Role of selected criteria and preventive chemotherapy in tumor recurrence after liver transplantation
2020-09-21MeiXiWangDongChenYuanYuanZhaoBoYangJiPinJiangFanJunZengLaiWeiZhiShuiChen
Mei-Xi Wang , Dong Chen , Yuan-Yuan Zhao , Bo Yang , Ji-Pin Jiang ,Fan-Jun Zeng , Lai Wei , *, Zhi-Shui Chen
a Institute of Organ Transplantation, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan 430030, China
b Key Laboratory of Organ Transplantation, Ministry of Education, Wuhan 430030, China
c NHC Key Laboratory of Organ Transplantation, Wuhan 430030, China
d Key Laboratory of Organ Transplantation, Chinese Academy of Medical Sciences, Wuhan 430030, China
Keywords:
ABSTRACT
Introduction
Hepatocellular carcinoma (HCC) represents one of the most common tumors worldwide and is the second most common cause of cancer-related deaths [1].Approximately 782 500 new cases of liver cancer are reported each year; of these approximately 745 500 patients die from liver cancer, with roughly 50% of the deaths in China [2].Compared with HCC patients from Western countries, Chinese HCC patients present with distinct clinical characteristics.When diagnosed at an early stage, Chinese HCC patients usually presented with a larger tumor diameter, higher incidences of portal vein invasion or thrombosis and extrahepatic spread and a lower median survival time [3 , 4].Presently, liver transplantation(LT) is considered the treatment of choice for HCC patients, especially for those with end-stage cirrhosis [5].Since Mazzaferro et al.[6]proposed the Milan criteria in 1966, several criteria, such as UCSF criteria [7], Hangzhou criteria [8], and up-to seven criteria[9]were introduced with an attempt to expand the indications ofLT.The Hangzhou criteria [maximal tumor diameter of ≤8 cm, regardless of the alpha-fetoprotein (AFP) levels and histopathological tumor differentiation or a tumor burden with a total tumor diameter>8 cm and AFP levels ≤ 100 ng/ml and a well to moderately differentiated histopathological tumor grading G1 or G2]were first proposed in 2008.The Hangzhou criteria were well accepted by several research centers since more HCC patients could benefit from these criteria for LT.Studies reported that the survival rates for the Hangzhou criteria were not significantly different from those for the Milan criteria [10 , 11], although the data warranted further verification.Since HCC tends to be asymptomatic for several months or even years, early diagnosis is very difficult.HCCs are often at the advanced stage or show distant metastasis at diagnosis, such that only 15% -35% of the HCC patients may be amenable to transplant surgery, and that the recurrence rate after transplantation remains high [12 , 13].Therefore, research effort s have been directed towards avoiding risks, lowering postoperative recurrence, and prolonging the survival time of the patients not meeting the specified criteria.Currently, opinions concerning the value of postoperative chemotherapy vary.Some studies [14 , 15]reported that post-LT preventive chemotherapy could extend the overall survival time and improve the tumor-free survival time.In contrast, some studies indicated that preventive chemotherapy was of no value [16 , 17], whereas others reported a stand between the two opinions [5].The present study aimed to evaluate the clinical data of HCC patients within or beyond the Milan or Hangzhou criteria in an attempt to evaluate the advantages of the Hangzhou criteria, to identify independent risk factors for tumor recurrence,and to examine the effect of post-LT prophylactic chemotherapy on HCC recurrence.
Methods
Patients
Our retrospective cohort included 199 patients with primary HCC who had undergone LT between 2005 and 2015.All liver grafts were from deceased donors, and written informed consents were obtained from all recipients before LT.Surgical procedures included standard orthotopic LT and piggyback LT.The immunosuppressive regimen consisted of induction with methylprednisolone,with oral hormones gradually discontinued in the early postoperative period, and tacrolimus/cyclosporine, alone or in combination with mycophenolate mofetil.The follow-up study ended on December 31, 2016.
Twenty variables were collected: sex, age, preoperative total bilirubin, creatinine, intenational normalized ratio (INR), Child-Pugh stage, model for end-stage liver disease (MELD) score, maximum tumor diameter (cm), the number of tumors (≤ 3 and>3), TNM, vascular invasion, preoperative AFP, preoperative treatments including radiofrequency ablation and transcatheter arterial chemoembolization, chronic hepatitis type [hepatitis B virus (HBV)or HCV], presence of cirrhosis, histopathological differentiation,postoperative preventive chemotherapy, the time from surgery to chemotherapy (months), reduction of chemotherapy dose, and postoperative immunotherapy (with or without mycophenolic acid drugs).
Moreover, we analyzed the survival of 199 patients who had undergone LT for HCC in terms of the preoperative compliance with the Milan criteria or Hangzhou criteria [Group 1: within both Milan and Hangzhou (n= 51), Group 2: within the Hangzhou but beyond the Milan criteria (n= 36); and Group 3: beyond both the Milan and Hangzhou criteria (n= 112)].The chemotherapy regimen included gemcitabine and capecitabine (6 cycles) and was administered to patients in Group 2 and 3.Clinical symptoms and periodic laboratory examinations such as blood cell counts and renal function were monitored during every treatment cycle.Once severe toxic side effects occurred, the dosage of chemotherapy was reduced or even discontinued.
Statistical analysis
Results
Child-Pugh stage and HBV infection were independent risk factors for tumor recurrence
The baseline characteristics of the three groups were shown in Table 1.The subjects included 184 males (92.5%) and 15 females(7.5%) with an average age of 46.8 ±9.9 years.Of the patients, 185(93.0%) had a history of HBV infection.
The univariate logistic regression analysis (Table 2) revealed that 11 variables were significantly related to HCC-recurrence after LT (P<0.05), including age, preoperative total bilirubin, INR,Child-Pugh stage, the number of tumors, maximum tumor diameter, chronic HBV infection, preoperative AFP, histopathologic grades,TNM stage, and postoperative preventive chemotherapy.Furthermore, multivariate logistic regression analysis showed that the Child-Pugh stage C (OR = 33.00; 95% CI: 1.088-100.612;P= 0.045)and HBV infection before LT (OR = 4.318; 95% CI: 1.293-14.425;P= 0.017) were positively correlated with the tumor recurrence of patients beyond the Milan criteria but within the Hangzhou criteria (Table 3).Furthermore, the Child-Pugh stage C before LT was positively correlated with the tumor recurrence of patients beyond the Hangzhou criteria (OR = 3.609; 95% CI: 1.101-11.836;P= 0.034; Table 3).
HCC patients within Hangzhou criteria had equal survival to those within Milan criteria
The differences of survival rates were statistically significant among the three groups (P<0.001, Fig.1).However, no significant difference was noted in the survival rate between group 1 and group 2 (P>0.05, Fig.1).
Prophylactic chemotherapy significantly improved the prognosis of patients with HCC after LT
One hundred and seven patients beyond the Milan criteria were originally planned to be treated with preventive adjuvantchemotherapy.However, 41 patients refused to accept or were not tolerant of chemotherapy because of their poor general condition.Multivariate logistic regression analysis showed that postoperative prophylactic chemotherapy reduced the risk of tumor recurrence in HCC patients beyond the Milan and Hangzhou criteria (OR = 0.478;95% CI: 0.308-0.741;P= 0.001; Table 4).For the patients exceeding the Milan and Hangzhou criteria who were treated with preventive adjuvant chemotherapy, the median survival time was 19 months compared to 12 months in those who did not receive any chemotherapy.In the chemotherapy group, the dosage was reduced in 42 patients because of myelosuppression or extreme weakness.Treatment was discontinued in 12 patients, with at least 2 cycles per patient.
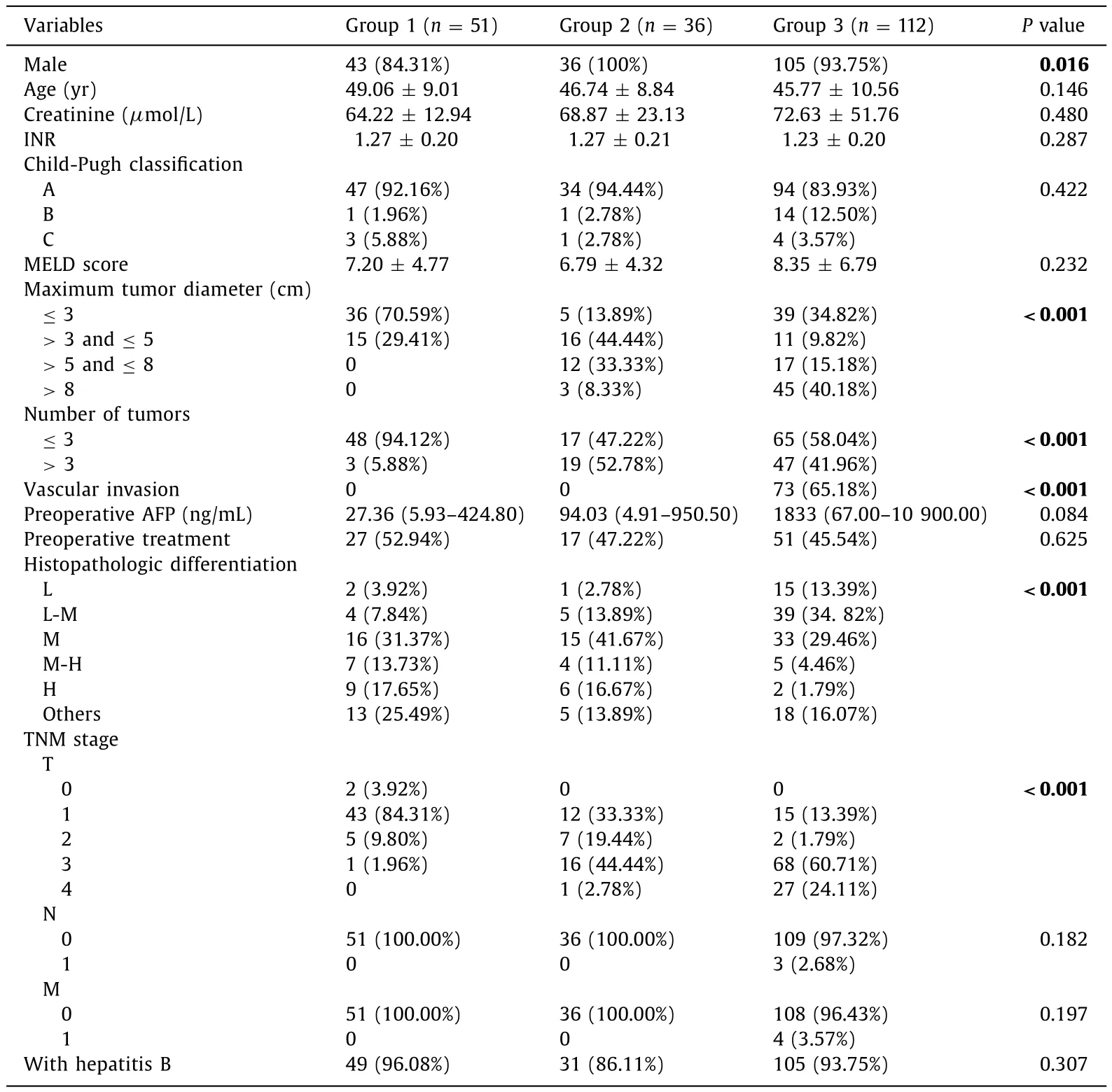
Table 1The baseline pre-transplant characteristics among the different patient groups.
Discussion
To date, LT is the most favorable treatment for HCC and is the treatment of choice for HCC patients complicated with hepatic cirrhosis since it reduces tumor burden and treats the underlying liver disease [5].In this study, 11 factors, including age, Child-Pugh stage, number of tumors, preoperative AFP, HBV, and TNM, were significantly correlated with liver tumor recurrence, which was coincident with the results of previous studies [7 , 18].Additionally,this study was the first to report that the Child-Pugh stage and HBV infection were independent risk factors significantly associated with HCC recurrence in patients beyond the Milan criteria.In Asia, especially in China, HBV infection is the predominant risk factor for the development of HCC and tends to result in a largersized tumor [19 , 20].It has been reported that the age of onset of HCC caused by HBV infection is even smaller [21].
Child-Pugh classification is a common tool for evaluating the liver function of patients with liver diseases [22 , 23].Hepatic dysfunction is associated with longer disease course and greater difficulty in surgery, a larger volume of transfusion, and higher risk of intraoperative tumor metastasis, which increases the possibility of HCC recurrence [24].Previous studies also demonstrated that liver dysfunction and a large volume of transfusion could affect the prognosis [25 , 26].Therefore, we believe that HCC patients with a high Child-Pugh score and HBV infection are not suitable for LT.
Due to the deep location of the liver and absence of pathognomonic symptoms or signs attributable to HCC, HCC usually has a relatively long silent course that renders clinical diagnosis difficult [13].Therefore, most HCC patients miss the opportunity for LT because of late diagnosis and failure to satisfy the Milan criteria or Hangzhou criteria.In our study, patients exceeding these criteria were included at the time of transplant registration, but exceeded the criteria according to the postoperative pathology examination in surgical resection specimens because of the long time waiting for LT.In the past decade, of the 199 HCC patients admitted to our center, 25.6% met the Milan criteria and 43.7% sat-isfied the Hangzhou criteria.Our study showed that the overall survival (OS) was significantly lower in patients beyond the Milan criteria and Hangzhou criteria than in those within these criteria.Nonetheless, the OS of patients beyond the Milan criteria but within the Hangzhou criteria was similar to those within the Milan criteria.This result was consistent with those of several other centers [8 , 10 , 27 , 28].Our intensive study suggested that the Hangzhou criteria worked just as well as the Milan criteria.
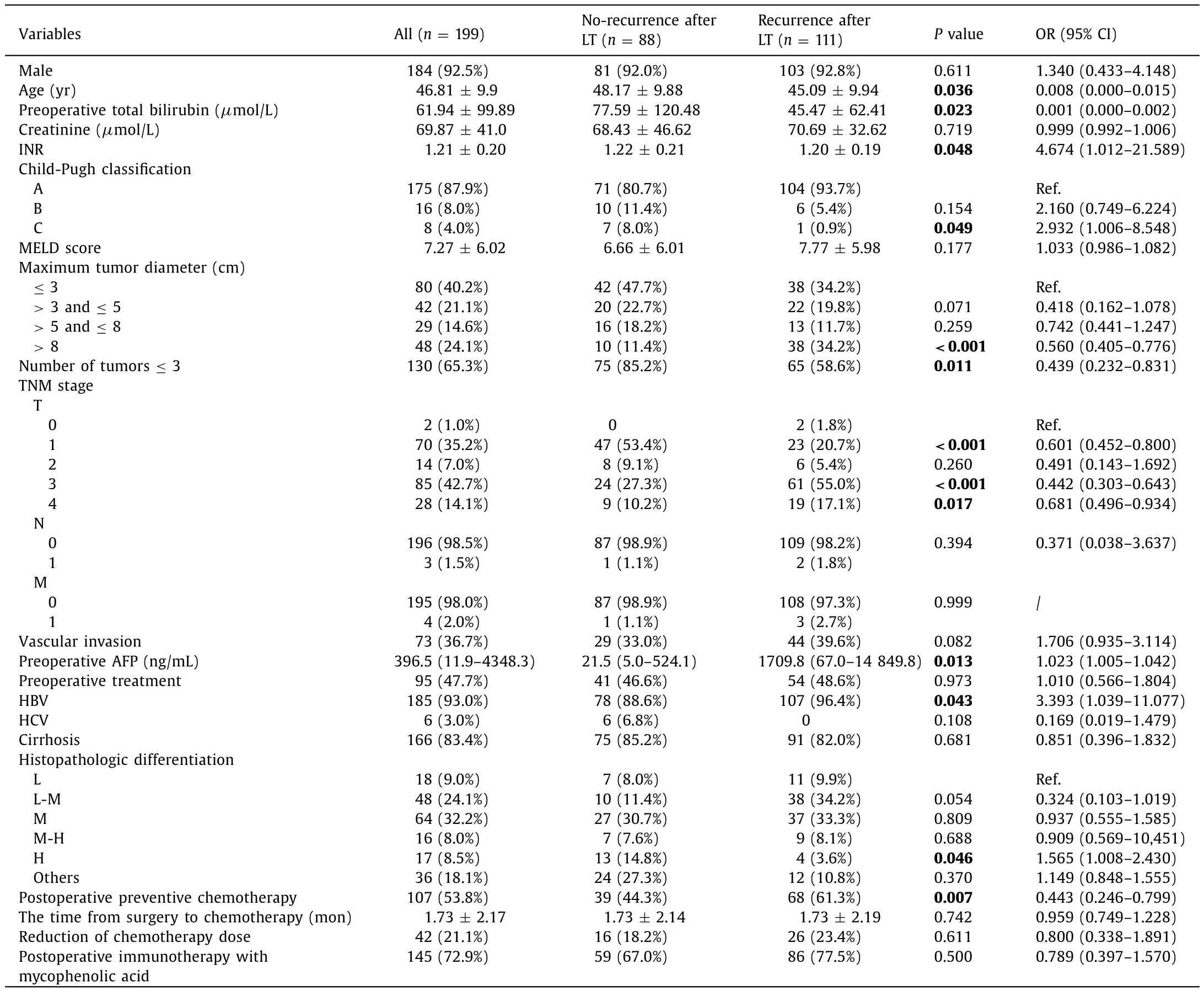
Table 2Univariate analysis of risk factors related to post-LT recurrence.

Table 3Risk factors on tumor recurrence after LT in patients exceeding Milan criteria.

Table 4Effects of preventive adjuvant chemotherapy on tumor recurrence in patients with HCC afterLT beyond Milan criteria.
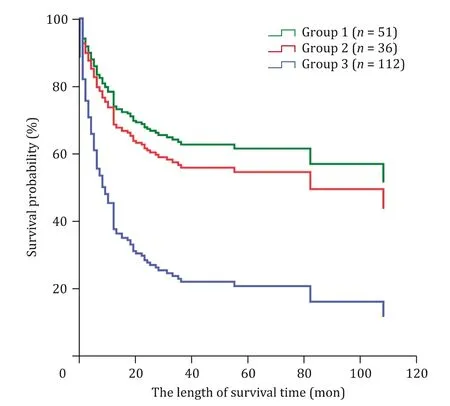
Fig.1.Multivariate Cox regression analysis for overall survival of 199 patients.Among three groups adjusted by the factors of Child-Pugh stage and HBV infection,significant difference in overall survival was observed (P < 0.001).Furthermore, no significant difference in the survival rate between group 1 (within both the Milan and Hangzhou criteria) and group 2 (beyond the Milan criteria but within the Hangzhou criteria) was found (P > 0.05).
Another important finding is that the combined treatment of gemcitabine with capecitabine reduced the risk of tumor recurrence and prolonged the survival time for HCC patients beyond the Hangzhou criteria.Our study was in line with others, which also demonstrated that preventive chemotherapy after LT could significantly reduce the risk of HCC recurrence [14 , 15].Capecitabine can induce apoptosis of tumor cells, and gemcitabine, an analog of cytarabine, can inhibit the synthesis of DNA and further suppress tumor growth [29-31].Thus, in theory, combined use of gemcitabine and capecitabine can specifically kill or suppress tumor cells that metastasize, preoperatively or intraoperatively, into the blood, lungs, and bones.Therefore, we believe that preventive chemotherapies for HCC recurrence after LT are useful.However, some researchers argue that due to the multidrug resistance of HCC cells, post-LT chemotherapy is of no value in HCC patients [16 , 17].Our data clearly support the application of post-LT chemotherapy to HCC patients beyond Hangzhou criteria.
Immediately after this he was called upon, and swam through the sea up the river to where the troll stood on the bank and restored him to human shape with the same words as before
In conclusion, this study indicated that 1) liver dysfunction and HBV infection affect the prognosis of LT in the patients exceeding the Milan criteria; 2) the Hangzhou criteria work equally to the Milan Criteria; and 3) preventive chemotherapy post-LT for HCC patients beyond the Milan and Hangzhou criteria reduces the risk of tumor recurrence and prolongs the survival time.
Acknowledgment
None.
CRediT authorship contribution statement
Mei-Xi Wang:Data curation, Writing - original draft.Dong Chen:Resources, Writing - review & editing.Yuan-Yuan Zhao:Methodology, Formal analysis.Bo Yang:Methodology, Formal analysis.Ji-Pin Jiang:Resources, Writing - review & editing.Fan-Jun Zeng:Resources, Writing - review & editing.Lai Wei:Conceptualization, Supervision, Funding acquisition, Writing - review & editing.Zhi-Shui Chen:Funding acquisition, Supervision, Writing - review & editing.
Funding
This study was supported by grants from the National Natural Science Foundation of China (No.81770652) and Science and Technology Foundation of Hubei Province (No.2017ACA096 and WJ2017Z011).
Ethical approval
The study was approved by the Ethical Board of Tongji Medical College of Huazhong University of Science and Technology.All the patients enrolled have signed the written informed consent.
Competing interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
杂志排行

Hepatobiliary & Pancreatic Diseases International的其它文章
- Endoscopic papillary large balloon dilation with or without sphincterotomy for large bile duct stones removal: Short-term and long-tem outcomes
- Two-in-one: A pooled analysis of primary hepatic neuroendocrine carcinoma combine d/collide d with hepatocellular carcinoma
- A ten-year experience of inferior vena cava reconstruction for malignancy: The importance of a multidisciplinary approach with hepatobiliary surgery
- New variation of median arcuate ligament compression causing hepatic arterial hypoperfusion during liver transplantation
- Echinococcus granulosus: A novel parenchymal sparing surgical treatment
- Serum chitinase-3-like protein 1 is a biomarker of liver fibrosis in patients with chronic hepatitis B in China