安陆德免荷一号矫形器治疗内侧膝关节骨关节炎的研究
2017-06-01周峰张菲王会祥邓国英吴晓明王秋根王谦王建东
周峰 张菲 王会祥 邓国英 吴晓明 王秋根 王谦 王建东
安陆德免荷一号矫形器治疗内侧膝关节骨关节炎的研究
周峰 张菲 王会祥 邓国英 吴晓明 王秋根 王谦 王建东
目的评估安陆德免荷一号矫形器对内侧膝骨关节炎患者活动、疼痛、膝关节功能、日常生活以及生活质量的影响。方法36 例骨关节炎患者。按平均、计算机随机、双盲方法将患者分为 A、B、C 三组。A 组以安陆德免荷一号矫形器加非甾体抗炎药 ( non-steroidal antiinflammatory drugs,NSAIDs ) 美洛昔康联合治疗,B 组单用安陆德免荷一号矫形器治疗,C 组单用美洛昔康治疗,每组 12 例。从入组起,每 3 周门诊随访,通过 Lysholm 膝关节评分表、KOOS 评分表、SF-12 生活质量评价量表、过去 24 h VAS 疼痛评分表以及 Tegner 活动积分表对患者进行评估,总疗程为 12 周。结果( 1 ) 治疗后 12 周,A 组患者 Lysholm 膝关节评分:85.64±4.74,KOOS 评分症状:73.17±8.29、疼痛:70.33±5.96、日常生活:77.08±4.32、体育及娱乐:81.67±5.77、生活质量:80.58±5.76,SF-12 生活质量评分:19.08±1.88,过去 24 h VAS 疼痛评分 1.25±0.754,Tegner 活动积分:7.45±1.08,各项评分较开始改善显著,差异有统计学意义 ( P<0.05 )。B 组患者 Lysholm 膝关节评分:85.33±4.68,KOOS 评分症状:71.33±10.63、疼痛:68.83±5.01、日常生活:75.92±5.18、体育及娱乐:80.00±7.07、生活质量:78.17±6.63,SF-12 生活质量评分:18.83±2.52,过去 24 h VAS 疼痛评分 1.4±0.809,Tegner 活动积分 7.55±1.31,各项评分较开始改善显著,差异有统计学意义 ( P<0.05 )。C 组患者 Lysholm 膝关节评分:76.17±5.557,KOOS 评分症状:60.92±7.75、疼痛:57.67±8.69、日常生活:68.17±4.61、体育及娱乐:70.00±8.53、生活质量:69.33±8.24,SF-12 生活质量评分:14.18±1.81,过去 24 h VAS 疼痛评分 2.2±0.669,Tegner 活动积分:4.36±0.91,各项评分较开始改善显著,差异有统计学意义 ( P<0.05 )。B 组评分与 A 组差异无统计学意义 ( P≥0.05 ),疗效较 C 组显著,差异有统计学意义 ( P<0.05 )。( 2 ) 从整体趋势而言:C 组患者症状好转快,最终疗效不如 A、B 组。B 组起效慢,最终疗效比 C 组好。A 组起效快,最终疗效较 C 组好,但与 B 组差异无统计学意义 ( P≥0.05 )。( 3 ) 使用后3 周,C 组患者 Lysholm 膝关节评分:71.08±7.63,KOOS 评分症状:56.25±12.22、疼痛:41±10.24、日常生活:55.5±10.7、体育及娱乐:57.08±14.22、生活质量:55.5±10.7,SF-12 生活质量评分:10.92±2.11,过去 24 h VAS 疼痛评分 2.08±1.08,Tegner 活动积分:3.67±1.23,较疗效较 B 组显著,差异有统计学意义 ( P<0.05 ),C 组与 A 之间差异无统计学意义 ( P≥0.05 )。( 4 ) 使用后 6 周,A 组 Lysholm 膝关节评分:81.25±8.95,KOOS 评分症状:69.5±11.33、疼痛:62.5±9.8、日常生活:69.5±9.35、体育及娱乐:72.92±10.97、生活质量:69.5±9.35,SF-12 生活质量评分:16.58±2.84,过去 24 h VAS 疼痛评分 1.58±0.79,Tegner 活动积分:6.58±1.56,疗效明显优于 C 组,差异有统计学意义 ( P<0.05 ),C 组疗效较 3 周前差异无统计学意义 ( P≥0.05 ),但与 B 组相比疗效差异有统计学意义 ( P<0.05 )。( 5 ) 在第 9 周时,A 组 Lysholm 膝关节评分:85.08±4.91,KOOS 评分症状:71.17±10.53、疼痛:65.67±7.33、日常生活:72.42±6.1、体育及娱乐:77.5±7.54、生活质量:72.42±6.1,SF-12 生活质量评分:18.92±2.07,过去 24 h VAS 疼痛评分 1.46±0.54,Tegner 活动积分:7.42±0.9,疗效明显优于 C 组,差异有统计学意义 ( P<0.05 );C 组疗效较第 6 周差异无统计学意义 ( P≥0.05 ),且与 B 组疗效差异无统计学意义 ( P≥0.05 )。结论( 1 ) 安陆德免荷一号骨关节炎矫 形器治疗内侧膝骨关节炎具有较好的疗效。( 2 ) 单独使用安陆德一号骨关节炎矫形器起效较 NSAIDs 缓慢,但最终能全面改善患者症状、膝关节功能、日常生活以及生活质量。( 3 ) 矫形器联合使用 NSAIDs 在短期内可以缓解疼痛症状,且最终治疗效果良好,但最终疗效与单用矫形器差异无统计学意义。
骨关节炎,膝;矫正装置;临床方案;队列研究;前瞻性研究
膝关节骨关节炎是中老年人常见慢性疾病[1-2],它会引起关节疼痛导致关节活动受限,进一步导致残疾[3]。据统计,2008 年美国有 2700 万成年人患有骨关节炎[1]。而且随着社会老龄化,膝关节骨关节炎发病率呈不断上升趋势。
作为一种常见的慢性骨骼、肌肉系统疾病,膝关节骨关节炎发病机制尚不完全清楚,已知的机制涉及关节面磨损,关节炎症,关节软骨退变,骨质结构重塑以及骨赘形成[4-6]。其它因素包括老化,肥胖和遗传易感性也促成骨关节炎的发生[7]。
膝关节骨关节炎的治疗方案有很多,保守治疗包括服用药物治疗、物理治疗、生物力学治疗[8],手术治疗包括截骨术、关节镜清扫以及人工膝关节置换术[9-11]。单纯截骨术改善膝关节不稳疗效不显著,且较之保守治疗来说创伤大,制动时间长,且存在截骨不愈合等问题,可能后期行膝关节置换术[12]。关节镜清扫能缓解关节炎临床症状[10],但无法纠正膝关节力线,不能改善膝关节不稳。人工膝关节置换术费用昂贵,且存在假体松动、术后感染等手术并发症[13]。除手术治疗外,药物疗法及物理疗法虽可以暂缓患者关节的疼痛,但均无法纠正膝关节力线,无法从根本上解决疾病,容易复发。生物力学治疗作为目前正在广泛应用的治疗方法,有着成本低,疗效佳,无创伤等优势。常见的生物力学治疗有矫形器和外侧楔形角矫形鞋垫[14]。
安路德一号免荷矫形器采用“三点力学”免荷方式,在膝关节内侧施加外翻力矩,将患侧软骨承受的压力转移到对侧的软骨上 ( 图 1 )。此外免荷矫形器还可对关节载荷进行重新分配,减小胫骨与股骨间的接触力。佩戴免荷矫形器后内侧骨性关节炎患者将内侧的载荷分配到外侧半月板上,降低内侧半月板的压力[15]。按照上述原理并且结合以往的临床研究,安德路一号免荷矫形器可以通过减小关节载荷达到治疗或者减缓膝关节骨关节炎的功效[16]。然而,这些作用尚未在中国人群得到验证,考虑到亚洲人群和欧美人群在人体解剖数据和骨关节炎的危险因素不尽相同,使用该支具对国人进行详细的临床实验,具有重要意义。
资料与方法
一、纳入与排除标准
1. 纳入标准:( 1 ) 40~70 岁患者;( 2 ) 参考Kellgrene & Lawrence 分型[17]( 图 2 ),使用标准化立位透视,诊断为内侧膝骨关节炎 II 度或 III 度的患者。
2. 排除标准:( 1 ) 其它类型关节炎;双侧骨关节炎,近 3 个月内有关节感染,膝内翻或膝外翻>10°;( 2 ) 运动障碍如帕金森疾病、偏瘫、多发性硬化或运动神经元疾病,周围血管疾病,皮肤疾病;( 3 ) 全膝置换术后或膝单髁关节假体存留;( 4 ) 肢体周长限制的患者:大腿周长<13.5 英寸 ( 35 cm )或>29 英寸 ( 73.5 cm ),小腿周长<10 英寸 ( 25 cm )或>24 英寸 ( 61.5 cm );( 5 ) 非甾体类抗炎药高危人群:对美洛昔康过敏、急性胃溃疡或消化道出血、充血性心力衰竭 ( 美国纽约心脏协会分级 2~4 级 ),确诊冠心病、外周动脉阻塞性疾病或脑血管疾病、肌酐清除率<30 ml / min。

图 1 安陆德免荷一号骨关节炎矫形器“三点力学”原理图,佩戴矫形器后膝关节内侧关节间隙较佩戴之前显著增加Fig.1 The 3-point leverage system of Unloader®One OA knee braces. This system could“unload” the pressure from the affected area
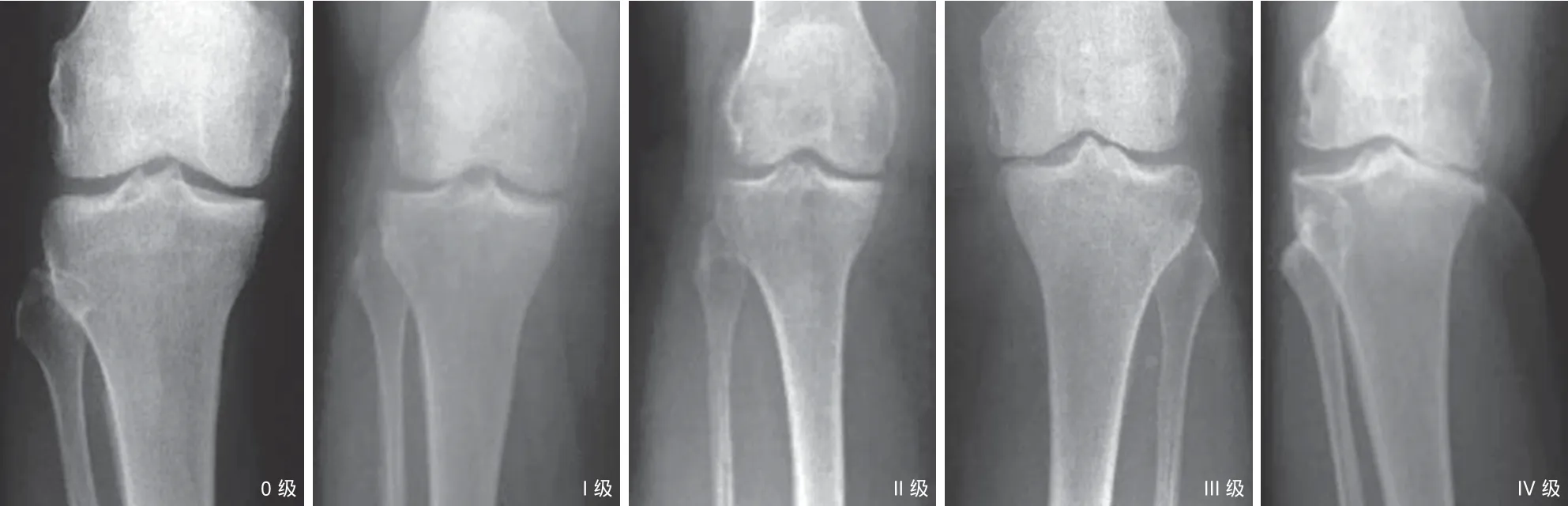
图 2 膝关节骨关节炎严重度 K-L 分级 0~IV 级。0 级:正常;I 级:可疑,不明显的少量骨赘;II 级:轻度,明显的骨赘,关节间隙正常;III 级:中度,关节间隙明显变窄;IV 级:重度,关节间隙严重变窄,软骨下骨硬化 [ 图 1,2 由奥索假肢矫形康复器材 ( 上海 ) 有限公司提供 ]Fig.2 K-L grade of knee OA 0 - IV. K-L grade 0: normal; grade I: doubtful narrowing of joint space and possible osteophytic lipping; grade II: def i nite osteophytes and possible joint space narrowing; grade III: def i nite narrowing of joint space; grade IV: marked narrowing of joint space and severe sclerosis
二、一般资料
本组纳入 2014 年 12 月至 2015 年 12 月至上海市第一人民医院就诊的 36 例骨关节炎患者。患者临床表现为:膝关节疼痛、活动受限、膝关节肿胀。由研究护士通过抽取信封的方式将患者随机纳入到 A,B,C 三组,以确保分组随机双盲。36 例按平均、计算机随机、双盲分为 A、B、C 三组,每组 12 例。A 组:男 4 例,女 8 例,年龄48~68 岁,平均 ( 53.6±7.4 ) 岁,病程 1~8 年,平均 ( 3.3±1.9 ) 年;B 组:男 5 例,女 7 例,年龄52~66 岁,平均 ( 57.4±8.4 ) 岁,病程 1~6 年,平均 ( 4.0±1.7 ) 年;C 组:男 4 例,女 8 例,年龄50~69 岁,平均 ( 55.3±7.8 ) 岁,病程 1~8 年,平均 ( 4.6±1.6 ) 年。三组年龄、性别、临床表现差异无统计学意义。所有患者均签署知情同意书。本课题的数据采集严格按照准入标准,患者全部来自上海市第一人民医院门诊就诊患者,同时由第三方进行质量控制。所采集的数据客观、连续、真实可靠。数据的整理及分析由经过专门培训的研究人员处理。在有限的数据下,能够反映出不同处理方式对患者预后的影响。
三、治疗方案
A 组以安陆德免荷一号矫形器 ( 奥索假肢矫形康复器材 ( 上海 ) 有限公司,国食药监械 ( 进 ) 字2013 第 1260602 号 ) 加美洛昔康 ( 勃林格殷格翰国际贸易 ( 上海 ) 有限公司,国药准字 H20020217 ) 联合治疗,B 组单用安陆德免荷一号矫形器,C 组单用美洛昔康。A、C 组患者,在研究期间需每天按医嘱服用美洛昔康 ( 7.5 mg / 次,每天 1 次 ),持续12 周。A、B 组患者,由奥索公司技术人员教会正确佩戴方法,在研究期间每天佩戴矫形器至少 6 h。患者每隔 3 周来门诊随访,在研究护士的帮助下完成调查问卷,并对矫形器佩戴状况和进行检查。
四、评估指标
治疗前后三组患者 Lysholm 膝关节评分,KOOS评分 ( 包括症状及僵硬、疼痛、日常生活、体育娱乐活动、生活质量 5 项 ),SF-12 生活质量评价量表,过去 24 h VAS 疼痛评分以及 Tegner 活动积分变化。
五、统计学处理
数据用 SPSS 20.0 软件进行统计学分析,计量资料以 x-±s 表示,组内治疗前后比较采用配对 t 检验,组间比较采用单因素 ANOVA 方差分析,P<0.05 差异有统计学意义。使用 graphpad prism 5 作为制图软件。
结 果
在 12 周的研究中,A 组 1 例失联,B 组患者完整地完成了随访,C 组 1 例失联,随访完成度为94.44% ( 34 / 36 )。佩戴支具的患者中,95.65% ( 22 / 23 ) 的患者表示佩戴支具后无不适,并表示愿意继续佩戴。佩戴矫形器后,可见患者内侧膝关节间隙增宽,外侧缩小 ( 图 3 )。服用美洛昔康的患者中,未出现过敏、消化道溃疡、出血等并发症。
将三组患者治疗前后的 Lysholm 膝关节评分表、KOOS 评分表、SF-12 生活质量评价量表、过去24 h VAS 疼痛评分表以及 Tegner 活动积分制成统计表并进行 t 检验结果见表 1~3。较之初始情况,治疗后 12 周三组患者情况改善显著,差异有统计学意义 ( P<0.05 )。
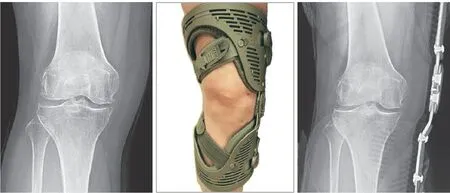
图 3 正位 X 线片上,佩戴矫形器后,该患者内侧膝关节间隙增宽,外侧缩小Fig.3 The AP X-ray of the knee joint showed after wearing Unloader®One OA knee braces, the patient’s medial knee space was widened, the lateral knee space was narrowed
从整体趋势上看,药物治疗起效快,在用药后3 周的数据明显优于治疗前。但在用药 6 周时的数据与 3 周的数据差异无统计学意义,最终效果不如佩戴支具。佩戴支具起效慢,佩戴后 3 周数据与治疗前差异无统计学意义,但最终结果比单独用药好。联合使用药物和支具,从数据上看,可以结合两者的优势,起效快且最终的效果好。
治疗后 3 周,C 组的疗效较 B 组更显著,差异有统计学意义 ( P<0.05 ),C 组与 A 组之间差异无统计学意义 ( P≥0.05 )。治疗后 6 周,A 组疗效明显优于 C 组 ( P<0.05 ),C 组疗效较 3 周前差异无统计学意义 ( P≥0.05 ),但与 B 组相比疗效差异有统计学意义 ( P<0.05 )。第 9 周时,A 组疗效明显优于 C 组,差异有统计学意义 ( P<0.05 );C 组疗效较第 6 周差异无统计学意义 ( P≥0.05 ),且与 B 组疗效差异无统计学意义 ( P≥0.05 )。治疗后 12 周,B 组疗效与A 组差异无统计学意义 ( P≥0.05 ),疗效较 A 组更显著,差异有统计学意义 ( P<0.05 ) ( 图 4~11 )。
表 1 A 组患者治疗前后指标比较 (±s )Tab.1 Comparison of indexes before and after the treatment in group A (±s )
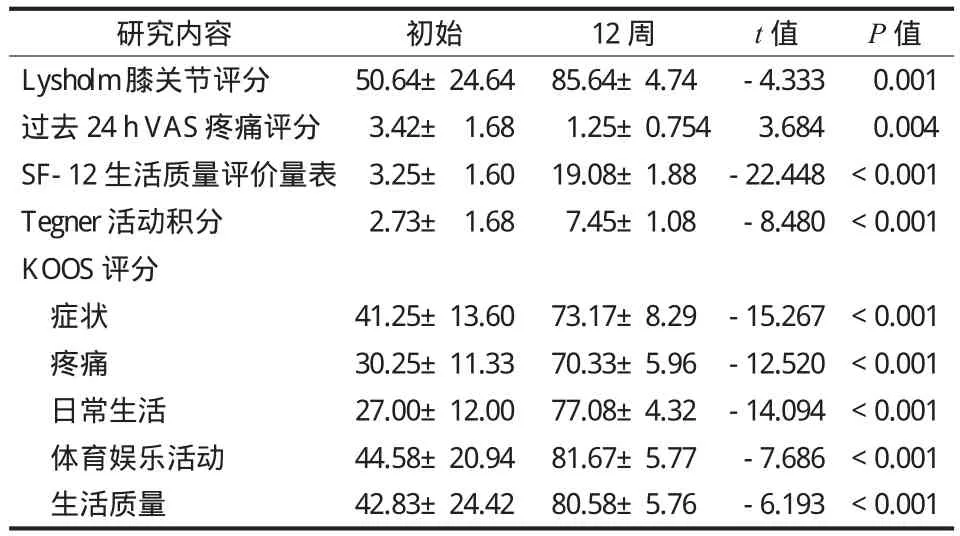
表 1 A 组患者治疗前后指标比较 (±s )Tab.1 Comparison of indexes before and after the treatment in group A (±s )
研究内容 初始 12 周 t 值 P 值Lysholm 膝关节评分 50.64±24.64 85.64±4.74 -4.333 0.001过去 24 h VAS 疼痛评分 3.42± 1.68 1.25±0.754 3.684 0.004 SF-12 生活质量评价量表 3.25± 1.60 19.08±1.88 -22.448 < 0.001 Tegn er 活动积分 2.73± 1.68 7.45±1.08 -8.480 < 0.001 KOOS 评分症状 41.25±13.60 73.17±8.29 -15.267 < 0.001疼痛 30.25±11.33 70.33±5.96 -12.520 < 0.001日常生活 27.00±12.00 77.08±4.32 -14.094 < 0.001体育娱乐活动 44.58±20.94 81.67±5.77 -7.686 < 0.001生活质量 42.83±24.42 80.58±5.76 -6.193 < 0.001
表 2 B 组患者治疗前后指标比较 (±s )Tab.2 Comparison of indexes before and after the treatment in group B (±s )

表 2 B 组患者治疗前后指标比较 (±s )Tab.2 Comparison of indexes before and after the treatment in group B (±s )
研究内容 初始 12 周 t 值 P 值Lysholm 膝关节评分 54.83±18.35 85.33± 4.68 -5.696 < 0.001过去 24 h VAS 疼痛评分 4.09± 1.70 1.40± 0.809 4.628 < 0.001 SF-12 生活质量评价量表 4.92± 1.83 18.83± 2.52 -11.492 < 0.001 Tegner 活动积分 2.18± 1.60 7.55± 1.31 -9.061 < 0.001 KOOS 评分症状 40.67±19.20 71.33±10.63 -4.454 0.001疼痛 29.25±11.39 68.83± 5.01 -10.091 < 0.001日常生活 26.67±12.18 75.92± 5.18 -13.946 < 0.001体育娱乐活动 45.42±21.48 80.00± 7.07 -4.793 0.001生活质量 43.33±20.50 78.17± 6.63 -5.113 < 0.001
表 3 C 组患者治疗前后指标比较 (±s )Tab.3 Comparison of indexes before and after the treatment in group C (±s )
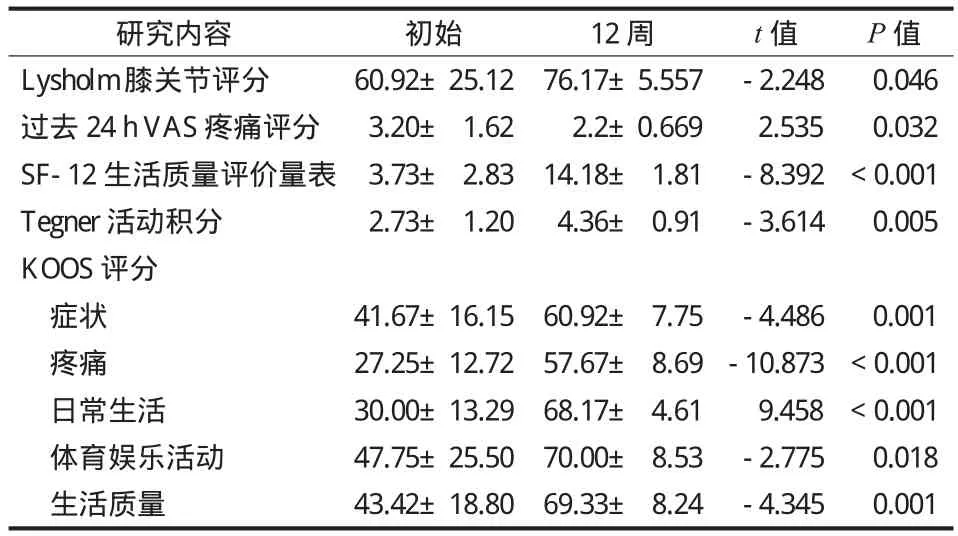
表 3 C 组患者治疗前后指标比较 (±s )Tab.3 Comparison of indexes before and after the treatment in group C (±s )
研究内容 初始 12 周 t 值 P 值Lysholm 膝关节评分 60.92±25.12 76.17±5.557 -2.248 0.046过去 24 h VAS 疼痛评分 3.20± 1.62 2.2±0.669 2.535 0.032 SF-12 生活质量评价量表 3.73± 2.83 14.18± 1.81 -8.392 < 0.001 Tegner 活动积分 2.73± 1.20 4.36± 0.91 -3.614 0.005 KOOS 评分症状 41.67±16.15 60.92± 7.75 -4.486 0.001疼痛 27.25±12.72 57.67± 8.69 -10.873 < 0.001日常生活 30.00±13.29 68.17± 4.61 9.458 < 0.001体育娱乐活动 47.75±25.50 70.00± 8.53 -2.775 0.018生活质量 43.42±18.80 69.33± 8.24 -4.345 0.001
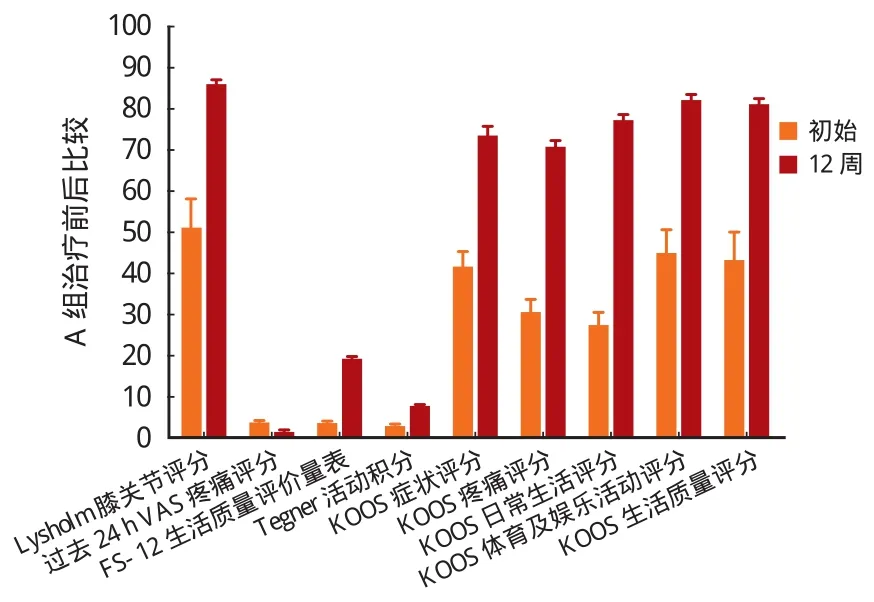
图 4 治疗后 12 周,A 组患者较治疗前情况改善显著 ( P < 0.05 )Fig.4 Twelve weeks later, the symptoms of patients in group A got improved signif i cantly ( P < 0.05 )
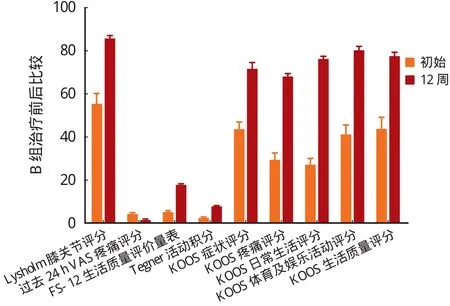
图 5 治疗后 12 周,B 组患者较治疗前情况改善显著 ( P < 0.05 )Fig.5 Twelve weeks later, the symptoms of patients in group B got improved signif i cantly ( P < 0.05 )

图 6 治疗后 12 周,C 组患者较治疗前情况改善显著 ( P < 0.05 )Fig.6 Twelve weeks later, the symptoms of patients in group C got improved signif i cantly ( P < 0.05 )

图 7 三组患者 Lysholm 评分比较 Fig.7 Comparison of Lysholm scores among the 3 groups

图 8 三组患者过去 24 h VAS 疼痛评分比较 Fig.8 Comparison of VAS pain scores in the past 24 hours among the 3 groups
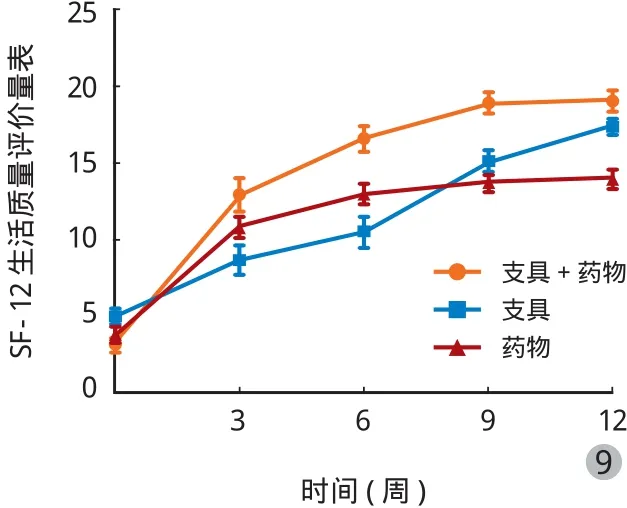
图 9 三组患者 SF-12 生活质量评价量表比较 Fig.9 Comparison of SF-12 scores among the 3 groups

图 10 三组患者 Tegner 活动积分比较Fig.10 Comparison of Tegner active scores among the 3 groups
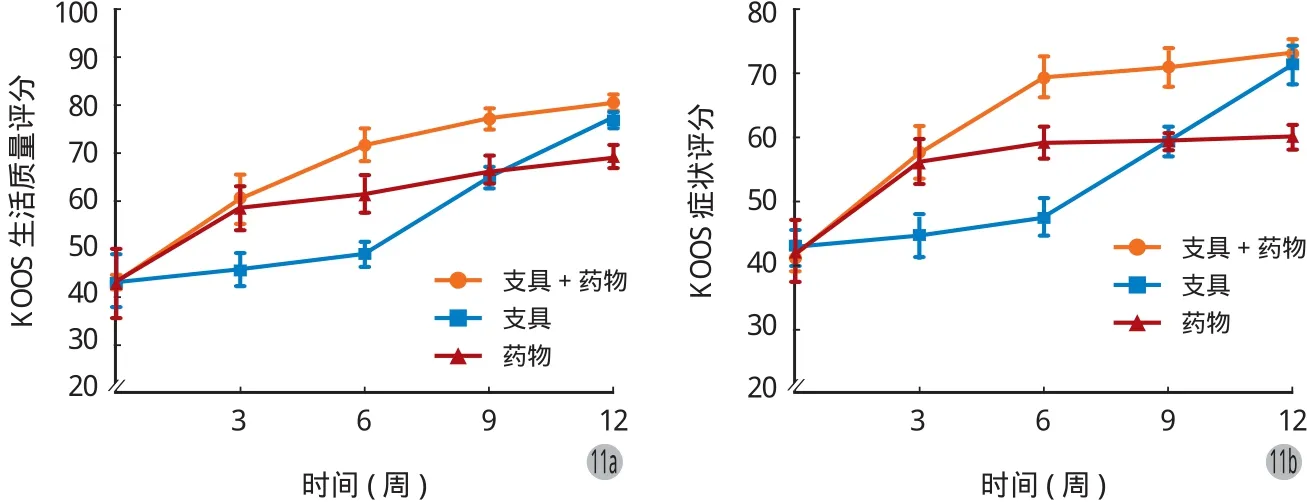

图 11 三组患者 KOOS 评分 ( 包括症状、疼痛、日常生活、体育及娱乐、生活质量 5 项 ) 比较Fig.11 Comparison of KOOS scores ( symptoms, pain, daily life, sports and entertainment, quality of life ) among the 3 groups
讨 论
实验结果表明:单用药物组在短期内可以明显缓解症状,但最终疗效不如矫形器组及药物加矫形器组;单用矫形器组起效时间慢,但最终疗效优于药物组,且与药物、矫形器联用组差异无统计学意义;联用组短期内即可缓解症状,且最终疗效较好。
美洛昔康 ( Meloxicam ) 是烯醇酰胺类非甾体抗炎药 ( NSAIDs ),由德国勃林格殷格翰公司研制,它有抗炎、镇痛作用以及较低胃肠道、肾脏副作用[18],是治疗骨关节炎的常用药物[19]。炎症因子可以导致软骨细胞代谢异常,细胞外基质重塑加快,引起软骨细胞生物力学环境的改变,进而加速 OA 进程[20]。美洛昔康选择性抑制环氧化酶 2 ( Cox-2 ),从而抑制花生四烯酸最终生成前列环素,前列腺素和血栓素 A2,因此直接抑制了炎症因子的合成而起到止痛和抗炎作用[21-22]。本实验中的服用美洛昔康的患者通过抑制炎症因子的合成,早期即可缓解膝关节疼痛症状。但是服用美洛昔康后,患者膝关节仍然处于非正常力线的负重状态,膝关节所承担的压力和关节磨损并未减轻。此外,在服药后关节疼痛减缓的情况下,患者可能增加膝关节活动,因此药物组患者最终疗效不如佩戴矫形器患者。
膝关节是人体最大的承重关节,由于其长期负荷或者承受过大载荷,是骨关节炎的好发部位[23-24]。下肢矫形器按照功能分为稳定型矫形器、功能型矫形器及免荷型矫形器。稳定型矫形器用于固定关节,限制所有的关节活动,长期佩戴会出现关节挛缩、僵硬等并发症。功能型矫形器,又称动力型矫形器,具有弹性,辅助下肢膝关节运动,常用于矫正髌骨力线或维持冠状面上的股骨胫骨稳定性。免荷矫形器不仅能达到固定及运动的效果,且有上述两种矫形器缺乏的免荷的作用。在外观上更加美观简洁,佩戴更加轻便。此外,免荷矫形器着重于动力学特性,在行走时仍能保持其免荷作用。奥索公司的安路德一号免荷矫形器采用“三点力学”免荷方式,对关节负重力线进行重新分配,在膝关节内侧施加外翻力矩,将患侧软骨承受的力转移到对侧的软骨上,降低内侧半月板压力,减小胫骨与股骨间的接触力,从而达到治疗效果[15,25]。软骨细胞有自适应关节载荷的功能,载荷不同软骨的恢复能力不同,适当的关节载荷有益于软骨的成分和生物力学性能的改变[26],因此膝关节免荷矫形器减少了实验组患者膝关节内侧压力,进而达到减缓、治疗的关节炎的效果。并且随着膝关节软骨的自行修复,局部血液循环的建立,可以降低炎症因子的浓度,起到减缓骨关节炎的作用。因此佩戴免荷矫形器的患者治疗后 12 周达到了良好的治疗效果。
联合药物及矫形器治疗的患者,NSAIDs 的抗炎作用短期内可以缓解疼痛,再加上支具对膝关节力线矫正功能,因此对初期疼痛减轻非常明显。从长期治疗角度来讲,佩戴免荷矫形器降低了膝关节内侧的压力,为软骨修复提供了良好的环境,从而达到治疗效果或者缓解疾病进程。
[1] Lawrence RC, Felson DT, Helmick CG, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II[J]. Arthritis Rheum, 2008, 58(1):26-35.
[2] Neogi T, Zhang Y. Epidemiology of osteoarthritis[J]. Rheum Dis Clin of North Am, 2013, 39(1):1-19.
[3] Longo UG, Loppini M, Fumo C, et al. Osteoarthritis: new insights in animal models[J]. Open Orthop J, 2012, 6:558-563.
[4] Kraus VB, Blanco FJ, Englund M, et al. Call for standardized definitions of osteoarthritis and risk stratification for clinical trials and clinical use[J]. Osteoarthritis Cartilage, 2015, 23(8):1233-1241.
[5] Dieppe PA, Lohmander LS. Pathogenesis and management of pain in osteoarthritis[J]. Lancet, 2005, 365(9463):965-973.
[6] Ettinger WH Jr. Osteoarthritis II: pathology and pathogenesis[J]. Md State Med J, 1984, 33(10):811-814.
[7] Koonce RC, Bravman JT. Obesity and osteoarthritis: more than just wear and tear[J]. J Am Acad Orthop Surg, 2013, 21(3): 161-169.
[8] Vaishya R, Pariyo GB, Agarwal AK, et al. Non-operative management of osteoarthritis of the knee joint[J]. J Clin Orthop Trauma, 2016, 7(3):170-176.
[9] Nishida K, Matsumoto T, Takayama K, et al. Remaining mild varus limb alignment leads to better clinical outcome in total knee arthroplasty for varus osteoarthritis[J]. Knee Surg Sports Traumatol Arthrosc, 2016, 9.
[10] Ouyang X, Hong SD, Xin F, et al. The curative efficacy of arthroscopic therapy in treating anterior cruciate ligament rupture with secondary osteoarthritis[J]. Eur Rev Med Pharmacol Sci, 2016, 20(2):214-219.
[11] Herman BV, Giffin JR. High tibial osteotomy in the ACL-def i cient knee with medial compartment osteoarthritis. Journal of orthopaedics and traumatology: off i cial journal of the Italian Society of[J]. J Orthop Traumatol, 2016, 17(3):277-285.
[12] Song SJ, Bae DK, Kim KI, et al. Conversion total knee arthroplasty after failed high tibial osteotomy[J]. Knee Surg Relat Res, 2016, 28(2):89-98.
[13] Huizinga MR, Brouwer RW, Bisschop R, et al. Longterm follow-up of anatomic graduated component total knee arthroplasty: a 15- to 20-year survival analysis[J]. J Arthroplasty, 2012, 27(6):1190-1195.
[14] Phillips S, Silvia Li C, Phillips M, et al. Treatment of osteoarthritis of the knee with bracing: a scoping review[J]. Orthop Rev (Pavia), 2016, 8(2):6256.
[15] Steadman JR, Briggs KK, Pomeroy SM, et al. Current state of unloading braces for knee osteoarthritis[J]. Knee Surg Sports Traumatol Arthrosc, 2016, 24(1):42-50.
[16] Briggs KK, Matheny LM, Steadman JR. Improvement in quality of life with use of an unloader knee brace in active patients with OA: a prospective cohort study[J]. J Knee Surg, 2012, 25(5):417-421.
[17] Kellgren JH, Lawrence JS. Ra diological assessment of osteoarthrosis[J]. Ann Rheum Dis, 1957, 16(4):494-502.
[18] Asghar W, Jamali F. The effect of COX-2-selective meloxicam on the myocardial, vasc ular and renal risks: a systematic review[J]. Inf l ammopharmacology, 2015, 23(1):1-16.
[19] Low-dose meloxicam (Vivlodex) for osteoarthritis pain[J]. Med Lett Drugs Ther, 2016, 58(1490):35-36.
[20] Hoff P, Buttgereit F, Burmester GR, et al. Osteoarthritis synovial fl uid activates pro-inf l ammatory cytokines in primary human chondrocytes[J]. Int Orthop, 2013, 37(1):145-151.
[21] Noble S, Balfour JA. Meloxicam[J]. Drugs, 1996, 51(3): 424-430.
[22] Turck D, Roth W, Busch U. A review of the clin ical pharmacokinetics of meloxicam[J]. Br J Rheumatol, 1996, 35(Suppl 1):13-16.
[23] Murphy L, Schwartz TA, Helmick CG, et al. Lifetime risk of symptomatic knee osteoarthritis[J]. Arthritis Rheum, 2008, 59(9):1207-1213.
[24] Felson DT. Obesity and vocational and avocational overload of the joint as risk factors for osteoarthritis[J]. J Rheumatol Suppl, 2004, 70(2):2-5.
[25] Briggs KK, Matheny LM, Aultman H, et al. 310 use of an unloader brace for medial or lateral compartment osteoar thritis of the knee[J]. Osteoarthritis Cartilage, 2009, 17(Suppl 1): S166-167.
[26] Herzog W, Clark A, Wu J. Resultant and local loading in models of joint disease[J]. Arthritis Rhe um, 2003, 49(2): 239-247.
( 本文编辑:裴艳宏 )
Research on Unloader®One knee brace in the treatment of medial knee osteoarthritis
ZHOU Feng, ZHANG Fei, WANG Hui-xiang, DENG Guo-ying, WU Xiao-ming, WANG Qiu-gen, WANG Qian, WANG Jian-dong. Department of Orthopaedics and Traumatology, Shanghai first People’s Hospital, Shanghai Jiaotong University, Shanghai, 201600, China
WANG Jian-dong, Email: jdwang1973@sina.com
Objective To evaluate the influence of Unloader® One knee brace on the range of motion, pain, function, quality of daily life in the patients with medial knee osteoarthritis ( OA ).MethodsA prospective, randomized and double-blind trial was performed on 36 patients with OA, who were divided into 3 groups, with 12 patients in each group. In group A, the patients were treated with the combination of Unloader®One knee brace and nonsteroidal anti-inf l ammatory drugs ( NSAIDs ) ( meloxicam ). In group B, the patients were treated with Unloader®One knee brace alone. In group C, the patients was treated with NSAIDs ( meloxicam ) alone. All the patients visited the outpatient department every 3 weeks. The therapeutic effects were evaluated by means of the Lysholm knee scoring scale ( LKSS ), knee injury and osteoarthritis outcome score ( KOOS ), SF-12 physical component score, visual analogue scale ( VAS ) and Tegner activity level scale. The overall treatment time was 12 weeks.Results( 1 ) At 12 weeks after the treatment, Lysholm score: 85.64 ± 4.74; KOOS score: 73.17 ± 8.29; pain: 70.33 ± 5.96; daily life: 77.08 ± 4.32; sports and entertainment: 81.67 ± 5.77; quality of life: 80.58 ± 5.76; SF-12 score: 19.08 ± 1.88; VAS pain score in the past 24 hours: 1.25 ± 0.754; Tegner active score: 7.45 ± 1.08 in group A, and all of the indexes got improved significantly ( P < 0.05 ). Lysholm score: 85.33 ± 4.68; KOOS score: 71.33 ± 10.63; pain: 68.83 ± 5.01; daily life: 75.92 ± 5.18; sports and entertainment: 80.00 ± 7.07; quality of life: 78.17 ± 6.63; SF-12 score: 18.83 ± 2.52; VAS pain score in the past 24 hours: 1.4 ± 0.809; Tegner active score: 7.55 ± 1.31 in group B, and all of the indexes got improved signif i cantly ( P < 0.05 ). Lysholm score: 76.17 ± 5.557; KOOS score: 60.92 ± 7.75; pain: 57.67 ± 8.69; daily life: 68.17 ± 4.61; sports and entertainment: 70.00 ± 8.53; quality of life: 69.33 ± 8.24; SF-12 score: 14.18 ± 1.81; VAS pain score in the past 24 hours: 2.2 ± 0.669; Tegner active score: 4.36 ± 0.91 in group C, and all of the indexes got improved signif i cantly ( P < 0.05 ). No signif i cant differences were noticed between group B and group A ( P ≥ 0.05 ), while the therapeutic effects were much better than that in group C ( P < 0.05 ). ( 2 ) From the overall trend, the improvement of symptoms was achieved quickly in group C, but the fi nal effects were worse than those in group A and B. The improvement of symptoms was achieved slowly in group B, but the fi nal effects were better than those in group C. The improvement of symptoms was achieved quickly in group A. There were no signif i cant differences between group A and group B ( P ≥ 0.05 ), while the fi nal effects in group A were much better than those in group C. ( 3 ) Three weeks later, Lysholm score: 71.08 ± 7.63; KOOS score: 56.25 ± 12.22; pain: 41 ± 10.24; daily life: 55.5 ± 10.7; sports and entertainment: 57.08 ± 14.22; quality of life: 55.5 ± 10.7; SF-12 score: 10.92 ± 2.11, VAS pain score in the past 24 hours: 2.08 ± 1.08; Tegner active score: 3.67 ± 1.23 in group C, and the therapeutic effects were much better than those in group B ( P < 0.05 ), while no signif i cant differences existed between group C and group A ( P ≥0.05 ). ( 4 ) Six weeks later, Lysholm score: 81.25 ± 8.95; KOOS score: 69.5 ± 11.33; pain: 62.5 ± 9.8; daily life: 69.5 ± 9.35; sports and entertainment: 72.92 ± 10.97; quality of life: 69.5 ± 9.35; SF-12 score: 16.58 ± 2.84; VAS pain score in the past 24 hours: 1.58 ± 0.79; Tegner active score: 6.58 ± 1.56 in group A, and the therapeutic effects were much better than those in group C ( P < 0.05 ). No signif i cant differences were noticed when compared with group C 3 weeks earlier ( P ≥ 0.05 ), while there were signif i cant differences when compared with group B ( P < 0.05 ). ( 5 ) Nine weeks later, Lysholm score: 85.08 ± 4.91; KOOS score: 71.17 ± 10.53; pain: 65.67 ± 7.33; daily life: 72.42 ± 6.1; sports and entertainment: 77.5 ± 7.54; quality of life: 72.42 ± 6.1; SF-12 score: 18.92 ± 2.07; VAS pain score in the past 24 hours: 1.46 ± 0.54; Tegner active score: 7.42 ± 0.9 in group A, and the therapeutic effects were much better than those in group C ( P < 0.05 ). No signif i cant differences were noticed when compared with those at the 6th weeks in group C ( P ≥ 0.05 ), while there were no significant differences when compared with group B ( P ≥ 0.05 ).Conclusions( 1 ) Better therapeutic effects can be achieved using Unloader®One knee brace in the treatment of medial knee OA. ( 2 ) The symptoms, pain, function and quality of daily life can be effectively improved by using the brace alone even though it takes a longer time relatively. ( 3 ) Pain can be relieved in a shorter time and the fi nal effectsare better by the combination of Unloader®One knee brace and NSAIDs, but no signif i cant differences are found in the fi nal effects when compared with that using the brace alone.
Osteoarthritis, knee; Orthotic devices; Clinical protocols; Cohort studies; Prospective studies
10.3969/j.issn.2095-252X.2017.05.014
R684.3, R687.3
上海市第一人民医院创伤急救中心学科建设经费 ( 院重 1304 );上海市第一人民医院优秀医学青年人才培养前期计划 ( 061417 )
201600 上海市第一人民医院创伤骨科
王建东,Email: jdwang1973@sina.com
2016-09-28 )
