Lesson Ninety- five A narrow complex tachycardia with atrioventricular dissociation:What is the mechanism?
2020-06-18童鸿
Case Presentation
A 74-year-old woman underwent diagnostic electrophysiologic study because of recurrent,symptomatic supraventricular tachycardia. Baseline atrio-His1and His-ventricular intervals measured 75 ms and 50ms, respectively. Programmed atrial extrastimu-lation elicited dual atrioventricular(AV)nodal physiology and ventricular pacing showed no ventriculoatrial conduction despite isoproterenol. Figure 1 shows her clinical tachycardia. The response of tachycardia to a His-refractory ventricular premature depolarization (VPD)is shown in the top section of Figure 2, while its induction twice by rapid ventricular pacing(340 ms)is shown in the middle and bottom sections of Figure 2. Based on these observations, what is the mechanism of tachycardia?
Discussion
Figure 1 shows a narrow complex tachycardia with AV dissociation, the differential diagnosis of which includes the following: (1)junctional ectopic tachycardia(JET)with junctional-atrial block,(2)AV nodal reentrant tachycardia (AVNRT) with upper common final pathway block,(3)orthodromic reentrant tachycardia (ORT)using either a nodofascicular(NF)or nodoventricular (NV)bypass tract (BPT)with nodal-atrial block, and (4) intra-Hisian reentrant tachycardia. The absence of split His bundle potentials excludes intra-Hisian reentry. Tachycardia also shows cycle length alternans, which can be explained by JET with 3:2 exit block from an automatic focus or alternating antegrade conduction over 2 AV nodal pathways during ORT- NF/NV(eg, fast [FP] and slow[SP]) or during AVNRT. Another narrow complex tachycardia associated with cycle length alternans is dual antegrade response tachycardia resulting from simultaneous conduction over the FP and SP of the AV node after each sinus beat("double fire"),but the wide variability in"AH"intervals that do not reliably precede and predict His-His intervals argues against this diagnosis. Although atrial overdrive pacing and the delivery of single atrial premature depolarizations can differentiate JET from AVNRT, these maneuvers are limited in the presence of complete AV dissociation.Figure 2 (Top)shows a His-refractory VPD that resets tachycardia with delay of the subsequent His bundle(indicated by an asterisk), proving the presence of a concealed NF/NV BPT but not necessarily its participation in tachycardia. Such a finding, however,effectively excludes pure JET, AVNRT, and dual antegrade response tachycardia. Though the delay could occur retrogradely in the BPT, it might also occur antegradely in the SP. This is then followed by 1 additional cycle of tachycardia with antegrade conduction over the FP, resulting in the shortest His-His interval on the tracing followed by tachycardia termination. (Alternatively, the second VPD[spontaneous,but also His-refractory] advances the His bundle over the BPT-FP). Further proof of the existence of a BPT is shown with tachycardia induction(Figure 2, Middle). During pacing, 2 consecutive His bundle electrograms occur at the pacing cycle length shortly after the second and third pacing stimuli.Although these could be retrograde His bundle potentials, the His bundle's absence after the fourth pacing stimulus would make AVNRT unlikely, as it is not possible to penetrate the AV node and initiate AVNRT without prior retrograde activation of the His bundle. Additionally, the morphology of these His bundle electrograms is identical to those during tachycardia, indicating that they are activated antegradely. A more likely explanation is that these His bundle electrograms are orthodromically activated after long stimulus-His(St-H)intervals(385 ms).Further support for orthodromic activation of the His bundle is that initiation of tachycardia after the last paced complex is associated with a similarly long St-H interval.Orthodromic activation of the His bundle can only occur in the presence of a BPT. Tachycardia induction,however, is associated with a long postpacing interval(PPI)relative to the tachycardia cycle length(TCL)(138 ms)raising the possibility that the mechanism of tachycardia is AVNRT with upper common final pathway block in the presence of a bystander NF/NV pathway that inserts into 1 limb of the AV nodal circuit.A long PPI-TCL, however, can also result from pacing-induced retrograde delay over the nodal portion of the BPT or antegrade delay over the AV node,particularly the SP. The latter explanation supports the findings of the second tachycardia induction(Figure 2,Bottom). The first 2 pacing stimuli orthodromically activate the His bundle over the NF/NV BPT-SP,generating a long St-H interval.The last paced complex,however,orthodromically activates the His bundle with a shorter St-H interval (346 ms)because of NF/NV BPT-FP conduction(thereby also explaining the cycle length alternans during tachycardia), producing a shor PPI-TCL (102ms), which excludes AVNRT and establishes a diagnosis of ORT-NF/NV. Figure 3 depicts the orthodromic activation of the His bundle(arrows)during rapid ventricular pacing by retrograde conduction over a concealed NF/NV BPT and then antegradely over the SP(longer St-H interval)or FP(shorter St-H interval).t
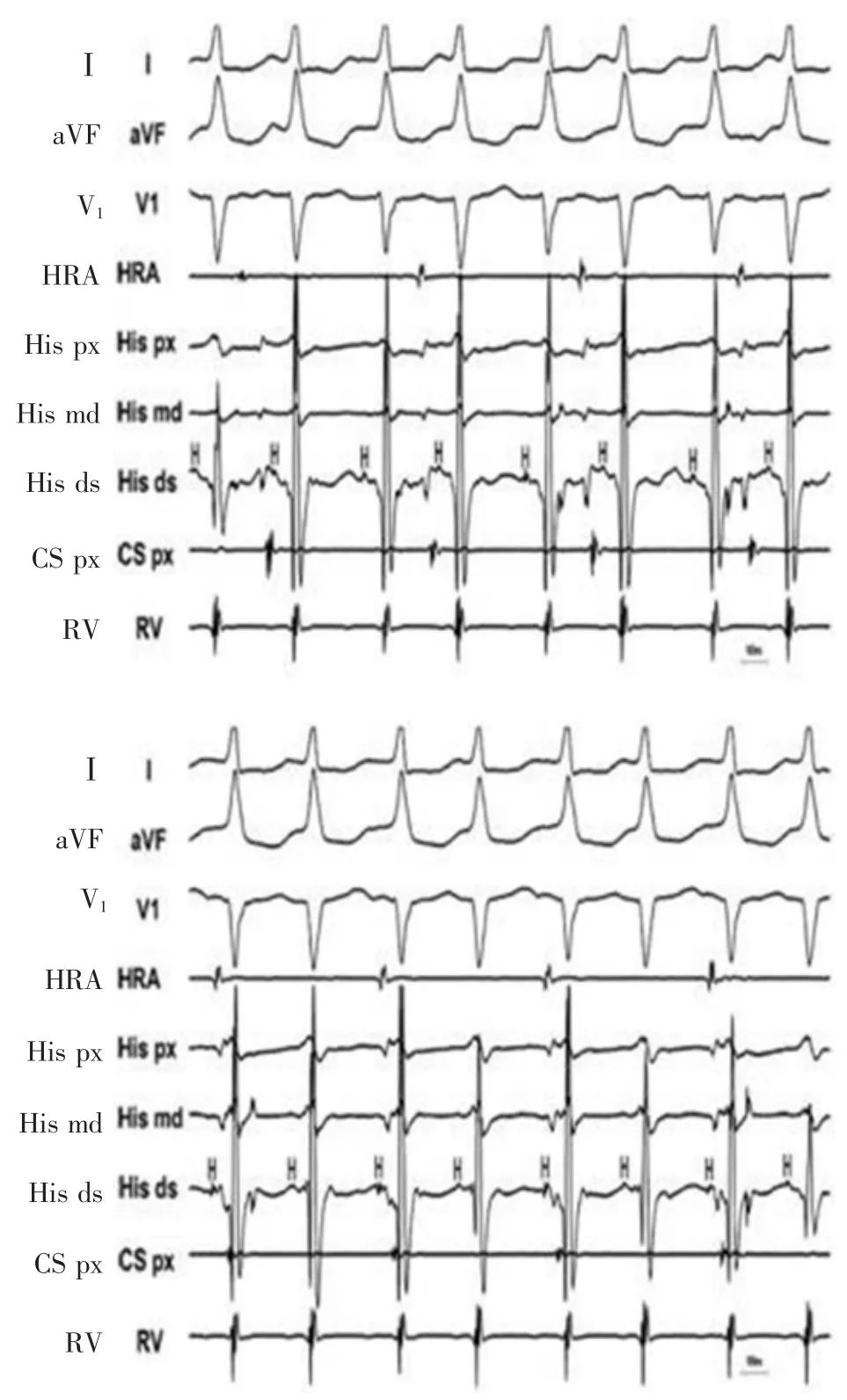
Figure 1 Narrow complex tachycardia with atrioventricular dissociation.

Figure 2 Top: Response of tachycardia to a His-refractory ventricular premature depolarization. Middle,Bottom: Induction of tachycardia by rapid ventricular pacing(340 ms)
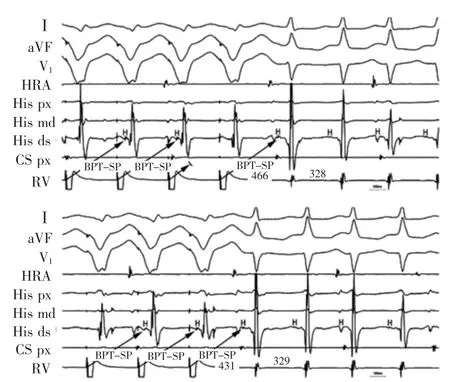
Figure 3 Induction of tachycardia by right ventricular pacing with arrows depicting orthodromic activation of the His bundle (H)over a concealed nodofascicular/nodoventricular bypass tract (BPT) and the slow pathway(SP)(longer stimulus-His interval)or fast pathway(FP)(shorter stimulus-His interval).
The distal insertion(fascicular or ventricular)of the nodal fiber could not be identified. Para-Hisian pacing might differentiate between an NF and NV BPT by demonstrating its dependence upon His-Purkinje vs ventricular activation, respectively, but would be difficult in the absence of ventriculoatrial conduction.Entrainment with manifest fusion(particularly mild or progressive fusion)might favor an NV BPT because entrainment involving an NF BPT requires that paced antidromic wavefronts penetrate the distal Purkinje system to reach the circuit. It is theoretically possible,however, to entrain ORT-NF with manifest fusion if the collision point between antidromic and orthodromic wavefronts occurs in the proximal right bundle between the bifurcation of the His bundle and take-off of the NF BPT from the distal right bundle. In such a situation,paced antidromic wavefronts from the right ventricle would fuse with orthodromic activation of the His bundle-left bundle-left ventricle axis. Manifest fusion was not observed in this case.
In summary, the patient had ORT using a concealed NF/NV BPT with both(1)nodal-atrial block and AV dissociation and(2)dual AV nodal physiology with cycle length alternans. Although the NF/NV BPT could not be mapped, anecdotal cases have shown that its proximal insertion can be in the SP; and, therefore,the patient underwent SP ablation in the right posteroseptal region. During radiofrequency delivery,the integrity of the AV node was monitored by atrial pacing because junctional ectopy was associated with junctional-atrial block. After SP ablation, the patient had no further tachycardia and has remained symptom-free.
词 汇
dissociation n. 脱节,分离
orthodromic adj. 顺向的,顺向性
nodofascicular adj. 房室结-束支的,结-束的
nodoventricular adj. 房室结-心室的,结-室的
antegrade adj. 前进的,顺传的,顺行的
retrogradely adv. 逆向地,后退地,颠倒地
antidromic adj. 逆向的,逆行的
wavefront n. 波阵面,波前
collision n. 碰撞,对立,抵触
manifest n.&adj.&v. (船或飞机的)货单,旅客名单;明显的;显而易见的;表明,显现,使人注意到
anecdotal adj. 逸事的,趣闻的,传闻的
integrity n. 诚实正直,完整,完好
注 释
1.His 指希氏束,又称房室束,是心脏特殊传导系统的重要组成部分,始于房室交接区的房室结,向下延续于室间隔内,在室间隔膜部下缘行走,到达室间隔肌部上缘后分为
左、右束支。
参考译文
第95 课 窄QRS 波群心动过速伴房室分离:机制是什么?
1 例74 岁女性因反复症状性心动过速行诊断性电生理检查。基础状态下心房-希氏束间期和希氏束-心室间期分别为75ms 和50ms。程序心房期外刺激诱发出房室结双径路,而滴注异丙肾上腺素下心室起搏未见室房传导。图1 是她临床发作时的心动过速。图2 上图显示心动过速对希氏束不应期间心室期前除极(VPD)的反应,图2 中图和下图显示快速心室起搏(340ms)二次诱发。基于这些,心动过速的机制是什么?
讨论
图1 显示窄QRS 波群心动过速伴房室分离,鉴别诊断如下:(1)交接区心动过速(JET)伴交接区-心房传导阻滞,(2)房室结折返性心动过速(AVNRT)伴上端最后共同通路阻滞,(3)以结-束(NF)或结-室(NV)为旁道(BPT)的顺传型房室折返心动过速(ORT)伴结-房传导阻滞,(4)希氏束内折返性心动过速。无希氏束分裂电位排除了希氏束内折返。心动过速同时显示周长交替变化,这可解释为源于自律性节点的JET 伴3:2 传出阻滞,或ORT-NF/NV 或AVNRT 时经房室结双径路[即快径路(FP)和慢径路(SP)]交替顺传。窄QRS 波群心动过速伴周长交替的另一种机制是每一窦性节律同时经FP 和SP 传导引起双重反应心动过速(“双发”),但变化不定的“AH”间期既不先于也不能预测希氏-希氏间期,因而不支持这一诊断。虽然心房超速起搏或单一的心房期前刺激能鉴别JET 和AVNRT,但因存在完全性房室分离而使这些方法受限。图2(上图)显示希氏束不应期VPD 重整心动过速伴延迟的希氏束电位(星标),证实存在隐匿性NF/NV BPT,但未必证实它参与心动过速。不过,这一发现有效地排除了单纯性JET、AVNRT 和双重顺传的心动过速。虽然延迟可发生于旁道的逆传,但也可发生于慢径的顺传。其后为一与心动过速不同的波,经快径顺传而产生描记到的最短希氏-希氏间期,随后心动过速中止[或许,第2 个VPD(自发的,但也是处于希氏不应期的)经旁道-快径而激动希氏束]。BPT 存在的进一步依据出现在心动过速诱发中(图2,中图)。起搏期间,在第2 个和第3 个起搏刺激后紧随的起搏周长内出现2个连续的希氏束电图。虽然这些可以是逆传的希氏束电位,但第4 个起搏刺激后无希氏束电位,使得AVNRT 的诊断不能成立,因为没有先前的逆向希氏束激动,不可能穿越房室结并引起AVNRT。另外,这些希氏束电图与心动过速时相一致,表明是顺传激动的。更有可能的解释是这些希氏束电图是在长起搏刺激-希氏束电位(St-H)间期(385ms)后顺向激动的。进一步支持希氏束顺向激动的是最后一个起搏波后心动过速的起始伴随一类似的长St-H 间期。只有存在旁道时才能顺向激动希氏束。然而,诱发心动过速的起搏后间期(PPI)超出心动过速周长(TCL)138ms,这增大了下述心动过速机制的可能性,即AVNRT 伴上端共同最后通路阻滞合并存在NF/NV BPT 插入房室结折返环的一条径路。不过,长PPI-TCL 也可由起搏逆传旁道结部延迟或房室结顺传延迟所引起,特别是慢径。后一种解释支持第2 个心动过速诱发中所见(图2,下图)。前两个起搏刺激经NF/NV BPT-SP 顺向激动希氏束,产生长St-H 间期。最后一个起搏激动希氏束伴随较短的St-H 间期(346ms),这是因为经NF/NV BPTFP 传导产生短PPI-TCL(102ms)(这也可解释心动过时的周长交替),这排除了AVNRT 从而确立ORT-NF/NV 的诊断。图3 描述快速心室起搏时经隐匿性NF/NV BPT 逆传顺向激动希氏束(箭头标记),随后经SP(较长St-H 间期)或FP(较短St-H 间期)顺传。
无法确定房室结纤维远端插入部位(束支或心室)。希氏束旁起搏通过证实其依赖希氏-浦肯氏还是心室激动而鉴别NF 和NV BPT,但在缺乏室房传导时是难以实施的。拖带伴显见的融合(特别是轻度或进行性融合)倾向于NV BPT诊断,因为涉及NF BPT 的拖带需要起搏的逆传波面穿透浦肯氏远端达到折返环。然而,当逆传和顺传波面之间碰撞点位于希氏束分叉与右束支远端NF BPT 起点之间的右束支近端时,拖带NF BPT 伴显见的融合理论上是有可能的。在此情况下,来自右心室的起搏逆传波面将与希氏束-左束支-左心室的顺传波融合。该病例未见明显的融合波。
总之,该患者为利用隐匿性NV/NV BPT 的顺传型房室折返性心动过速,同时伴(1)房室结-心房阻滞和房室分离和(2)房室结双径路呈周长交替。虽然不能标测NF/NV BPT,但既往的病例表明其近端插入可以位于SF,因此,在右后间隔区域对患者实施SF 消融。因为存在房室结-心房传导阻滞,消融放电过程中,通过心房起搏监测房室结的传导功能。SP 消融后,患者再无心动过速发作而维持无症状状态。
图1窄QRS 波群心动过速伴房室分离。
图2上图:心动过速对希氏束不应期室性期前除极的反应。中、下图:快速心室起搏(340ms)诱发心动过速。
图3右心室起搏诱发心动过速,箭头标记显示经隐匿性结-束/结-室旁道(BPT)和慢径路(SP)(较长的刺激信号-希氏波间期)或快径路(FP)(较短的刺激信号-希氏波间期)顺向激动希氏束。