Huge urinoma caused by spontaneous ureteral rupture secondary to ureteral obstruction due to prostate cancer
2020-12-28MikiNaito,RinzoUkai,KunihiroHashimoto等
Dear editor,
Spontaneous ureteral rupture (SUR) due to prostate cancer is very rare. The most common cause is calculus. To the best of our knowledge, SUR secondary to ureteral obstruction caused by prostate cancer was first reported by Deng et al. [1], so this case may be the second report. We report a case of a huge urinoma caused by SUR secondary to prostate cancer that was difficult to treat. This case is significant because the long-term presence of urinomas has never been reported.
A 67-year-old man was admitted to a nearby hospital with difficulty in urinating and walking. Laboratory evaluation revealed a prostate-specific antigen (PSA) level of 168.57 ng/mL. Computerized tomography (CT) showed prostate cancer (T3N0M0), left hydronephrosis, and a huge cystic lesion. A prostate biopsy showed adenocarcinoma with Gleason score of 8 (4+4).
After androgen deprivation therapy(ADT)was begun,he came to our hospital for treatment of the cystic lesion. A left nephrostomy tube and a drain were inserted,following which 3 470 mL of urine was drained over 10 h, and we diagnosed the cystic lesion as a urinoma.We failed to insert a ureteral stent because the tumor had invaded the bladder. The drain was subsequently removed, and he was discharged. ADT was continued for 15 months and was effective in reducing the PSA to 0.08 ng/mL. However, the patient felt abdominal tightness due to the recurrence of the urinoma and had it drained at a nearby hospital.
Thereafter, he was admitted to our hospital because of fever. Post-contrast CT imaging showed a large 28 cm×19 cm cystic lesion extending from the abdomen to the left pelvis(Fig.1),and a drain was inserted again.After he improved with antibiotics, antegrade insertion of a ureteral stent was attempted.Although we could not see a point of rupture, the ureteropelvic junction (UPJ) was narrow, so we suspected ureteral rupture. The ureteral stent was successfully inserted this time because the prostate cancer had been reduced by ADT,but the urinoma did not disappear.
Because we could not manage his fever, we performed open nephrectomy and resection of the urinoma. Intraoperative findings showed that the urinoma existed in succession next to the UPJ (Fig. 2), and it was considered part of the rupture. The urinoma had a thick wall with adhesions to the peritoneum and thus was difficult to extirpate. Pathological examination confirmed ureteral rupture because the ureter was present at the bottom of the cut face of the urinoma (Fig. 3). Gelatinous urine was also present inside the urinoma. The patient was discharged from hospital 8 days after surgery. He has not needed to return and he is working now.
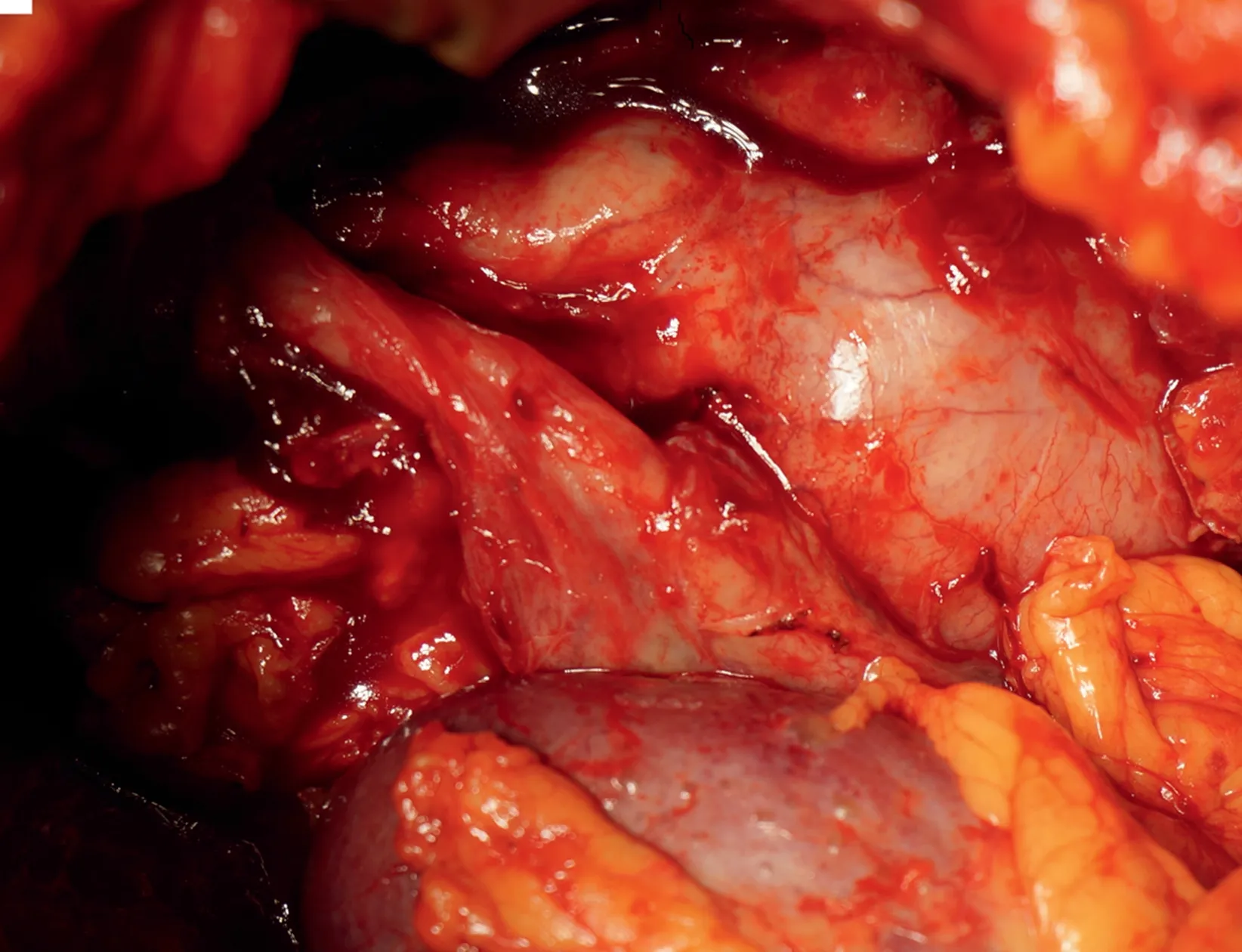
Figure 2 Intraoperative findings showed that the urinoma existed in succession next to the ureteropelvic junction.
We experienced a case of a huge urinoma caused by SUR secondary to ureteral obstruction due to prostate cancer.Intraoperative findings and pathological examination supported the clinical diagnosis. Deng et al. [1] reported the first case of SUR caused by prostate cancer.They also found it difficult to insert a ureteral stent,but they managed their patient with nephrostomy.
The present patient was very difficult to treat, and because the urinoma was asymptomatic and had been present for a long time, it required surgery. Urinomas that exist over a long period of time are very rare,so the present case is significant.
SUR is a very rare condition. Schwarz et al. [2] defined the word “spontaneous” as indicating a condition not caused by trauma or surgery. One half of SURs are caused by calculus,and obstruction by benign prostate hyperplasia and neurogenic bladder, cancer of the ureter, and steroid therapy may also cause it [3]. SUR caused by prostate cancer has only been reported once, thus indicating its rareness. It has non-specific symptoms such as abdominal tenderness and pain and costovertebral angle tenderness that make it difficult to diagnose [3].
Imaging including nephrostogram and retrograde pyelography did not reveal a point of rupture in our patient,but visualization at surgery and the pathological results indicated that the urinoma had grown within the retroperitoneum while accumulating urine within it. The treatment of SUR is initially conservative, but then urgent ureteral stent insertion, nephrostomy tube insertion, and urgent ureteroscopy may be required [4].
Urinomas may cause sensations of pressure or pain, but they may also be asymptomatic [5] as in the present case.The most important treatment is to deal with the underlying condition.
However,nephrostomy or stenting may be needed when the obstruction cannot be easily repaired [5]. In addition,fever or leukocytosis is a good reason to proceed to drainage, with surgery being the next step[5]. In our case,however, the obstruction was initially resolved with ADT,nephrostomy,ureteral stenting,and drainage,but after the urinoma reappeared, it required surgery.
Reported rates of obstructive uropathy for prostate cancer vary between 3.3%and 16.0%,and the prognosis for patients with malignant obstruction of the ureter ranges from 6 to 24 months [6]. However, hormone-sensitive patients such as our patient can live longer, so they require aggressive treatment. A case of hydronephrosis was reported that improved with ADT [7], which resolved obstruction of the bladder, but it is difficult to cure SUR only with ADT, and it can require advanced treatment.
Because the long-term existence of urinomas over several years has never been reported,there is currently no established treatment.We hope with further reports of this condition that a standard method of treatment can be devised.
SUR caused by prostate cancer is very rare,but this case emphasizes the necessity of controlling hydronephrosis.SUR can result in serious consequences, including urinoma,perinephric or retroperitoneal abscess formation, and urosepsis [8], so we should begin with conservative treatment.However,resolution of urinomas that may have been present for years can be very difficult,so treatment should start as quickly as possible.
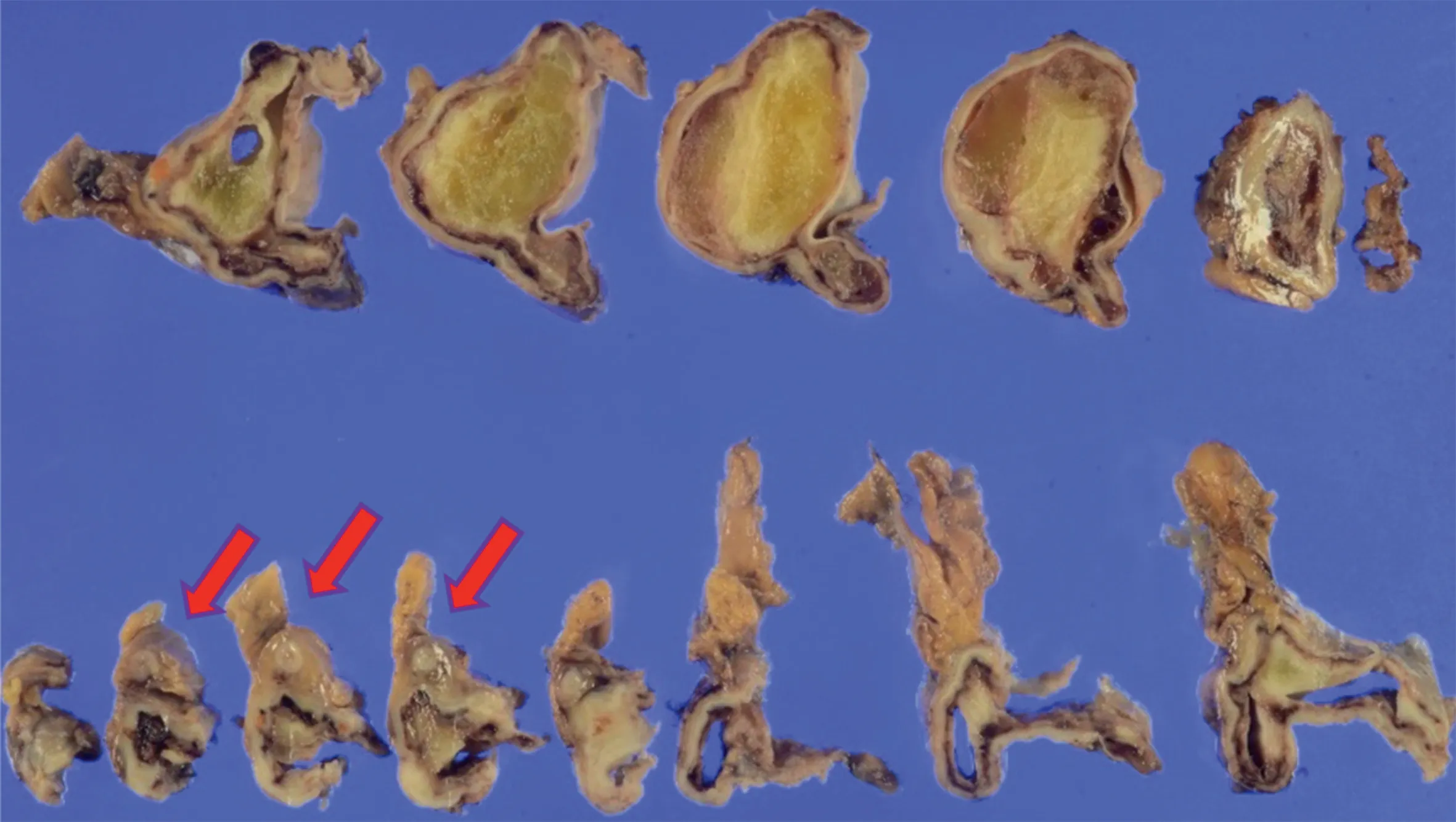
Figure 3 The cut face of the resected urinoma with the ureter at the bottom (arrows).
Author contributions
Study design:Kunihiro Hashimoto.
Data acquisition:Eiso Kawashita.
Drafting of manuscript:Miki Naito.
Critical revision of the manuscript:Rinzo Ukai.
Conflicts of interest
The authors declare no conflict of interest.
杂志排行
Asian Journal of Urology的其它文章
- Primary lymphomas of the genitourinary tract: A population-based study
- Xanthogranulomatous prostatitis:Impressive MRI appearance of a rare entity
- Giant pyogenic granuloma on the glans penis
- Cystoscopic extraction of an inadvertently placed ureteral stent in inferior vena cava
- Ambiguous clear cell carcinoma in medullary sponge kidney: A case report
- Investigation of confocal microscopy for differentiation of renal cell carcinoma versus benign tissue. Can an optical biopsy be performed?