Lysyl oxidase and hypoxia-inducible factor 1α: biomarkers of gastric cancer
2019-05-08YaLinHanLiChenRuiQinGuanQingWangXiaoHuaLinGuangHaiDai
Ya-Lin Han, Li Chen, Rui Qin, Guan-Qing Wang, Xiao-Hua Lin, Guang-Hai Dai
Abstrac t BACKGROUND Gastric cancer (GC) is one of the main causes of cancer mortality worldwide.Recent studies on tumor microenvironments have shown that tumor metabolism exerts a vital role in cancer progression.AIM To investigate whether lysyl oxidase (LOX) and hypoxia-inducible factor 1α(HIF1α) are prognostic and predictive biomarkers in GC.METHODS A total of 86 tissue and blood samples were collected from 140 patients admitted to our hospital between August 2008 and March 2012. Immunohistochemical staining was performed to measure the expression of LOX and HIF1α in tumor and adjacent tissues collected from patients with GC. Real-time quantitative reverse transcription polymerase chain reaction (qRT-PCR) analysis was used to detect the m RNA expression levels of LOX and HIF1α in patients with GC. In addition, single-factor analysis was applied to analyze the relationship between LOX, HIF1α and prognosis of GC.RESULTS Immunohistochemical staining suggested that the expression levels of LOX and HIF1α increased in tumor tissues from patients with GC. QRT-PCR analysis indicated that mRNA expression of LOX and HIF1α was also upregulated in tumor tissues, which was in accordance with the above results. We also detected expression of these two genes in blood samples. The expression level of LOX and HIF1α was higher in healthy controls than in patients with GC. Additional analysis showed that the expression level of LOX and HIF1α was related to the clinicopathological characteristics of GC. Expression of LOX and HIF1α increased experiments.
Key words: Lysyl oxidase; Hypoxia-inducible factor 1α; Gastric cancer; Biomarker;Prognosis
INTRODUCTION
Gastric cancer (GC) is one of the main causes of cancer mortality world wid e[1].Current epidemiological data indicate that the incidence rate and mortality of GC rank among the top three of all malignant tumors[2]. The morbidity of GC rises gradually with age, and people aged 50-70 years account for the majority of cases.There is no gender differences in patients with GC, and the occurrence of GC is related to geographic variation in many countries. The clinical manifestations mainly include stomach ache, abdominal distension, loss of appetite and weight loss[3]. GC at early stages is free of symptoms, and advanced GC or metastasis sites could be pathological diagnosed by endoscopy or endoscopic ultrasound[4-7]. Patients who suffer from GC have a poor quality of life, and the survival rates are reported to be low[8]. As estimated in the statistics of GLOBOCAN 2012, about 410,000 patients are newly found to suffer from the pain caused by GC in China[9]. Among them, 330,000 patients die of tumor-related causes.
While several therapies have emerged in recent years, the effects of chemotherapy and surgery for GC remain limited[10]. These interventions do not improve prognosis,increase survival rate or prolong survival time[11]. In addition, there are disadvantages to current treatment methods, including inconvenience, increased prevalence of complications, and side-effects[12]. It has been reported that many factors are involved in the progression of GC. More seriously, approximately 60% of patients with GC have metastases when they are diagnosed[13]. Furthermore, the outcome of patients with late stage GC is poor, and most die within 1 year. Therefore, determination of predictive biomarkers for early diagnosis of GC is important.
Recent studies on tumor microenvironments have shown that tumor metabolism plays a vital role in cancer progression. The role of the microenvironment in tumor metabolism is currently attracting significant attention. Lysyl oxidase (LOX) and hypoxia-inducible factor 1α (HIF1α) affect the tumor microenvironment, and play a crucial role in cancer occurrence and development[14-18]. LOX is a secreted extracellular matrix protein that plays an important role in remodeling the extracellular matrix and promoting tumor progression. The LOX family comprises the prototypic LOX, as well as LOX-like proteins that are involved in carcinogenesis. LOX is a copper-dependent monoamine oxidase, and its overexpression is related to both poor survival and the development of multiple types of cancers[19-22]. HIF1α is a transcription factor complex that can regulate oxygen tension[23]. In addition, HIF1α can activate or bind to multiple target genes, and can contribute to inflammatory and other d iseases[22,20]. HIF1α accelerates the growth and metastasis of hepatocellular carcinoma[17].
The present study investigated the expression of LOX and HIF1α in patients with GC and d etermined w hether LOX and HIF1α act as p rognostic and p red ictive biomarkers of GC. Research on the interaction betw een cancer and factors in the metabolic microenvironment is necessary to investigate the progression of GC and determine predictive biomarkers. Our study show ed that LOX and HIF1α can act as biomarkers for the diagnosis and prediction of GC.
MATERIALS AND METHODS
Patients and samples
A total of 86 tissue and blood samples w ere collected from 140 patients ad mitted to our hospital between August 2008 and March 2012. The tumor and adjacent tissues w ere obtained from p atients w ith GC. The blood samp les w ere obtained from 80 patients w ith GC and 80 healthy controls. The use of human tissues in this research w as agreed to by the volunteers and their relatives. All participants gave w ritten informed consent. This study w as cond ucted w ith permission from the Institutional Research Ethics Committee of our hospital. GC patients w ere aged > 18 years, and w ere d iagnosed p athologically and clinically w ith GC. Clinicians measured and analyzed the cond itions accord ing to the Resp onse Evaluation Criteria in Solid Tumors.
RNA extraction and cDNA synthesis
Total RNA from tissues and blood samples w as prepared using TRIzol reagent(Invitrogen, Carlsbad, CA, United States). The samples were added to TRIzol for 30 min in a 4 °C refrigerator. Total RNA was extracted from samples using chloroform,isopropanol, 75% absolute ethanol (all from Beijing Shiji Tuoxin Fine Chemical Industry Co. Ltd., Beijing, China) and diethyl-pyrocarbonate-treated water (Biosharp,Heifei City, China). RNA was stored in a - 80 °C freezer. Concentration and purity were measured using a Nanodrop machine (Thermo Scientific, Carlsbad, CA, United States). As described previously, to synthesize cDNAs, PrimeScript RT reagent kits(TaKaRa, Dalian City, China) were purchased and used for reverse transcription(RT)[21]. cDNA synthesis was conducted using a RT apparatus (Applied Biosystems,Foster City, CA, United States). The cDNA samples were stored at - 20 °C, and used for additional analysis.
Real-time quantitative reverse transcription polymerase chain reaction
To determine the expression of LOX and HIF1α in tissues and blood samples from patients with GC, qRT-PCR analysis was performed using SYBR reagents (Vazyme,Nanjing City, China) on an Applied Biosystems Real-Time PCR machine (Thermo Scientific). The cDNAs, SYBR reagents, double-distilled water and corresponding primers were used to measure expression of LOX and HIF1α. In addition, β-actin was used as a housekeeping gene. The sequences of primers used in this study are listed in Table 1.
Immunohistochemistr y
Immunohistochemical staining w as performed as d escribed previously[22,23]. Tissue sp ecimens w ere fixed in 4% p araformald ehyd e, and embed d ed in p araffin for subsequent analysis. Antibodies against LOX, HIF1α and β-actin w ere p urchased from Abcam (Cambrid ge, United Kingd om). The concentrations of p rimary antibodies were 1:500, and the antibodies w ere diluted in phosphate buffer solution.The paraffin blocks w ere incubated w ith these tw o antibod ies that w ere used to monitor the exp ression of LOX and HIF1α in the GC tissues. Tissue sections w ere incubated w ith antibod ies against LOX or HIF1α, and then incubated w ith p eroxid ase-conjugated goat anti-rabbit second ary antibod y (Cell Signaling Technology, Boston, MA, United States). All sp ecimens w ere fixed in 4%paraformaldehyde, embedded in paraffin, and stored in the Department of Pathology at our hospital.
Statistical analysis
All experiments w ere repeated at least three times. Statistical analyses w ere performed with SPSS software (IBM, Armonk, NY, United States). Independent t tests were used for continuous variables, and Pearson's χ2 tests for categorical variables.Logistic regression was used to confirm the relationship between LOX, HIF1α and the development of GC. Analysis of LOX and HIF1α expression was conducted usingGraphPad Prism software. P < 0.05 w as considered statistically significant.
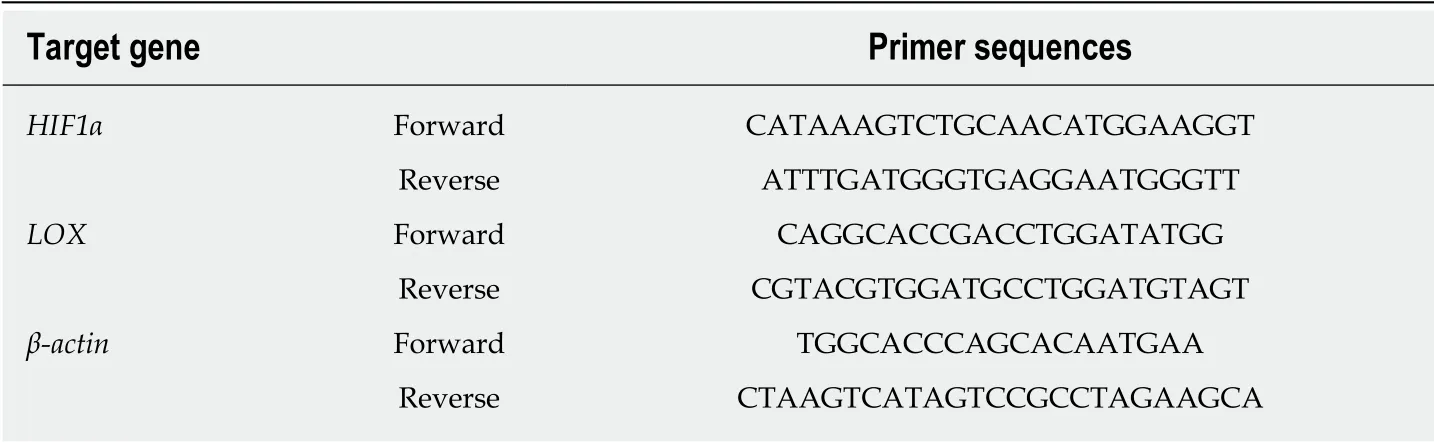
Table 1 Primer sequences
RESULTS
Expression of LOX in patients with GC
Immunohistochemical staining and qRT-PCR analysis were performed to determine whether expression of LOX was dysregulated in tissues and blood samples from patients with GC versus healthy controls. Immunohistochemical staining indicated that LOX was mainly located in the cytoplasm of tumor cells. Most of the cytoplasm of tumor cells exhibited brow n positively stained particles, w hich d isplayed a scattered particle distribution. The same results were seen in the extracellular matrix(Figure 1A). The expression rate of LOX in GC tissues was 40.0% (56/140), which was significantly higher than that in adjacent tissues (18.6%, 26/140) (Figure 1A). QRTPCR showed that mRNA expression of LOX was markedly increased in GC tissues;about five times higher than in adjacent tissues (Figure 1B). We further detected the expression level of LOX in blood samples from GC patients and healthy controls.Expression of LOX was higher in patients with GC than in the control group (Figure 1C). Taken together, these results suggested that expression of LOX was significantly higher in patients with GC.
Expression of HIF1α in patients with GC
Further analysis was performed to detect expression of HIF1α in patients with GC.Immunohistochemistry revealed that HIF1α was mainly expressed in the nuclei of tumor cells (Figure 2A). The cytoplasm of HIF1α-positive cells presented with a brown color, and HIF1α exhibited occasional limited expression in the cytoplasm(Figure 2A). Scattered light brown granules were revealed by immunohistochemical staining (Figure 2A). The expression rate of HIF1α in GC tissues was 28.6% (40/140),which was significantly higher than in adjacent tissues (12.1%, 17/140). The high expression of HIF1α in tumor compared with adjacent tissues was measured by qRTPCR (Figure 2B). Expression of HIF1α in GC tissues was approximately five times higher than in adjacent tissues (Figure 2B). Additional analysis showed that the later the clinicopathological stage, the higher the expression level of HIF1α in the blood samples (Figure 2C). Thus, we concluded that expression of HIF1α was upregulated in tumor tissues and blood samples from patients with GC.
Correlation between LOX and clinicopathological characteristics of GC
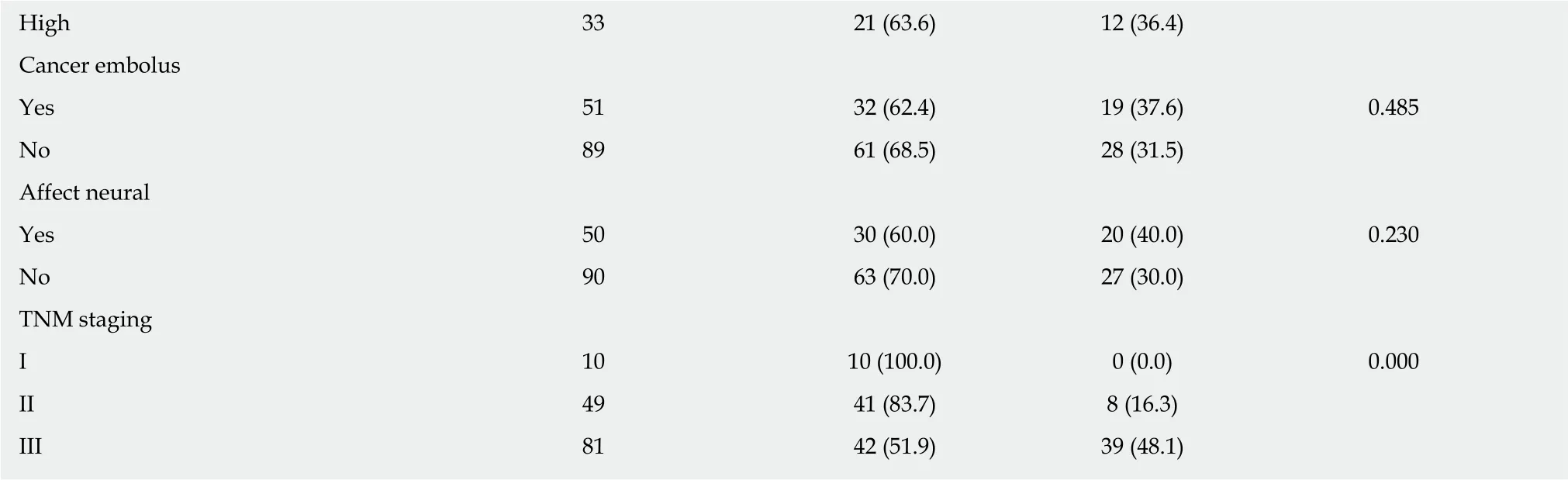
Expression of LOX and clinicopathological characteristics are shown in Table 2. In various groups with different clinical characteristics, expression of LOX was different.Expression of the LOX gene correlated with lymph node metastasis of GC and the tumor-node-metastasis (TNM) stage. The P values for the correlation between LOX expression and lymph node metastasis of GC, between LOX expression and the infiltration depth of GC, and between LOX expression and clinical stage were 0.000,0.005 and 0.000, respectively. When the time of lymph node metastasis was > 16 mo in patients with GC, the rate of high expression of LOX was 100.0%. When the tumor infiltration depth reached T4, the high expression rate of LOX was 54.1%. When the tumor was clinicopathological stage III, the high expression rate of LOX was 55.6%.How ever, expression of LOX did not show any relationship w ith other clinical features, such as age, gender, tumor size, and tumor location. The results showed that the expression of LOX increased with the number of lymph node metastases and the late TNM stage.
Relationship between HIF1α and clinicopathological characteristics of GC
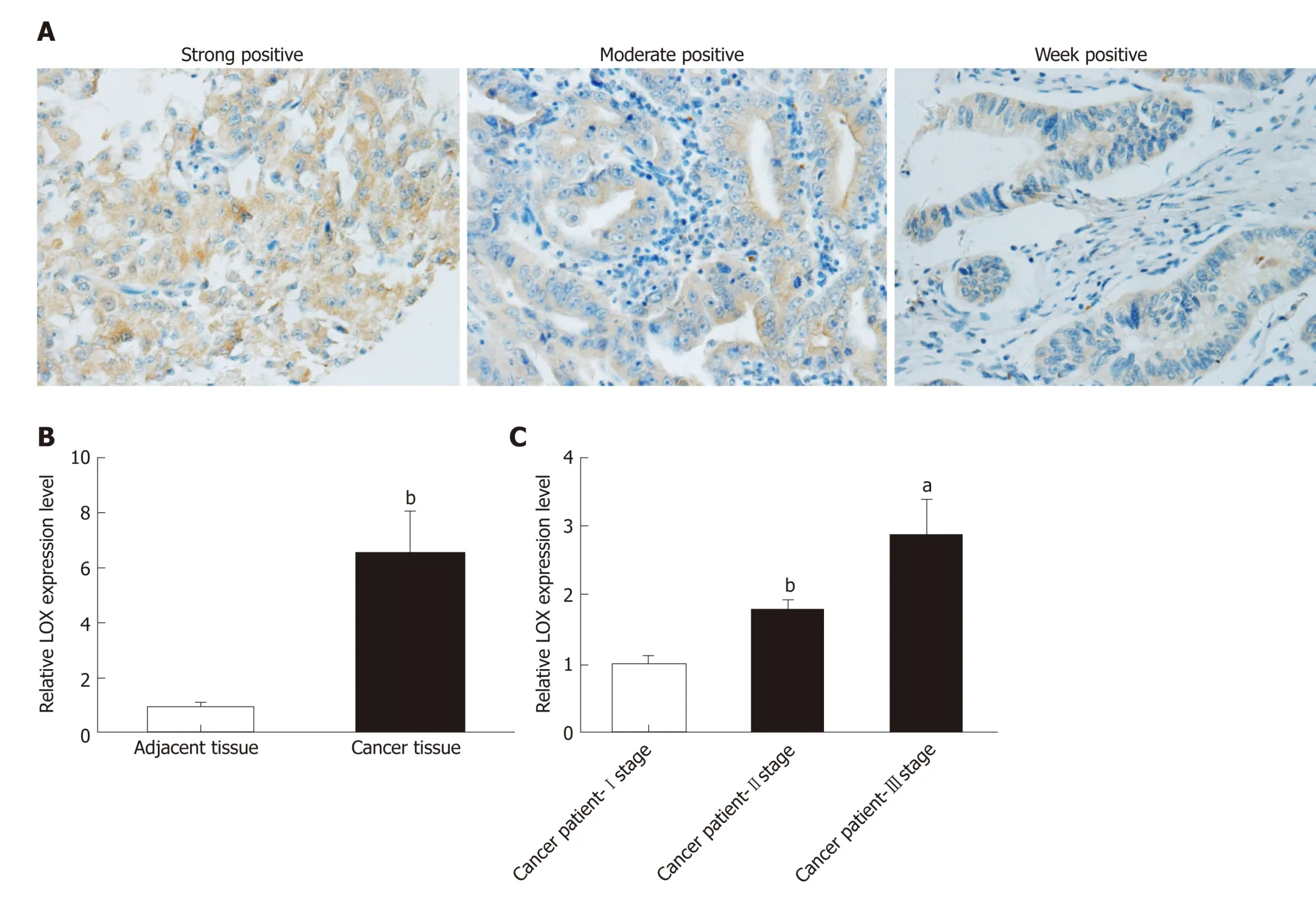
Figure 1 Expression of LOX in GC patients. A: Immunohistochemical staining was used to detect expression of LOX in tumor tissues from patients with GC; B:qRT-PCR was performed to measure mRNA expression of LOX in adjacent tissues and cancer tissues from GC patients; C: qRT-PCR was performed to examine the expression level of LOX in patients with GC. a P < 0.05, b P < 0.01 and c P < 0.001 represent significant difference compared with controls. LOX: Lysyl oxidase; GC:Gastric cancer; qRT-PCR: Quantitative reverse transcription polymerase chain reaction.
Expression of HIF1α and clinicopathological characteristics are show n in Table 3.Expression of HIF1α differed among various groups. Expression of HIF1α was related to lymph node metastasis (P = 0.000). When the time of lymph node metastasis was >16 mo, the rate of high expression of HIF1α was 100.0%. When patients had Borrmann stage IV disease, high expression of HIF1α was 56.8% (P = 0.001). When they had stage III disease, the rate of high expression of HIF1α was 48.1% (P = 0.000). These results suggested that expression of HIF1α correlated with the number of metastatic lymph nodes. However, expression of HIF1α was not associated with other clinical characteristics, such as age, gender, tumor size, and tumor location.
Relationship between expression of LOX and prognosis of GC
Single-factor analysis show ed that d isease-free survival (DFS) in the LOX-low expression group w as 26.7 mo, which was significantly longer than in the LOX-high expression group at 15.6 mo (P = 0.037) (Figure 3A and Table 3). Overall survival (OS)of patients in the LOX-low expression group w as significantly longer than that in the LOX-high exp ression group (P = 0.033) (Figure 3B and Table 3). These results demonstrated that high expression of LOX was associated with poor prognosis.
Relationship between expression of HIF1α and prognosis of GC
To determine the correlation betw een HIF1α expression and the prognosis of GC, we focused on DFS and OS in patients w ith d ifferent levels of HIFα expression. Singlefactor survival analysis show ed that DFS and OS in the HIF1α-low expression group were 26.9 mo and 40.2 mo, respectively, which w ere significantly longer than in the HIF1-high expression group at 14.0 mo and 20.4 mo (both P = 0.03) (Figure 4A, 4B and Table 4). High expression of HIF1α w as associated with poor prognosis.
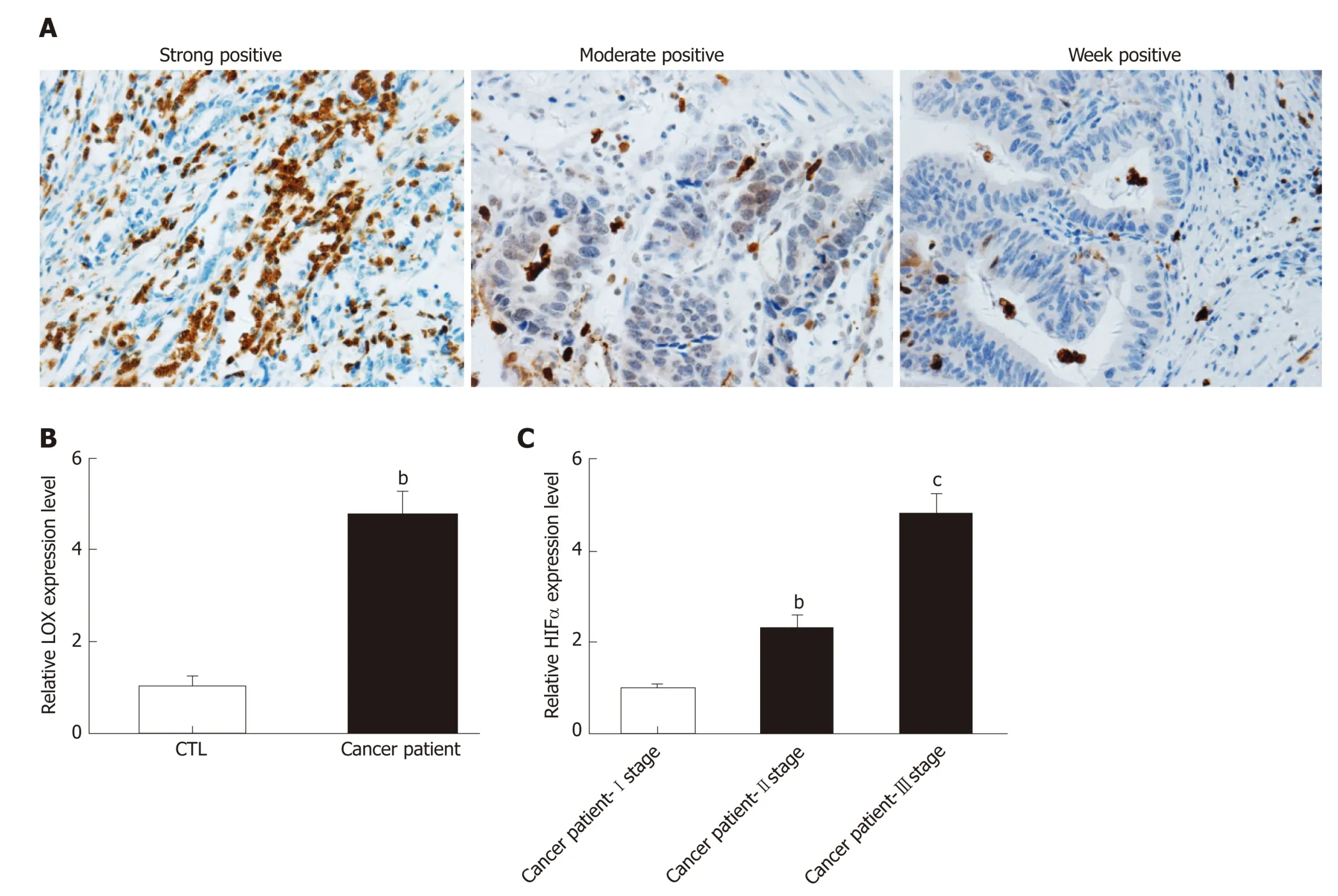
Figure 2 Expression of HIF1α in patients with GC. A: Immunohistochemical analysis of HIF1α in tumor tissues from patients with GC; B: qRT-PCR was applied to study the expression level of HIF1α in GC patients; C: qRT-PCR was used to detect the level of HIF1α in both cancer patients. a P < 0.05, b P < 0.01 and c P < 0.001 represent significant difference compared with controls. HIF1α: Hypoxia-inducible factor 1α; GC: Gastric cancer; qRT-PCR: Quantitative reverse transcription polymerase chain reaction.
DISCUSSION
The occurrence of GC has been increasing rapid ly worldwide[24]. GC is related to the presence of tumor-suppressor or tumor-associated genes[25]. There is no accurate and efficient clinical biomarker of GC. Other gastrointestinal biomarkers or early detection method s w ere also not applied in GC[26-28]. Therefore, the aim of our stud y w as to investigate whether LOX and HIF1α could be used as biomarkers of GC.
LOX p articip ates in the osteoclastogenesis of breast cancer, w hich suggests a therapeutic tool for osteolytic bone destruction[21]. MiRNA-31-5p inhibits expression of HIF1α and strengthens the Warburg effect by inhibiting its target HIF-1α inhibitor. In ad d ition, hep atitis transactivator p rotein X accelerates extracellular matrix mod ification by activating the HIF/LOX pathw ay and p romoting the metastasis of hepatocellular carcinoma[13]. Therefore, w e predicted that LOX and HIF1α could act as biomarkers of GC.
In the present study, immunohistochemical staining suggested that expression of LOX and HIF1α increased in tumor tissues from patients with GC. QRT-PCR analysis ind icated that m RNA exp ression of LOX and HIF1α w as up regulated in tumor tissues. We also detected expression of these tw o genes in blood samples. The results revealed that the expression levels of LOX and HIF1α w ere higher in healthy controls than in GC patients. Ad ditional analysis show ed that the expression levels of LOX and HIF1α w ere related to the clinicop athological characteristics of GC. The expression of LOX and HIF1α increased w ith the number of lymph node metastases and the later TNM stage. Single-factor analysis showed that high expression of LOX and HIF1α led to poor prognosis of GC patients.
In conclusion, our results demonstrated that expression of LOX and HIF1α w as higher in patients w ith GC than in healthy controls. Expression of LOX and HIF1α was associated with clinicopathological characteristics and prognosis of GC. Thus, we conclud ed that LOX and HIF1α could be used as p rognostic and p red ictive biomarkers for GC. Our study provided a link betw een LOX, HIF1α and GC, which contributes to the development and progression of GC.

Table 2 Relationship between lysyl oxidase and clinicopathological factors in patients with gastric cancer

HIF1α: Hypoxia-inducible factor 1α; WHO: Word Health Organization; TNM: Tumor-node-metastasis.
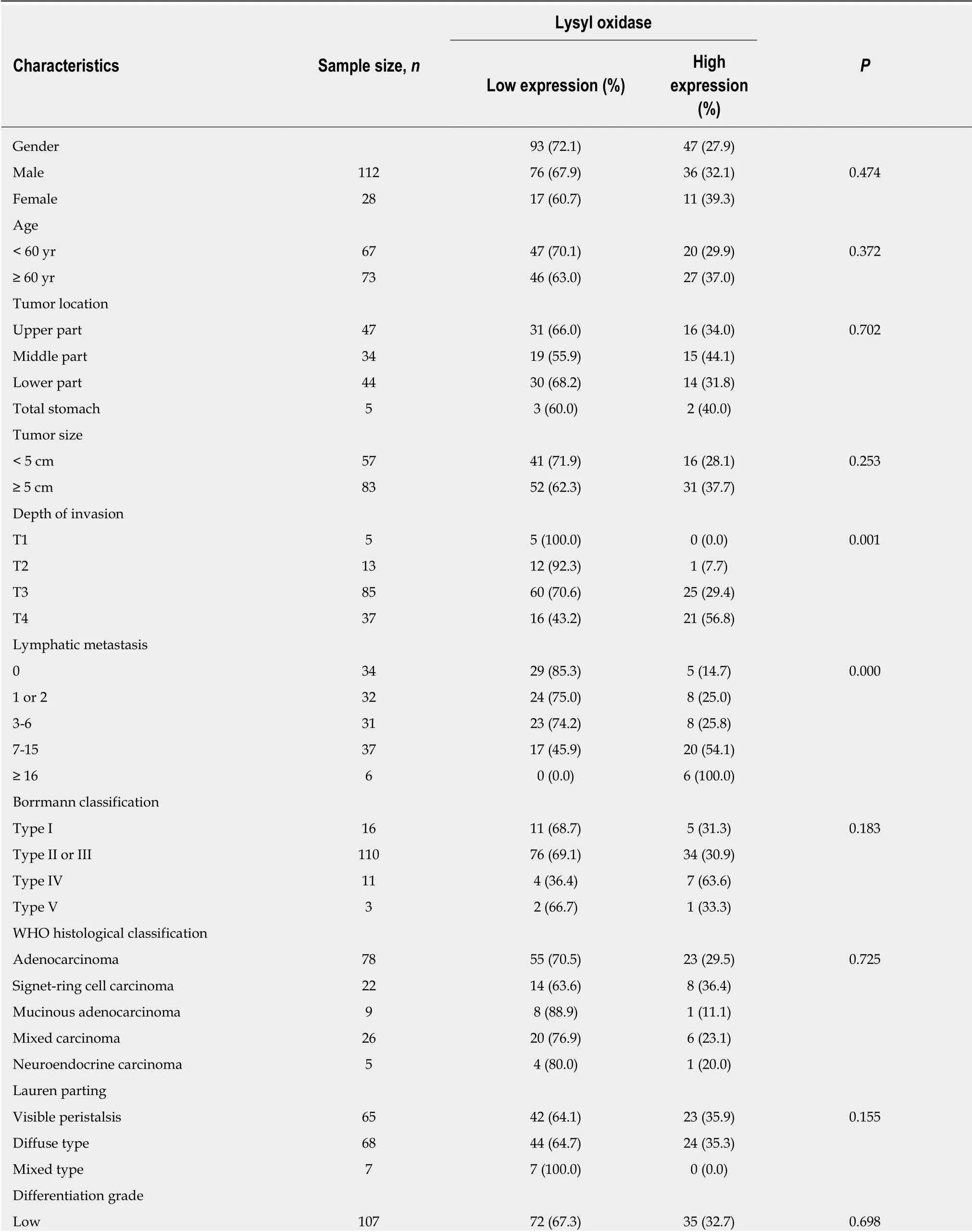
Table 3 Relationship between hypoxia-inducible factor 1α and clinicopathological factors in patients with gastric cancer
WHO: Word Health Organization; TNM: Tumor-node-metastasis.
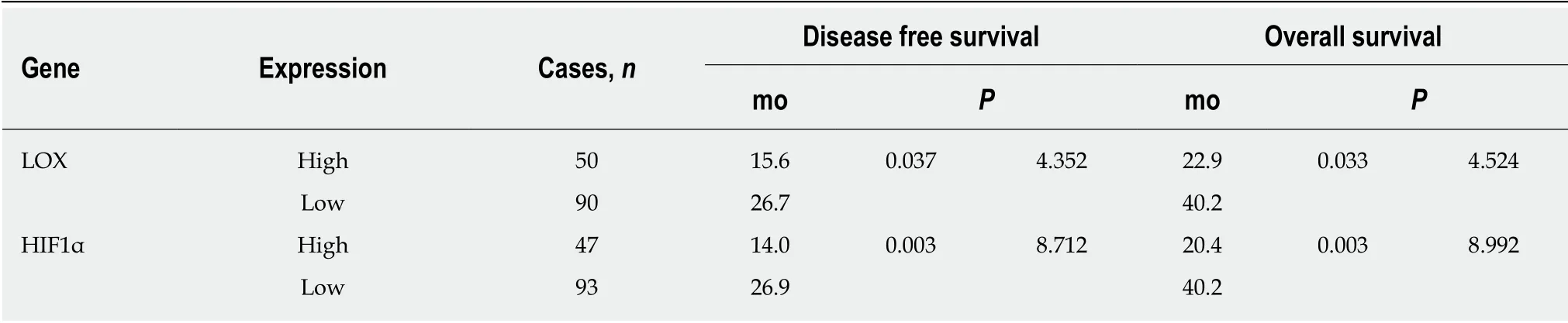
Table 4 Univariate analyses of disease-free survival and overall survival in patients with gastric cancer
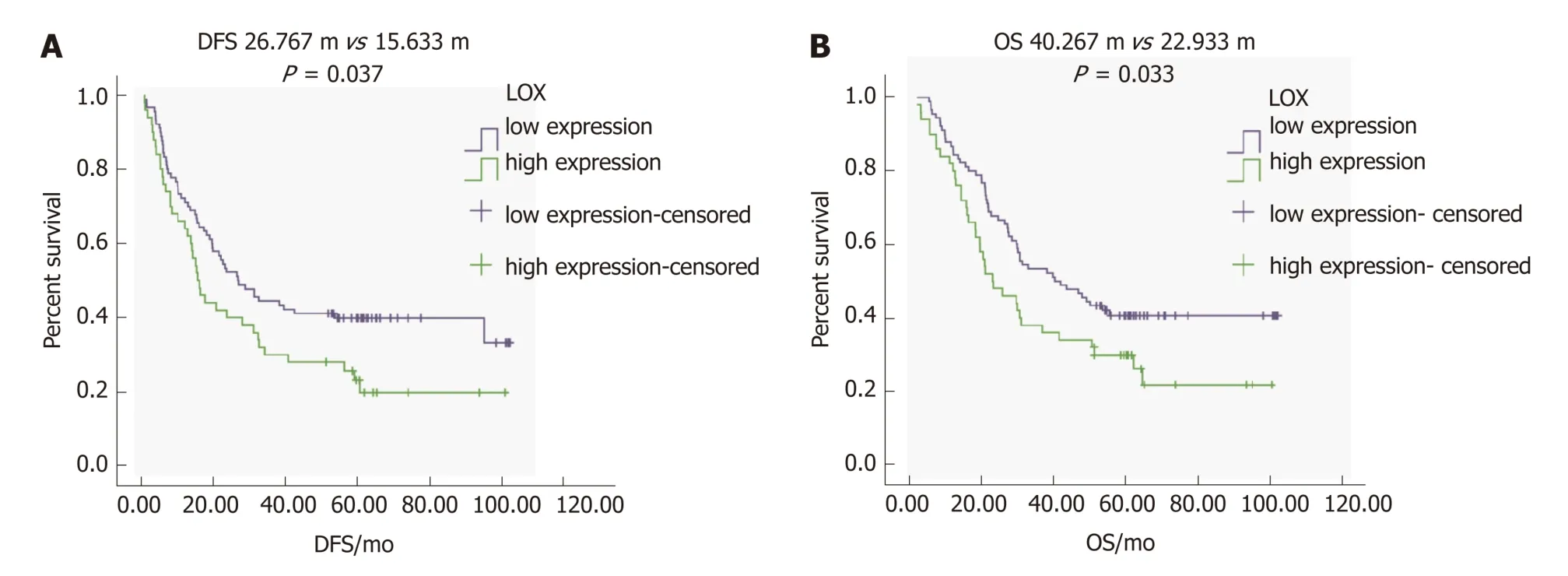
Figure 3 LOX expression is associated with DFS and OS. A: Survival curve of patients with GC with regards to lysyl oxidase expression, a P < 0.05; B: Survival analysis of overall survival and disease-free survival in patients with GC, a P < 0.05. LOX: Lysyl oxidase; GC: Gastric cancer; DFS: Disease-free survival; OS: Overall survival.
Figure 4 HIF1α correlates with poor OS of patients with GC. A: Survival curve of patients with GC with respect to HIF1α expression, a P < 0.05; B: OS curve of patients with GC expressing low and high HIF1α levels. a P < 0.05. GC: Gastric cancer; DFS: Disease-free survival; OS: Overall survival; HIF1α: Hypoxia-inducible factor 1α.
ARTICLE HIGHLIGHTS
Research background
To study whether lysyl oxidase (LOX) and hypoxia-inducible factor 1α (HIF1α) can be used as prognostic and predictive biomarkers in gastric cancer (GC).
Research motivation
To provide the prognostic and predictive biomarkers for treating GC.
Research objectives
To explore the interaction between cancer and factors in the metabolic microenvironment and determine predictive biomarkers of GC.
Research methods
Patients and samples: This work is difficult and requires patient approval.
RNA extraction and cDNA synthesis: Thiswork requires a lot of time, and so the manipulator should be patient. Real-time quantitative reverse transcription polymerase chain reaction (qRTPCR):The manipulator should add the samples accurately during qRT-PCR analysis.
Immunohistochemistry: The experiments take a long time, and the manipulator should perform the experiments step by step.Statistical analysis:All of the experiments were repeated at least three times, and the statistical analysis was then performed.
Research results
The expression levels of LOX and HIF1α increased in the tumor tissues and blood samples of patients with GC. The expression levels of LOX and HIF1α were related to the clinicopathological characteristics and prognosis of GC.
Research conclusions
LOX and HIF1α can be used as prognostic and predictive biomarkers for the treatment of GC.Our study indicated that the expression of LOX and HIF1α was upregulated in patients with GC compared with the control group. In addition, the expression of LOX and HIF1α was related to the clinicopathological characteristics and prognosis of GC.
Research perspectives
The present study suggested that LOX and HIF1α might be used as both prognostic and predictive biomarkers for GC, and provided a link between LOX, HIF1α and GC.
ACKNOWLEDGEMENTS
We appreciate the technical support and help from the Tumor Center Laboratory of PLA General Hospital.
杂志排行
World Journal of Gastroenterology的其它文章
- Repurposing drugs to target nonalcoholic steatohepatitis
- Central role of Yes-associated protein and WW-domain-containing transcriptional co-activator with PDZ-binding motif in pancreatic cancer development
- Considerations of elderly factors to manage the complication of liver cirrhosis in elderly patients
- Predictive and prognostic implications of 4E-BP1, Beclin-1, and LC3 for cetuximab treatment combined with chemotherapy in advanced colorectal cancer with wild-type KRAS: Analysis from real-world data
- Extract of Cycas revoluta Thunb. enhances the inhibitory effect of 5-f luorouracil on gastric cancer cells through the AKT-mTOR pathway
- Unconjugated bilirubin alleviates experimental ulcerative colitis by regulating intestinal barrier function and immune inflammation