盐酸多奈哌齐能使认知功能更能进一步获益[17-18];(3)胆碱能神经功能在BPSD发生、发展中起着重要作用[19]。美金刚联合盐酸多奈哌齐较单一应用盐酸多奈哌齐刺激大脑皮质和海马乙酰胆碱的释放更明显[20];(4)正电子发射成像(PET)[21]、磁共振波谱分析技术(MRS)[22]、弥散张量成像(DTI)[23]功能影响学研究发现,BPSD与脑功能关系密切,BPSD亚临床症状与脑区不同代谢物异常或功能相关。而盐酸多奈哌齐和美金刚对AD患者不同脑区功能和代谢物的影响又具有各自特点[25-27]。因此,推断联合应用盐酸多奈哌齐和美金刚较单一使用盐酸多奈哌齐更能全面改善脑功能,从而更有效改善BPSD;(5)激越和精神病性症状与phospho-tau相关[28]。美金刚能减轻phospho-tau[29];(6)BPSD是突触丧失直接作用的结果[30]。NMDA及NMDA受体在神经突触功能丧失过程中起着关键性作用[31]。美金刚能减轻NMDA毒性,盐酸多奈哌齐通过NMDA Receptor调节突触可塑性[33]。因此,盐酸多奈哌齐联合美金刚突触可塑性调节具有协调作用,可能增加对BPSD的治疗作用。
本研究结果显示,联合用药不良反应发生率与单一用药相当,与国外单一用药不良反应基本一致[34]。症状均轻微,经相应对症处理后好转,并没有因不良反应而脱落病例。但观察12周后,研究组BEHAVE-AD评分虽然由治疗前的13.7±2.73降低到8.1±3.30,且减分较对照组显著,但BEHAVE-AD平均分仍>8分,仍有32.5 %(13/40)患者BPSD没有缓解,说明两者联用并不能完全消除BPSD。
[1]沈渔邨主编.精神病学[M].5版.北京:人民卫生出版社,2009:309.
[2]Schneider L S,Dagerman K S,Insel P.Risk of death with atypical antipsychotic drug treatmentfor dementia:meta-analysis of randomized placebo-controlled trials[J].JAMA,2005,294(15): 1934-1943.
[3]Cummings J,Mcrae T,Zhang R.Effects of donepezil on neuropsychiatric symptoms in patients with dementia and severe behavioral disorders[J].Geriatric Psychiatry,2006,14(7):605-612.
[4]Gauthier S,Loft H,Cummings J.Improvement in behavioural symptoms in patients with moderate to severe Alzheimer's disease by memantine:a pooled data analysis[J].Geriatr.Psychiatry, 2008,23:537-545.
[5]盛树力主编.老年性痴呆[M].北京:科学技术文献出版社,1999:3-6.
[6]盛建华,陈美娟,高之旭,等.阿尔茨海默病病理行为评分表信度和效度[J].临床精神医学杂志,2001,11(2):75-77.
[7]McIlroy S,Craig D.Neurobiology and genetics of behavioural syndromes of Alzheimer's disease[J].Curr Alzheimer Res,2004, 1(2):135-142.
[8]Rajesh R,Tampi M D,FAPA M S,et al.Behavioral and Psychological Symptoms of Dementia:PartI-Epidemiology,Neurobiology, Heritability and Evaluation[J].Clinical Geriatrics,2011,5:300-315.
[9]贾建平,王荫华,魏翠.中国痴呆与认知障碍诊治指南(五):痴呆治疗[J].中华医学杂志,2011,91(14):940-945.
[10]Huang Y J,Lin H C,Lane H Y,et al.NMDA Neurotransmission Dysfunction in Behavioral and Psychological Symptoms of Alzheimer's Disease[J].Curr Neuropharmacol,2012,10(3):272-285.
[11]Gauthier S,Feldman H,HeckerJ,et al.Efficacy of donepezil on behavioral symptoms in patients with moderate to severe Alzheimer's disease[J].International Psychogeriatrics,2002,14 (4):389-404.
[12]Howard R J,Juszczak E,Ballard C G,et al.Donepezil for the treatment of agitation in Alzheimer's disease[J].N Engl J Med, 2007,357,1382-1392.
[13]Gauthier S,Loft H,Cummings J.Improvement in behavioural symptoms in patients with moderate to severe Alzheimer's disease by memantine:a pooled data analysis[J].Geriatr.Psychiatry,2008,23:537-545.
[14]Wilcock G,Ballard C,Cooper J.Memantine for agitation/aggres-sion and psychosis in moderately severe to severe Alzheimer's disease:a pooled analysis of 3 studies[J].Clin Psychiatry,2008, 69:341-348.
[15]Margari F,Sicolo M,Spinelli L,et al.Aggressive behavior,cognitive impairment,and depressive symptoms in elderly subjects [J].Neuropsychiatr Dis Treat,2012,8:347-353.
[16]Gauthier S,Molinuevo J L.Benefits of combined cholinesterase inhibitor and memantine treatment in moderate-severe Alzheimer's disease[J].Alzheimers Dement,2012,27(11)03045.
[17]Molinuevo J L,Lemming O.Memantine in patients with Alzheimer's diseasereceiving donepezil:new analyses of efficacy and safety for combination therapy[J].Alzheimer's Research&Therapy,2013,5:6.
[18]Lanaria A,Ament F,iorgio Silvestrelli G,et al.Neurotransmitter deficits in behavioural and psychological symptoms of Alzheimer's disease[J].Dementias and Cognitive Disorders:New Insights and Approaches,2006,127(2):158-165.
[19]Jouni Ihalainena,Timo Saraja rvib,Doug Rasmusson.Effects of memantine and donepezil on cortical and hippocampal acetylcholine levels and object recognition memory in rats[J].Neuropharmacology,2011,61(5-6):891-899.
[20]Cerejeira J,Lagarto L,Mukaetova-Ladinska E B.Behavioral and Psychological Symptoms of Dementia[J].Front Neurol,2012, 3:73.
[21]Shinno H,Inagaki T,Miyaoka T,et al.A decrease in N-acetylaspar-tate and an increase in myoinositol in the anterior cingulate gyrus are associated with behavioral and psychological symptoms in Alzheimers disease[J].Journal of the Neurological Sciences,2007,260:132-138.
[22]Sarah K,Tighe,Kenichi O M.Diffusion Tensor Imaging of Neuropsychiatric Symptoms in Mild Cognitive Impairment and Alzheimer's Dementia[J].The Journal of Neuropsychiatry and Clinical Neurosciences,2012,24:484-488.
[23]Lima T S,Honga Y H,Leeb H Y,et al.Metabolite Investigation in Both Anterior and Posterior Cingulate Gyri in Alzheimer's Disease Spectrum Using 3-Tesla MR Spectroscopy[J].Dement Geriatr Cogn Disord,2012,33:149-155.
[24]Jessen F,Traeber F,Freymann K,et al.Treatment monitoring and response prediction with proton MR spectroscopy in AD[J].Neurology,2006,67:528-530.
[25]Modrego P J,Fayed N,Errea J M,et al.Memantine versus donepezil in mild to moderate Alzheimer's disease:a randomized trial with magnetic resonance spectroscopy[J].Eur J Neurol,2010,17:405-412.
[26]Glodzik L,King K G,Gonen O,et al.Memantine decreases hippocampal glutamate levels:a magnetic resonance spectroscopy study[J].Progress in Neuro-Psychopharmacology& Biological Psychiatry,2008,32:1005-1012.
[27]Guadagna S,Esiri M M,Williams R J,et al.Tau phosphorylation in human brain:relationship to behavioral disturbance in dementia[J].Neurobiol Aging,2012,33(12):2798-2806.
[28]Guadagna S,Esiri M M,Williams R J,et al.Tau phosphorylation in human brain:relationship to behavioral disturbance in dementia[J].Neurobiol Aging,2012,33(12):2798-2806.
[29]Gunnarsson M D,Kilander L,Sudelo¨f J,et al.Reduction of hyperphosphorylated-tau during memantine treatmentin Alzheimer's disease[J].Alzheim Dementia,2006,2(3):S63-S64.
[30]Smith A D.Imaging the progression of Alzheimer pathology through the brain[J].Proc Natl Acad Sci US A,2002,99(7):4135-4137.
[31]Palop J J,Mucke L.Amyloid-β Induced Neuronal Dysfunction in Alzheimer's Disease:From Synapses toward Neural NetworksNat Neurosci[J].2010,13(7):812-818.
[32]Sydow A,Jeugd A V,Zheng F,et al.Tau-Induced Defects in Synaptic Plasticity,Learning,and Memory Are Reversible in Transgenic Mice after Switching Off the Toxic Tau Mutant[J].The Journal of Neuroscience,2011,31(7):2511-2525.
[33]Chen G,Chen P,Tan H.Regulation of the NMDA Receptor-mediated Synaptic Response by Acetylcholinesterase Inhibitors and its Impairment in an Animal Model of Alzheimer's Disease [J].Neurobiol Aging,2008,29(12):1795-1804.
[34]Kim D H,Brown R T,Ding E L,et al.Dementia Medications and Risk of Falls,Syncope,and Related Adverse Events Meta-Analysis of Randomized Controlled Trials[J].J Am Geriatr Soc,2011, 59(6):1019-1031.
Combination of memantine and donepezil in treatment of patients with Alzheimer disease
Alzheimer Disease Behavioral and psychological symptoms DonepezilMemantine
2012-04-05)
(本文编辑:田云鹏)
310012 杭州,浙江省立同德医院老年科
【 Abstract】Objective To evaluate the efficacy and safety of combination of memantine and donepezil in treatment of patients with Alzheimer disease (AD).Methods Eighty patients with AD were randomly assigned to receive combination of memantine (starting dose 5 mg/d,5 mg weekly increments,20 mg/d after 4 weeks)and donepezil(starting dose 5 mg/d,10 mg/d after 4 weeks)(combination group,n=40)or donepezil alone(control group,n=40)for 12 weeks.The behavioral and psychological symptoms,activities of daily living and clinical global impression were evaluated with Behavioral Pathology in Alzheimer's Disease Rating Scale(BEHAVE-AD),Activities of Daily Living Inventory(ADL)and Clinical Global Impression Scale(CGI)before and after treatment.Results At the end of week 12,the scores of BEHAVE-AD and ADL were lower in combination treatment group than those in control group(8.1±3.30 vs 9.2±2.80,t=-3.317,P=0.002)and(28.1±2.35 vs 29.3±2.63,t=2.097,P<0.05), respectively.The CGI score in combination group was better than that in control group (3.43±0.82 vs 4.37±0.85,t=-5.413,P<0.01).Six patients(15.0%)in combination group and 5 patients(12.5%)in control group developed mild adverse effects respectively.Conclusion Combination of memantine and donepezil achieves better efficacy than donepezil alone in treatment of patients with Alzheimer disease.
