Investigation of confocal microscopy for differentiation of renal cell carcinoma versus benign tissue. Can an optical biopsy be performed?
2020-12-28MihlPhungAnrwRousJyPngilinnRortBllErikBrmontShrfunMshiArthurGmitroBnjmin
Mihl C. Phung , Anrw R. Rous , Jy Pngilinn ,Rort C. Bll , Erik R. Brmont , Shrfun Mshi ,Arthur F. Gmitro , Bnjmin R. L
a Department of Urology, University of Arizona College of Medicine, Arizona, USA
b Department of Medical Imaging, University of Arizona College of Medicine, Arizona, USA
c Department of Pathology, University of Arizona College of Medicine, Arizona, USA
d Ringgold Standard Institution, Aminu Kano Teaching Hospital, Kano, Nigeria
e Biomedical Engineering, University of Arizona College of Medicine, Arizona, USA
KEYWORDS Renal cell carcinoma;Confocal microscopy;Optical biopsy
Abstract Objective: Novel optical imaging modalities are under development with the goal of obtaining an “optical biopsy” to efficiently provide pathologic details. One such modality is confocal microscopy which allows in situ visualization of cells within a layer of tissue and imaging of cellular-level structures.The goal of this study is to validate the ability of confocal microscopy to quickly and accurately differentiate between normal renal tissue and cancer. Methods: Specimens were obtained from patients who underwent robotic partial nephrectomy for renal mass.Samples of suspected normal and tumor tissue were extracted from the excised portion of the kidney and stained with acridine orange.The stained samples were imaged on a Nikon E600 C1 Confocal Microscope. The samples were then submitted for hematoxylin and eosin processing and read by an expert pathologist to provide a gold-standard diagnosis that can later be compared to the confocal images. Results: This study included 11 patients,17 tissue samples,and 118 confocal images.Of the 17 tissue samples, 10 had a gold-standard diagnosis of cancer and seven were benign. Of 118 confocal images, 66 had a gold-standard diagnosis of cancer and 52 were benign. Six confocal images were used as a training set to train eight observers. The observers were asked to rate the test images on a six point scale and the results were analyzed using a web based receiver operating characteristic curve calculator. The average accuracy, sensitivity, specificity, and area under the empirical receiver operating characteristic curve for this study were 91%,98%,81%, and 0.94 respectively.
Conclusion: This preliminary study suggest that confocal microscopy can be used to distinguish cancer from normal tissue with high sensitivity and specificity.The observers in this study were trained quickly and on only six images. We expect even higher performance as observers become more familiar with the confocal images.
1. Introduction
Confocal microscopy is an imaging modality used to image thick sections of tissue in three dimensions.This technology is a method of optical sectioning, which captures twodimensional images at different depths and reconstructs a three-dimensional image.The confocal laser allows for high contrast and enhanced spatial resolution [1], identifying cellular structures with accuracy that is comparable to traditional histologic techniques [2]. It also allows for a wide variety of tissue such as bladder, gastrointestinal tract, cornea, skin, and oral mucosa to be imaged in both ex vivo and in vivo settings [3,4] with high fidelity. Given this capability, confocal microscopy has potential for various medical applications ranging from oncologic control to identification of inflammatory lesions and has been demonstrated to have both high sensitivity and specificity(see Tables 1 and 2).
Confocal microscopy has been applied to a number of oncologic and surgical fields. Previous work with ovarian cancer demonstrated confocal microscopy can be used to identify ovarian cancer versus normal tissue [5-7].Sankar et al. [8], in their preliminary study in mice,demonstrated the ability of confocal microscopy to diagnose glioblastoma with comparative accuracy to traditional histology. Similarly in ophthalmology, Tavakoli et al.[9] evaluated the potential of confocal microscopy to perform detailed morphological analysis of corneal structures. Gastrointestinal mucosa has also been assessed with applications such as the evaluation of dysplasia in Barrett’s esophagus with sensitivities up to 98% and specificities approaching 100% for observers with experience interpreting confocal images [10,11]. In the surgical setting, Terrier et al. [12] established that confocal microscopy can accurately identify surgical margins in genital Paget disease.Crowe and colleagues [13] used confocal microscopy to identify peripheral nerve injury and developed protocol of imaging peripheral nerves intraoperatively.
In the urological literature,work has been performed on the application of confocal microscopy for the treatment and diagnosis of upper and lower tract urothelial carcinoma[14-17]. Wu et al. [14] demonstrated that confocal imaging of urothelial structures was comparable to hematoxylin and eosin (H&E) histopathology, allowing for the differentiation between high and low grade urothelial carcinoma.Su et al. [18] used confocal microscopy to assess renal structures and demonstrated that ex vivo confocal laser microscopy could readily identify renal structures including glomeruli and tubules. They also demonstrated that malignant renal tumors had vastly different microarchitecture under confocal microscopy versus normal renal parenchyma. In vivo, Bui et al. [15] has piloted the use of confocal microscopy for the management of upper tract lesions.These studies demonstrated that optical biopsy can be used to aid in oncologic control by assessing the depth of penetration and the surgical margin in real time [16].
There is potential for confocal microscopy to evaluate the surgical margin in renal cell carcinoma. An estimated 65 340 new cases of kidney and renal pelvis cancer occurred in 2018. This number has steadily risen since the 1970’s[19,20]. Partial nephrectomy is currently considered the gold-standard for cancer control of cT1a renal lesions and becoming increasingly common in managing larger lesions amenable to resection [19,21]. To aid in intraoperative management, surgeons have used frozen section to guide resection and aid in cancer control [22]. Unfortunately,frozen section is time consuming, can lead to surgical delays, and has a high false negative rate compared to final pathology [23,24]. Additionally, there is substantial monetary cost of performing the frozen section, which can be upwards of $3 000 per case [25], as well as potential harm of prolonged general anesthesia. Final histology reports come days later,well after any intervention could occur at the time of the primary surgery. Repeat surgery is sometimes required,which leads to increased cost and increased risk for the patient and healthcare provider.
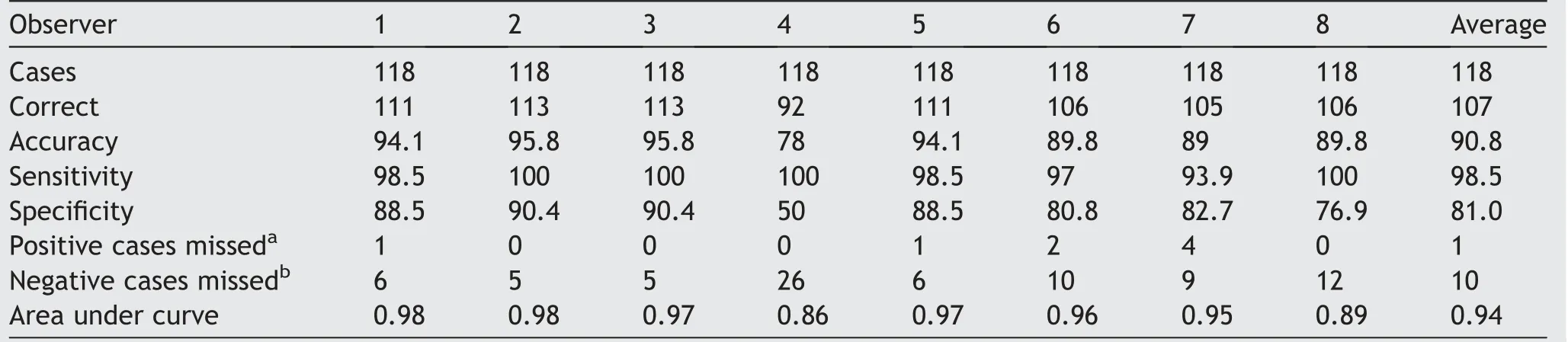
Table 1 Results of reviewer interpretation of confocal imagery as cancer vs. no cancer.
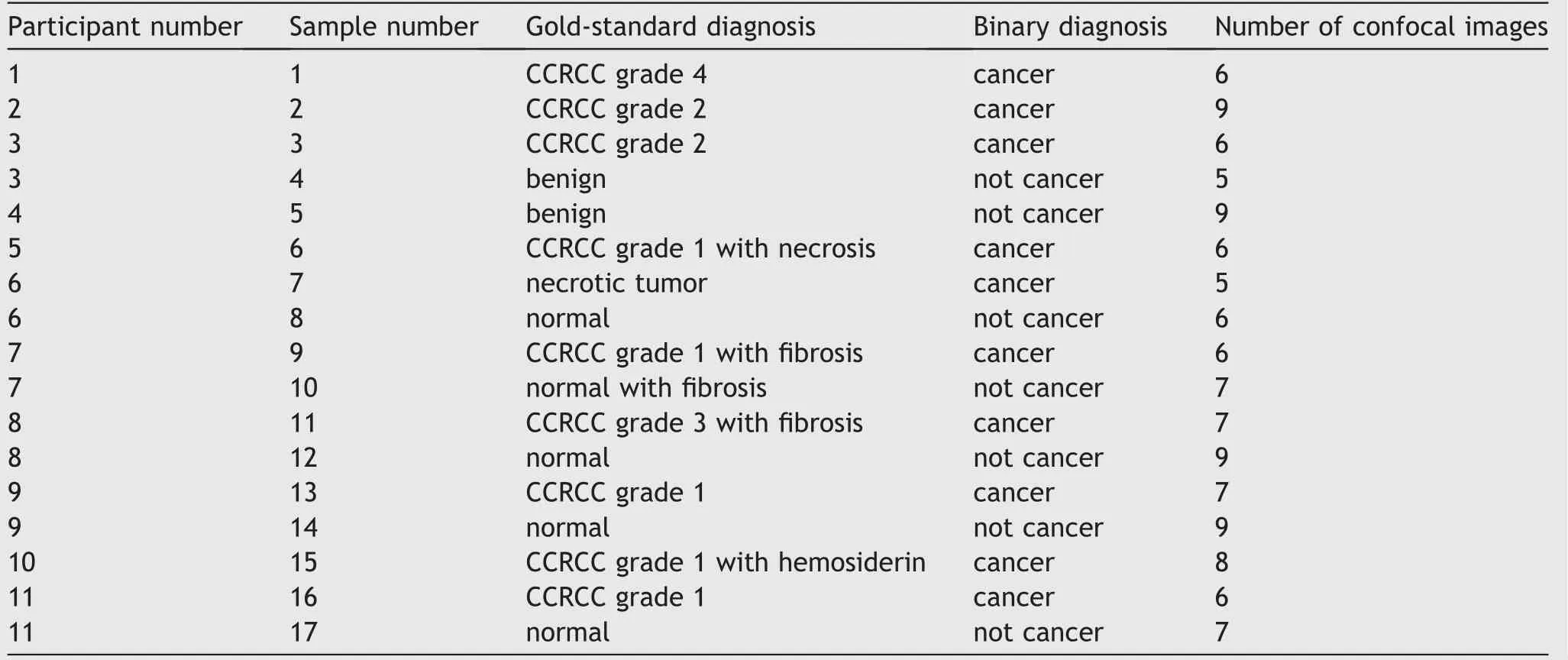
Table 2 Overview of pathology specimens obtained from enrolled subjectsa.
Given the detailed resolution of confocal microscopy,urologists could assess the margin in partial nephrectomy and avoid the lengthy delays,increased costs,and potential morbidity associated with frozen section.Both the provider and the patient would benefit greatly from improvements in the pathologic diagnosis process. The aforementioned work reveals that confocal microscopy is a promising modality that can improve efficiency in diagnosis while maintaining accuracy. The goal of this first stage, proof of concept study is to begin validating the use of confocal microscopy as an optical biopsy for renal cell carcinoma by directly comparing the pathologic assessment of specimens by confocal microscopy against formalin fixed histopathology.
2. Materials and methods
2.1. Data source and study population
This study was performed with approval from the Arizona Health Sciences Center institutional review board (IRB).Informed consents were obtained from all patients undergoing the study. From June 2016 to Nov 2017, 75 nephrectomies were performed via robotic partial nephrectomy or laparoscopic radical nephrectomy at the University of Arizona College of Medicine, Tucson, USA. Of these 75 nephrectomies,17 specimens were obtained from 11 patients who underwent robotic assisted laparoscopic partial nephrectomy for clinical suspicion of renal cell carcinoma.All surgeries were performed by a single surgeon.Lesions were localized intraoperatively using an Aloka roboticallycontrolled ultrasound transducer and resected with the goal of achieving a 1 cm margin.
Small samples of suspected normal and tumor tissue were then extracted from the excised portion of the kidney and stained with acridine orange (AO), an intravital fluorescent contrast agent that binds to nucleic acids. The stained samples were imaged on a Nikon E600 C1 Confocal Microscope(Nikon Corporation,Minato,Tokyo,Japan)using 10× and 20× objectives. The tissue samples were then submitted for H&E processing and read by an expert pathologist to provide a gold-standard diagnosis for later comparison to confocal images.
2.2. Primary outcome
Confocal images obtained from the excised specimens were reviewed by eight reviewers, which included one optical sciences graduate student, two optical science PhDs, one attending urologist,three urology residents,and one thirdyear medical student. Reviewers were trained to identify normal tissue versus cancer with a set of six confocal images consisting of three known normal tissue and three known cancer. The researchers had previously determined that the presence or absence of identifiable tubules was the best method to discern normal tissue from cancer. The training slides had a strong emphasis on this indicator.Upon completion of the training set, reviewers were shown a series of confocal images and instructed to rate each image on a 6-point scale ranging from definitely benign to definitely cancer.
3. Data analysis
Given the binary nature (cancer vs. normal) of the detection task,results from reviewer ratings were inputted into a web based receiver operating characteristic curve calculator[26]and the average accuracy,sensitivity,specificity,and area under the empirical receiver operating characteristic (ROC) curve were obtained.
4. Results
Of the 17 tissue samples obtained, 10 were pathologically confirmed to be renal cell carcinoma on final histopathology and seven were normal renal tissue. A total of 118 confocal images were used in this study. Of these 118 images, 66 were confirmed on final histopathology to be cancer and 52 were benign.
Fig. 1 shows example confocal images of normal kidney and kidney cancer. The normal kidney (Fig. 1A) has clearly identifiable normal renal tubules. Fig. 1B is renal cell carcinoma(RCC)in which there is a higher cellular density,and when magnified, the shape of the nuclei is also more heterogeneous. The average accuracy, sensitivity, specificity,and area under the empirical ROC curve were 91%, 98%,81%, and 0.94, respectively. The overall ROC evaluation results from the eight observers are shown in Fig. 2.
Reviewers were generally consistent in the images that were diagnosed correctly and incorrectly. This was likely a reflection of the presence or absence of normal appearing tubules within the image. There were some normal tissue images that were consistently diagnosed as being cancer.This may have been the result of a tangential cut through the tubules that skewed the appearance and made the identification of tubules more difficult. The best performance was achieved by members of the team who had the most experience observing confocal fluorescence images stained with AO,indicating that there is a learning curve for new observers viewing the non-conventional histology images.
5. Discussion
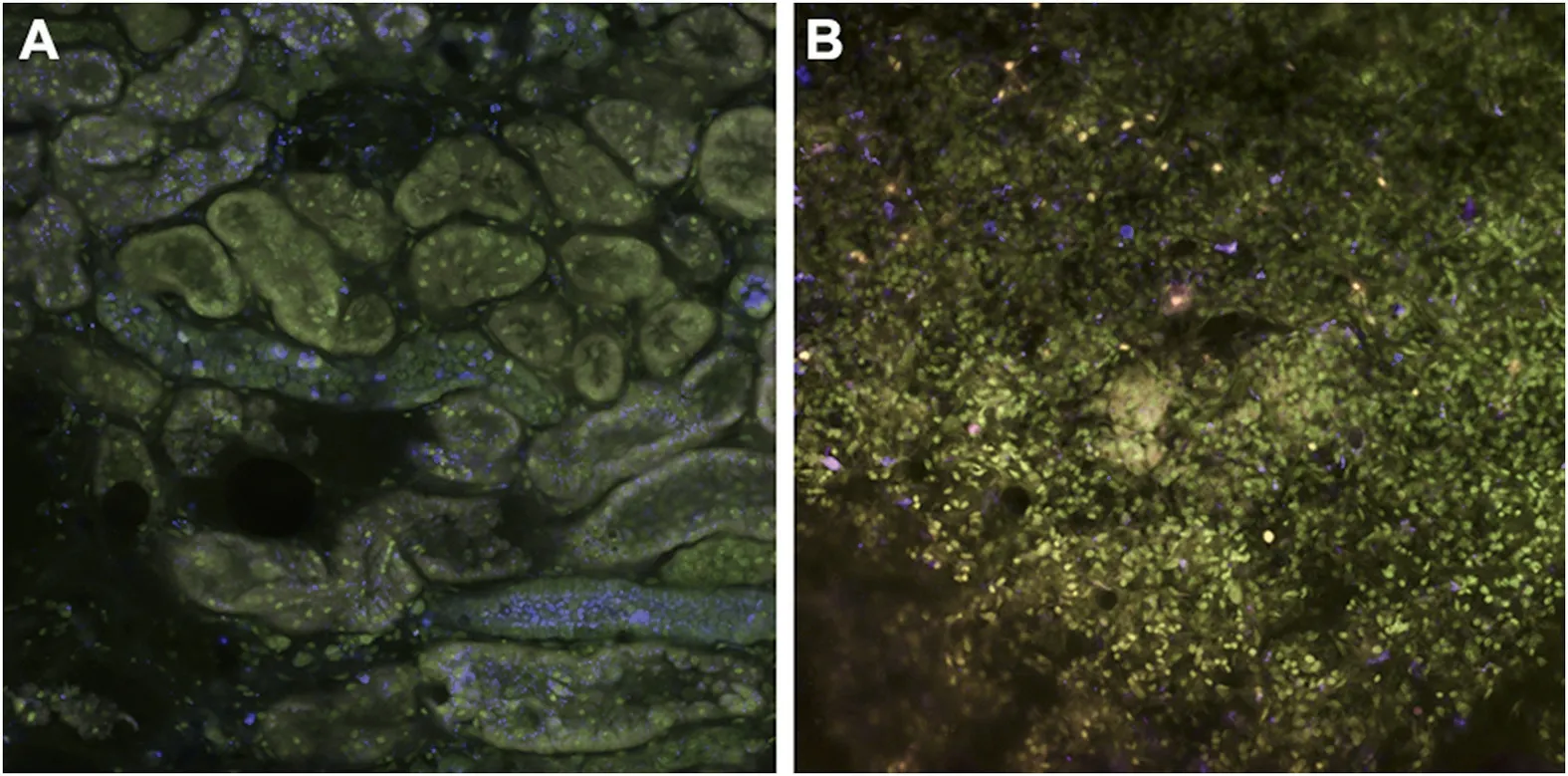
Figure 1 Example confocal images (20×) of normal kidney and kidney cancer. The normal kidney (A) has clearly identifiable normal renal tubules. (B) Renal cell carcinoma in which there is a higher cellular density, and when magnified, the shape of the nuclei is also more heterogeneous.
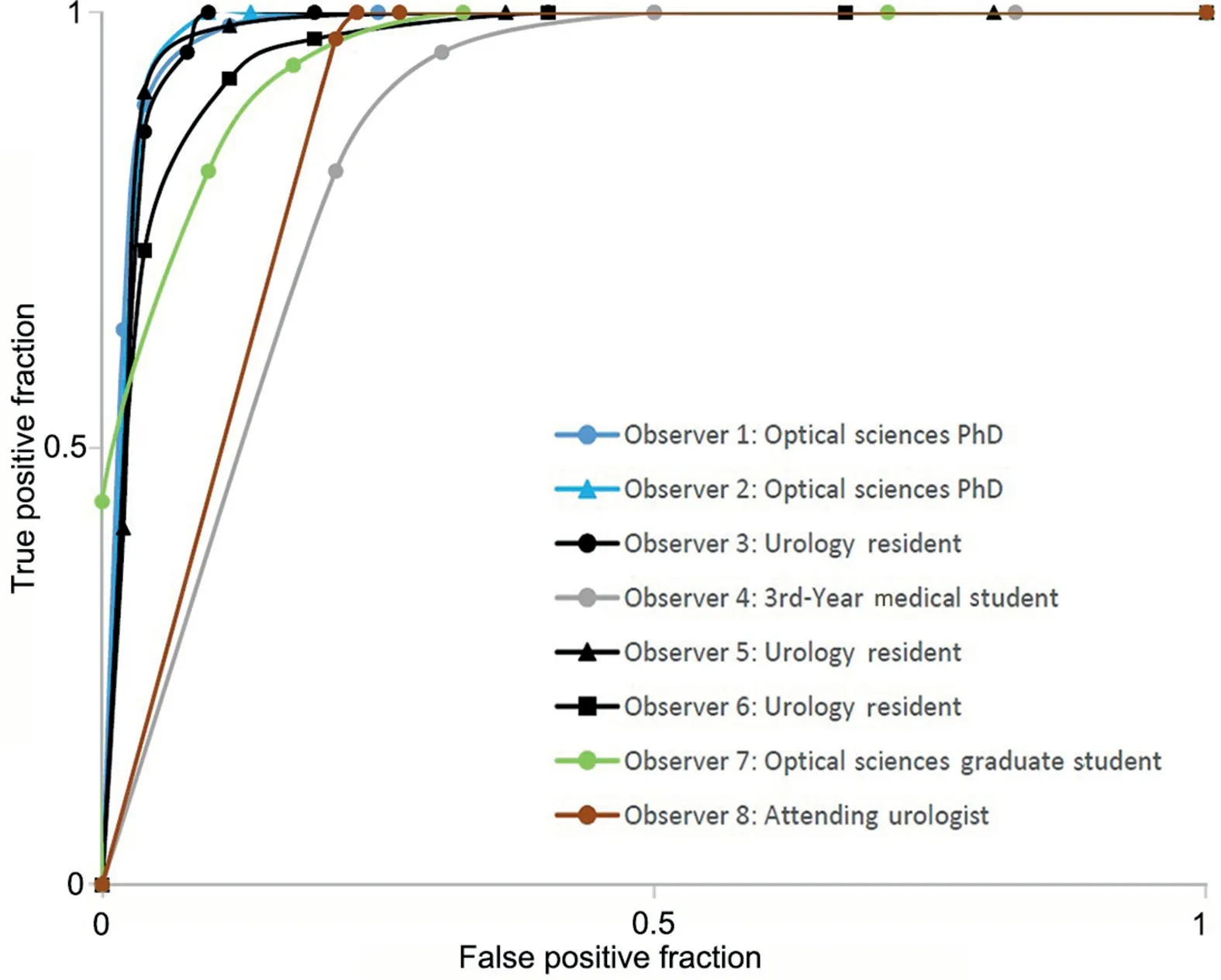
Figure 2 Operating characteristic curves from eight observers.
Su et al. [18] had previously demonstrated the ability of confocal microscopy to identify key renal structures in ex vivo specimens. Our study builds upon this body of work by demonstrating the promise of using confocal microscopy as a form of optical diagnosis following surgical resection of renal cell carcinoma. Our study is, to our knowledge, the first study attempting to validate the use of confocal microscopy vs. formalin fixed histopathology in the determination of normal renal tissue versus cancer. A large confocal image data set was used to test a series of reviewers from different backgrounds with varying degrees of medical knowledge and yet the results still demonstrated high sensitivity, specificity, accuracy, and area under the ROC curve. This was particularly impressive given the limited training prior to deciphering the confocal images.Slides that were wrongly marked normal or wrongly marked as cancer were generally consistent amongst reviewers,and it is reasonable to assume that reviewers could improve these results with increased training and exposure to confocal microscopy images. Given these results, confocal microscopy may serve as an alternative to frozen section in assessing ex vivo specimens at the primary surgery. This could allow for efficient and accurate evaluation of the surgical margin at the primary surgery, resulting in improved oncologic outcomes.
The results are also in line with previous literature concerning the accuracy of confocal microcopy regardless of medical background.Chen et al.[27]demonstrated that a large population of observers without a medical background were able to accurately distinguish malignant urothelium from benign urothelium.Chang et al.[28]similarly found a high rate of inter-observer agreement in the diagnosis of bladder cancer using confocal optical biopsies.The results of these previous studies, in addition to this study,support the ease of use, training, and accuracy of confocal microscopy as an optical biopsy.
Confocal microscopy has been applied to multiple other urologic fields including bladder cancer and prostate cancer[29,30]. Lopez et al. [30] demonstrated that confocal microscopy could be used intraoperatively during robotic assisted prostatectomy to identify structures in vivo and aid in sparing of the neurovascular bundles to improve patient outcomes. Smith and colleagues [31] used confocal microscopy in sperm extraction from azoospermic mice,demonstrating potential to decrease operative time and improve the sperm harvest rate. Naya and colleagues [32]have conducted a preliminary study using probe-based confocal laser microscopy and were able to show that the morphological patterns of bladder cancer using confocal microscopy were like those of histopathology studies.Similarly, Breda and colleagues [33] compared confocal laser endomicroscopy evaluation with histological findings and found concordances of 100%, 83%, and 100% in characterizing low-grade, high-grade, and carcinoma in situ of upper urinary tract cancer, respectively. There are also several reports that demonstrated the efficacy of a probebased confocal laser endomicroscopy in detecting bladder urothelial cancer using fluorescein [29,34-36]. Clearly,confocal microscopy has excellent potential for clinical applications that would improve patient outcomes and increase efficiency.
Compared to other modalities, such as optical coherence tomography which uses near-infrared light, confocal microscopy allows for increased depth of penetration and increased resolution. This leads to a more accurate diagnoses and reinforces the strengths of confocal microscopy as a modality for real time optical biopsy.Structured illuminated microscopy uses patterned illumination as a sectioning technique and provides similar resolution as confocal microscopy. However, confocal microscopy has more utility to image tissue in vivo with probes as small as 0.78 mm, allowing for its use in both endoscopic and laparoscopic settings.
Given these strengths, there is potential for intraoperative use of confocal microscopy in an in vivo setting during partial nephrectomy. Pathologic information regarding a positive margin could be relayed more quickly and perhaps more accurately when compared to intraoperative frozen section. This would allow for earlier counseling of the patient and/or their families in regards to clinical decision making. Thus far, this study represents an ex vivo first stage process towards the goal of being able to clinically evaluate an in vivo process.
Our study had some limitations. While attempts were made to ensure that the confocal images were obtained from the area of the specimen that was assessed for final diagnosis on histopathology, we were unable to do this with complete certainty. Also, reviewers were not timed and were able to spend as much or as little time on each image as they desired. Specimens were clear cell in final histopathology and it is possible that other subtypes of renal cell carcinoma may affect the results. However,subtypes may not be as significant for our study, as the presence of traditional renal structures was the main determinant in categorizing a specimen as normal or cancerous.
In addition, the adoption of confocal microscopy in a clinical setting will be dependent on the efficiency and the time required for diagnosis.There is currently a wide range of scan times reported in the literature ranging from 1 to 2 frames per second up to incredibly 16 000 frames per second at various resolutions[17,37,38].The Nikon microscope used in this study captured 2 mm×2 mm field of view at 2 frames per second with 10x magnification. Future work would focus on reducing time needed to scan the cut margin while maintaining diagnostic efficacy. This could perhaps be accomplished via parallel line-scanning confocal fluorescence microscope models and aided by automated diagnostic software to improve efficiency.
6. Conclusion
Confocal microscopy is a promising modality that could allow for efficient and accurate diagnosis of the surgical margin. Future studies will be focused on an even larger number of samples of varying subtypes and with a wider range of reviewers. A direct comparison between confocal microscopy, frozen section, and final histopathology would allow for further validation of the use of confocal microscopy in lieu of frozen section.
Author contributions
Study concept and design:Benjamin R. Lee, Arthur F.Gmitro, Andrew R. Rouse, Michael C. Phung.
Data acquisition:Andrew R. Rouse, Michael C. Phung,Robert C. Bell, Erika R. Bracamonte.
Data analysis:Andrew R. Rouse, Michael C. Phung, Robert C. Bell, Erika R. Bracamonte.
Drafting of manuscript:Michael C. Phung, Andrew R.Rouse, Benjamin R. Lee, Arthur F. Gmitro, Jayce Pangilinan, Sharfuddeen Mashi.
Critical revision of the manuscript:Michael C. Phung,Andrew R. Rouse, Benjamin R. Lee, Arthur F. Gmitro.
Conflicts of interest
The authors declare no conflict of interest.
Acknowledgments
Research reported in this publication was supported by the National Cancer Institute Cancer Center Support Grant(P30 CA023074) and used the Tissue Acquisition and Cellular/Molecular Analysis Shared Resource at the University of Arizona.
杂志排行
Asian Journal of Urology的其它文章
- Primary lymphomas of the genitourinary tract: A population-based study
- Xanthogranulomatous prostatitis:Impressive MRI appearance of a rare entity
- Giant pyogenic granuloma on the glans penis
- Huge urinoma caused by spontaneous ureteral rupture secondary to ureteral obstruction due to prostate cancer
- Cystoscopic extraction of an inadvertently placed ureteral stent in inferior vena cava
- Ambiguous clear cell carcinoma in medullary sponge kidney: A case report