阿托伐他汀钙强化治疗对老年冠心病合并阵发性心房颤动患者左心功能、hs-CRP及房颤发作次数的影响
2023-07-10胡红梅李睿王雪佼裴新
胡红梅 李睿 王雪佼 裴新

【摘要】 目的:分析阿托伐他汀鈣强化治疗对老年冠心病合并阵发性心房颤动患者左心功能、超敏C反应蛋白(hs-CRP)及心房颤动发作次数的影响。方法:将昆明市中医医院2021年1月-2022年1月收治的70例老年冠心病合并阵发性心房颤动患者作为研究对象,按照随机数字表法,将患者分为对照组与研究组,各35例。两组患者均口服阿托伐他汀钙进行治疗,其中对照组给予常规剂量(40 mg/d),研究组给予强化剂量(80 mg/d)。比较两组治疗前和治疗后房颤发作次数、左室射血分数(LVEF)、左心房内径(LAD)及hs-CRP水平的差异。结果:治疗后,两组心房颤动发作次数均少于治疗前,且研究组心房颤动发作次数较对照组少(P<0.05)。相比治疗前,两组治疗后LAD显著下降,LVEF显著增高,且研究组LAD较对照组低,LVEF较对照组高(P<0.05)。与治疗前相比,两组治疗后hs-CRP水平显著下降,且研究组hs-CRP水平较对照组低(P<0.05)。结论:应用阿托伐他汀钙治疗可有效改善老年冠心病合并阵发性心房颤动患者左心房功能,减少心房颤动发作次数,减轻临床症状,同时具有减轻炎症反应的作用,其中强化剂量治疗的效果更优,因此具有良好的临床应用前景。
【关键词】 冠心病 阵发性心房颤动 阿托伐他汀钙 心功能 超敏C反应蛋白
[Abstract] Objective: To analyze the effect of intensive Atorvastatin Calcium therapy on left ventricular function, hypersensitive C reactive protein (hs-CRP) and the frequency of atrial fibrillation in elderly patients with coronary heart disease complicated with paroxysmal atrial fibrillation. Method: A total of 70 elderly patients with coronary heart disease complicated with paroxysmal atrial fibrillation admitted to Kunming Traditional Chinese Medicine Hospital from January 2021 to January 2022 were selected as the research subjects. According to the random number table method, the patients were divided into the control group and the research group, 35 cases in each group. Patients in both groups were treated with Atorvastatin Calcium orally, in which the control group was given the conventional dose (40 mg/d) and the research group was given the intensive dose (80 mg/d). The differences of the frequency of atrial fibrillation, left ventricular ejection fraction (LVEF), left atrial diameter (LAD) and hs-CRP levels were compared between the two groups before and after treatment. Result: After treatment, the frequency of atrial fibrillation in both groups were less than that before treatment, and the frequency of atrial fibrillation in the research group was less than that in the control group (P<0.05). Compared with before treatment, LAD decreased significantly and LVEF increased significantly in the two groups after treatment, and LAD in the research group was lower than that in the control group, and LVEF was higher than that in the control group (P<0.05). Compared with before treatment, the levels of hs-CRP in the two groups decreased significantly after treatment, and the level of hs-CRP in the research group was lower than that in the control group (P<0.05). Conclusion: Application of Atorvastatin Calcium therapy can effectively improve the left atrial function of elderly patients with coronary heart disease complicated with paroxysmal atrial fibrillation, reduce the frequency of atrial fibrillation, and reduce clinical symptoms. At the same time, it has the effect of reducing inflammatory response. The effect of intensive dose therapy is better, so it has a good prospect for clinical application.
[Key words] Coronary heart disease Paroxysmal atrial fibrillation Atorvastatin Calcium Cardiac function hs-CRP
First-author's address: Kunming Traditional Chinese Medicine Hospital, Kunming 650599, China
doi:10.3969/j.issn.1674-4985.2023.13.015
冠心病伴阵发性心房颤动是临床常见病、多发病之一,且在老年器质性心脏病患者中更为常见。据报道,炎症反应在心房颤动与动脉粥样硬化的发生和发展过程中起到重要作用[1]。阿托伐他汀钙的非降脂作用日益受临床医师的关注和认可,如其具有的抗炎和稳定粥样硬化斑块的作用,对心肌细胞的保护作用,可有效阻滞心肌重构,清除心律失常的病理基础,因此可用于临床治疗心房颤动患者[2-3]。并且,阿托伐他汀钙的治疗效果有一定的量效关系,即随着剂量的增加,其非抗炎作用更强[4]。为此,本研究通过选取昆明市中医医院收治的70例老年冠心病合并阵发性心房颤动患者,分析阿托伐他汀钙强化治疗对患者房颤发作次数、左心功能及超敏C反应蛋白(hypersensitive C reactive protein,hs-CRP)的影响,旨在为临床规范治疗提供一定意义。
1 资料与方法
1.1 一般资料 将昆明市中医医院2021年1月-2022年1月收治的70例老年冠心病合并阵发性心房颤动患者作为研究对象。纳入标准:(1)经冠状动脉造影、动态心电图检查明确诊断;(2)年龄60~80岁;(3)近3 d心房颤动每天发作几次;(4)无治疗药物用药禁忌证或过敏史。排除标准:(1)伴急性心肌炎、急性心肌梗死或介入手术导致的心房颤动;(2)近期(1个月内)服用他汀类药物;(3)存在房室传导阻滞;(4)伴恶性肿瘤,病情危急;(5)伴精神性疾病,治疗依从性差;(6)中途转院、放弃治疗,或退出研究。按照随机数字表法,将患者分为对照组与研究组,各35例。本研究内容已通过本院医学伦理委员会审核批准。所有患者及家属均对本研究知情同意。
1.2 方法 两组患者均应用华法林、胺碘酮等心房颤动常规药物治疗。两组患者均口服阿托伐他汀鈣片(生产厂家:辉瑞制药有限公司,批准文号:国药准字H20051408,规格:20 mg)进行治疗,其中对照组给予常规剂量,40 mg/次,1次/d;研究组采取强化剂量治疗,80 mg/次,1次/d。两组均连续用药3个月。
1.3 观察指标及判定标准 记录两组患者治疗前和治疗后24 h内心房颤动发作次数、左心房内径(left atrium diameter,LAD)、左室射血分数(left ventricular ejection fraction,LVEF)及hs-CRP。心房颤动发作次数通过24 h动态心电图检查进行评估。LAD和LVEF的检测通过彩色超声多普勒检查进行评估。hs-CRP通过全自动特定蛋白分析仪和乳胶增强免疫比浊法测定,试剂盒购自上海恒远生物科技有限公司,严格按照试剂盒说明书完成检测操作。
1.4 统计学处理 将数据录入SPSS 23.0版统计学软件进行处理。计量资料用(x±s)表示,组间比较采用独立样本t检验,组内比较采用配对t检验;计数资料用率(%)表示,比较用字2检验。P<0.05表明差异有统计学意义。
2 结果
2.1 两组基线资料比较 对照组男20例,女15例;年龄62~78岁,平均(69.08±5.12)岁;心房颤动持续时间40~63 min,平均(49.14±5.05)min。研究组男22例,女13例;年龄61~80岁,平均(68.77±6.13)岁;心房颤动持续时间42~62 min,平均(50.96±6.15)min。两组基线资料比较,差异均无统计学意义(P>0.05),具有可比性。
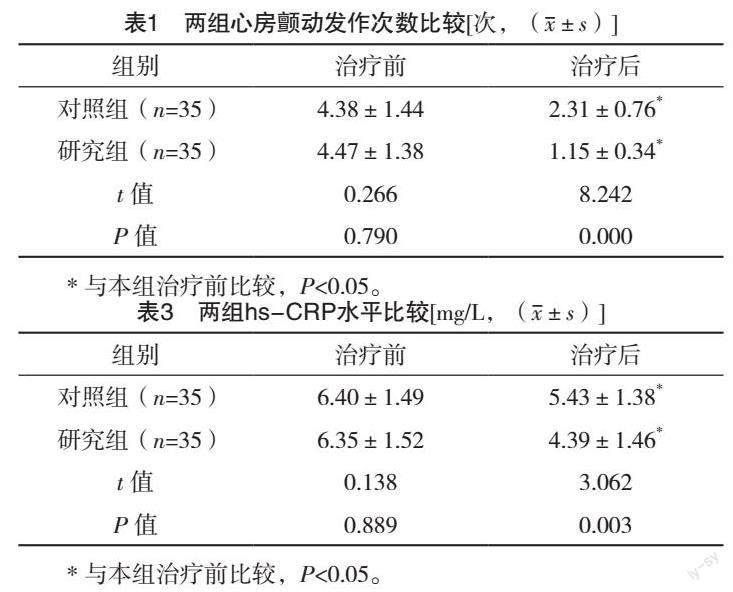
2.2 两组治疗前后心房颤动发作次数比较 两组治疗前心房颤动发作次数比较,差异无统计学意义(P>0.05);治疗后,两组心房颤动发作次数均显著少于治疗前,且研究组心房颤动发作次数较对照组明显减少(P<0.05)。见表1。
2.3 两组治疗前后LAD、LVEF比较 两组治疗前LAD、LVEF比较,差异均无统计学意义(P>0.05);相比治疗前,两组治疗后LAD均显著下降,LVEF均显著增高,且研究组治疗后LAD较对照组低,LVEF较对照组高(P<0.05)。见表2。
2.4 两组治疗前后hs-CRP水平比较 两组治疗前hs-CRP水平比较,差异无统计学意义(P>0.05);与治疗前相比,两组治疗后hs-CRP水平均显著下降,且研究组治疗后hs-CRP水平较对照组低(P<0.05)。见表3。
3 讨论
冠心病是心房颤动的常见病因之一,冠心病伴阵发性心房颤动在中老年人群中的患病率较高,超过65岁的老年人群心房颤动的发病率约为6%,而75岁以上的发病率约为10%[5]。这是因为,随着心房纤维化程度的加重和心房重构,使得传导减慢或出现传导阻滞,可进一步导致折返形成,使得老年人群出现心房颤动的风险增高[6]。并且,因局部心肌缺血,使得传导速度明显减慢,也易形成折返,加重心房颤动[7]。冠心病合并阵发性心房颤动可促使脑血管病的发病风险升高,并且心房颤动患者脑卒中发生率较无心房颤动者增高5倍,死亡率增高2倍[8]。因此,临床上应及时采取规范治疗,以免持续性心房颤动与永久性心房颤动的发生。动脉粥样硬化是引发冠心病的主要原因之一,心房颤动与冠心病的诱因、病因具有交叉重叠的特点,亦可共同发生,也可相互独立出现。炎症反应参与冠心病合并阵发性心房颤动的病理过程,其中hs-CRP浓度与心房颤动的发生存在密切关系[9-10]。
本研究發现,与治疗前相比,两组治疗后hs-CRP水平下降,且研究组hs-CRP水平较对照组低。分析原因:局部或全身性炎症在动脉粥样硬化及冠心病并发症的发生和发展过程中具有重要的促进作用。既往研究报道,炎症因子如hs-CRP等与冠心病发生和发展的病理过程存在显著关系,炎症因子浓度的高低对评估患者近远期心血管事件的发生具有重要的预测作用[11]。随着近年来国内外对炎症因子认识的进一步提高,已有研究证实炎症因子含量与心房颤动的病理过程密切相关[12]。此外,有研究表明,炎症因子与心房颤动的转归密切相关,其机制可能与心房肌重构和心房组织本身损伤有关[13]。
本研究发现,治疗后,两组患者房颤发作次数均显著少于治疗前,且研究组房颤发作次数较对照组少。此外,相比治疗前,两组治疗后LAD显著下降,LVEF显著增高,且研究组治疗后LAD较对照组低,LVEF较对照组高。分析原因:阿托伐他汀钙在临床治疗高血脂患者中发挥着显著作用,降脂效果较强,因而在冠心病患者临床治疗中的应用逐渐增多,已有研究证实该类药物具有减少冠心病发病和死亡风险的作用[14]。阿托伐他汀钙具有改善心脏自主神经功能、减轻炎症、抗血小板聚集、改善内皮功能、减少心房肌的结构重构与电重构等多种作用[15]。据报道,应用阿托伐他汀钙治疗的冠心病患者心房颤动发生率明显低于未服用阿托伐他汀钙者,且可有效降低心房颤动复发率,同时可降低其转化为持续性心房颤动的发生率[16]。美国心脏病学学会/2018年美国心脏协会血脂管理指南再次强调稳定型冠心病强化他汀治疗,且唯一明确推荐阿托伐他汀80 mg/d的用量[17-18],国内文献综述方面亦推荐冠心病患者应用强化他汀治疗[19-20]。上述研究均表明,老年冠心病合并阵发性心房颤动患者应用阿托伐他汀强化治疗可有效改善其心脏功能,减少心房颤动的发生,因此可有效减轻临床症状,增强临床疗效,同时可降低血清hs-CRP水平,其作用机制可能与缓解机体炎症反应密切相关,需今后进一步探究。
综上所述,应用阿托伐他汀钙强化治疗可有效改善老年冠心病合并阵发性心房颤动患者心功能,减少心房颤动发作次数,同时可降低血清hs-CRP水平,具有减轻炎症反应的作用,其中80 mg/d强化剂量治疗的效果更优,因此具有良好的临床应用前景。
参考文献
[1] KRISTIANSEN O,VETHE N T,PEERSEN K,et al.Effect of atorvastatin on muscle symptoms in coronary heart disease patients with self-perceived statin muscle side effects: a randomized, double-blinded crossover trial[J].Eur Heart J Cardiovasc Pharmacother,2021,7(6):507-516.
[2] LIU Q,DONG T,XI M,et al.Tongxinluo Capsule combined with Atorvastatin for coronary heart disease: a systematic review and Meta-analysis[J].Evid Based Complement Alternat Med,2021,2021:9413704.
[3] SZAREK M,AMARENCO P,CALLAHAN A,et al.Atorvastatin reduces first and subsequent vascular events across vascular territories: the SPARCL trial[J].J Am Coll Cardiol, 2020,75(17):2110-2118.
[4] LIU D,SHEN T,REN C,et al.The effects of Atorvastatin and Rosuvastatin on exercise tolerance in patients with coronary heart disease[J].Expert Opin Drug Saf,2020,19(9):1203-1208.
[5] ZHANG J,WANG J,YU H,et al.Comparison between Atorvastatin and Rosuvastatin on secondary percutaneous coronary intervention rate and the risk factors in patients with coronary heart disease[J].Curr Drug Metab,2020,21(10):818-828.
[6] KRISTIANSEN O,VETHE N T,FAGERLAND M W,et al.A novel direct method to determine adherence to Atorvastatin therapy in patients with coronary heart disease[J].Br J Clin Pharmacol,2019,85(12):2878-2885.
[7] LI K,LIU M M,YANG X,et al.Evaluation of efficacy and safety of combined Rosuvastatin and atorvastatin in treating with coronary heart disease: a protocol for systematic review and meta-analysis[J/OL].Medicine (Baltimore),2021,100(24):e26340.https://pubmed.ncbi.nlm.nih.gov/34128881/.
[8] PEREZ-CALAHORRA S,LACLAUSTRA M,MARCO-BENEDI V,et al.Comparative efficacy between atorvastatin and Rosuvastatin in the prevention of cardiovascular disease recurrence[J].Lipids Health Dis,2019,18(1):216.
[9]劉敏.氯吡格雷联合阿司匹林治疗老年冠心病的临床效果及对血清CRP水平的作用探讨[J].中外医学研究,2021,19(9):17-19.
[10] HANDAYANI W,SUHARJONO, YOGIARTO M.Analysis of HMGB-1 level before and after providing atorvastatin standard therapy in coronary artery disease patients with type-2 diabetes mellitus compared to without type-2 diabetes mellitus[J].J Basic Clin Physiol Pharmacol,2021,32(4):439-446.
[11] ABDULFATTAH S Y,AL-AWADI S J.ApoB gene polymorphism (rs676210) and its pharmacogenetics impact on atorvastatin response among Iraqi population with coronary artery disease[J].J Genet Eng Biotechnol,2021,19(1):95.
[12] TREMOULET A H,JAIN S,JONE P N,et al.Phase Ⅰ/Ⅱa trial of Atorvastatin in patients with acute kawasaki disease with coronary artery aneurysm[J].J Pediatr,2019,215:107-117.
[13]荣红丽,江珊.hs-CRP/ALB、LDL-C/HDL-C与冠状动脉病变程度的相关性研究[J].中国医学创新,2022,19(11):116-121.
[14]陈国,莫秀丽,林显营,等.氯吡格雷联合曲美他嗪治疗冠心病心绞痛的效果及对血清超敏C反应蛋白的影响[J].中国医学创新,2022,19(9):50-53.
[15]黄华,陈桂坚,彭志坚.短期强化他汀治疗对冠心病患者PCI术后心脏功能的影响[J].黔南民族医专学报,2021,34(2):87-89.
[16]邢玉良,柏松,戴新明,等.强化阿托伐他汀对急诊冠心病患者行冠状动脉介入治疗术后心源性休克和造影剂肾病的预防效果[J].中国实用医药,2021,16(12):12-14.
[17]吴娜琼,李建军.2018年美国心脏协会血脂管理指南解读[J].中国介入心脏病学杂志,2019,27(1):13-15.
[18] GRUNDY S M,STONE N J,BAILEY A L,et al.2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines[J/OL].Circulation,2019,139(25):e1082-e1143.https://pubmed.ncbi.nlm.nih.gov/30586774/.
[19]谢芳.强化阿托伐他汀对冠心病介入术后患者血清肌红蛋白、肌钙蛋白、心肌酶和心功能的影响[J].临床合理用药杂志,2022,15(1):44-47.
[20] LEI H P,QIN M,CAI L Y, et al.UGT1A1 rs4148323 A allele is associated with increased 2-hydroxy atorvastatin formation and higher death risk in Chinese patients with coronary artery disease[J].Front Pharmacol,2021,12:586973.
(收稿日期:2022-11-22) (本文编辑:陈韵)