Cystoscopic extraction of an inadvertently placed ureteral stent in inferior vena cava
2020-12-28AmbegodaLiyanaArachchigeMaduraChathurangaAmbegoda,MaduweGederaSagaraRuwanKumara,KusalaSandamalee等
Dear Editor,
A stent is a tube kept within a tubular structure to maintain luminal patency or protect an anastomosis or graft. In urological practice ureteral stents are inserted to relieve ureteral obstruction, to support ureteral anastomoses and repairs,to treat minor ureteric injuries,and to identify the ureters at open surgery. During insertion, ureteral stents may pierce the ureteric wall and enter adjacent structures.During removal, stents may cause undue damage to the ureter like ureteric avulsion and urine extravasation. Such injuries are categorized together under stenting induced trauma (SIT) [1]. Inadvertent entry of the stent into adjacent major vessels after perforation of the ureter is an important form of SIT due to its potential of causing life threatening complications.
A 68-year-old man with diabetes mellitus and a previous cerebral hemorrhage was found to have a renal abscess(12 cm×10 cm)in the right kidney.His serum creatinine was 186 μmol/L.The X-ray kidney ureter bladder(KUB)showed two calculi measuring 9 mm in the distal ureter. Despite intravenous antibiotics and percutaneous tube drainage of the abscess, the patient was having worsening sepsis and deteriorating renal functions. Hence a decision for retrograde ureteral stenting was made to decompress the obstructed right upper urinary tract.
Retrograde ureteral stenting was done using a 6 Fr,26 cm double-J stent and railroading it through a 0.038 Fr,Terumo© guide wire. Insertion of the stent was relatively straightforward apart from a slight resistance. Procedure was not done under image guidance as the facility was not available in the emergency operating room of the institute.There was a minimal pus discharge through the ureteric orifice. Immediate post-operative period was complicated with unusual severe hematuria, which gradually settled by the second post-operative day. Post-operative X-ray KUB revealed a medially positioned double-J stent (Fig. 1A).A non-contrast CT KUB showed the stent perforating the ureter just proximal to the stones to enter the right internal iliac vein.It had traversed through the common iliac vein to enter the inferior vena cava(Fig.1B).The upper end was at the level of the retro-hepatic inferior vena cava (IVC).There was no evidence of retroperitoneal hemorrhage in the CT scan. Flexible cystoscopy guided removal of the ureteral stent was done after preparing the patient for general anesthesia in case of an unprecedented bleed.There was no hematuria or ultrasound scan evidence of retroperitoneal bleeding after the procedure.
Though useful, ureteral stents can cause morbidity and even may lead to mortality. Stent related morbidity includes infection, severe lower urinary tract symptoms,flank and suprapubic pain, hematuria, bacterial colonization, stent migration, stent encrustation and stent fragmentation.Forgotten stent is another entity that can cause long-term morbidity like large stone formation, severe urosepsis, difficulty in removal and loss of renal unit.Compared to stent related morbidity, SIT is a rare, largely under-reported albeit important complication of ureteric stents. It is defined as traumatic injuries incurring to the urinary tract during the insertion and removal of ureteric stents.Major vessels are commonly involved apart from the gastro intestinal system [1]. According to published case reports, malposition of ureteral stents into adjacent major arteries is commoner than veins.A cause-specific mortality rate of 9%has been established based on reported cases of SIT [1]. Due to rarity of published reports of venousureteral fistulae, there are no data on the mortality rates of this condition [2]. Ureteral stenting is considered a safe procedure performed even when the clinical situation lacks scientific merit [3]. Although the associated morbidity is mild in most cases, life-threatening complications may occur. Overuse of medical interventions and inappropriate care are widespread phenomena all over the world [4].Medical personnel overuse ineffective but familiar, lucrative or otherwise convenient services, despite marginal benefits to patients [4]. Hence the indications for ureteral stenting should be evidence-based and truly beneficial to the patient [5].
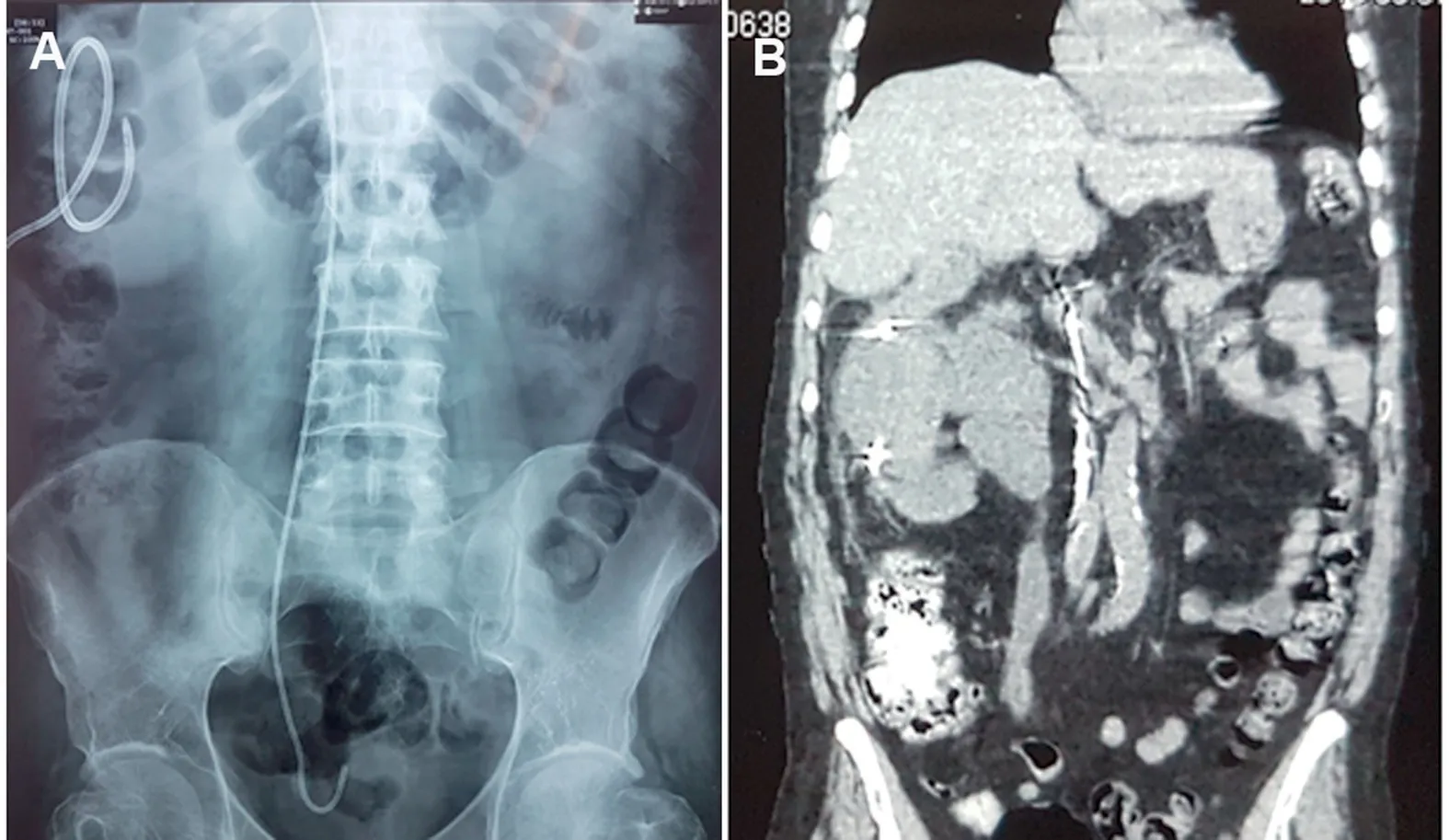
Figure 1 Post procedural cross sectional imaging. (A) X-ray KUB showing a medially displaced double-J stent with the straightened upper end. Note the lower ureteric calculi and percutaneous nephrostomy tube; (B) Non-contrast CT KUB showing the ureteral stent inside the IVC. KUB, kidney ureter bladder; IVC, inferior vena cava.
Patient related risk factors for SIT are pelvic irradiation, pelvic malignancy, extirpative pelvic surgery, urolithiasis, urinary diversion and vascular pathologies.Insertion of stents without fluoroscopy guidance, inadvertent insertion of the rigid reverse end of the guide wire and forcible stent insertion are the main operator-related risk factors [1,6-8]. However due to poor tissue quality,ureteric perforation may occur with minimal force [2].Although X-ray KUB would suggest a malpositioned ureteral stent, the mainstay of diagnosis is by a CT KUB [1].Removal of such stents can be attempted endoscopically,percutaneously or by open surgery [1]. Type of surgery depends on where the stent is located and ease of access to the malpositioned stent with minimal collateral damage. Open (37.5%) and percutaneous (37.5%) approaches have been attempted commonly while 25.0% of the interventions have been endourologically in a series of 24 interventions [1].
We found that cystoscopic removal of the inadvertently inserted ureteral stent into IVC,to be a safe approach if the lower end still lies inside the bladder without migrating completely into IVC.Migration was a possibility in our case as misplacement of the stent was detected on the second day after surgery. Endoscopic removal may be followed by a transient self limiting hemorrhage through the ureteric orifice.Since the puncture in the vein is so small and the vein involved is in the retroperitoneal space,significant bleeding is unlikely due to the tamponade effect enforced by surrounding structures [9]. The endourological removal of a stent malpositioned in veins is also supported by few published case reports[6,9,10].However,misplaced stents in the arterial tree have been dealt more commonly with open surgery.If the stent migrates completely into the vessel,an endovascular or open surgical approach is warranted.
In conclusion,ureteral stenting which is considered a simple procedure may cause serious morbidity including inadvertent insertion of stents into adjacent major vessels.Such mishaps can occur when fluoroscopy is not used to identify abnormal positioning of the guide wire before stent insertion.Itappearsthatendoscopicremovalofamalpositionedureteric stent in the IVC can be safely attempted endourologically.
Author contributions
Study Concept and Design:Anuruddha Mahasen Abeygunasekera.
Data Acquisition:Ambegoda Liyana Arachchige Madura Chathuranga Ambegoda, Kusala Sandamalee.
Data Analysis:Ambegoda Liyana Arachchige Madura Chathuranga Ambegoda, Maduwe Gedera Sagara Ruwan Kumara.
Drafting of Manuscript:Anuruddha Mahasen Abeygunasekera.
Critical Revision of the Manuscript:Anuruddha Mahasen Abeygunasekera, Ambegoda Liyana Arachchige Madura Chathuranga Ambegoda.
Conflicts of interest
The authors declare no conflict of interest.
杂志排行
Asian Journal of Urology的其它文章
- Primary lymphomas of the genitourinary tract: A population-based study
- Xanthogranulomatous prostatitis:Impressive MRI appearance of a rare entity
- Giant pyogenic granuloma on the glans penis
- Huge urinoma caused by spontaneous ureteral rupture secondary to ureteral obstruction due to prostate cancer
- Ambiguous clear cell carcinoma in medullary sponge kidney: A case report
- Investigation of confocal microscopy for differentiation of renal cell carcinoma versus benign tissue. Can an optical biopsy be performed?