Ajust®与TVT-OTM治疗压力性尿失禁的前瞻性研究
2015-10-12辛星宋悦夏志军
辛星,宋悦,夏志军
Ajust®与TVT-OTM治疗压力性尿失禁的前瞻性研究
辛星,宋悦,夏志军
目的:比较Ajust与TVT-OTM对于治疗女性压力性尿失禁的主观/客观治愈率、术后疼痛感、术后并发症,以及对于生活质量的影响。方法:将2012年1月—2013年5月期间收治的327例压力性尿失禁(SUI)患者随机分为Ajus手术组163例、TVT-OTM手术组164例。采用治愈率、手术并发症、术后疼痛感、患者整体印象改善度(Patient Global Impression of Improvement,PGI-I)、尿失禁问卷表简表(ICIQ-SF)评价疗效。结果:Ajust组患者术后疼痛感较TVT-OTM组显著减轻(P<0.05)。Ajus组手术时间及术中出血量小于TVT-OTM组(P=0.00)。2组围手术期并发症差异无统计学意义(P>0.05)。Ajust组与TVT-OTM组比较,主观治愈率及客观治愈率差异无统计学意义(分别为92.0%比89.6%和95.1%比93.9%,P>0.05)。Ajust组患者术后可以更早恢复正常生活(P=0.00)。2组患者术后生活质量评分较术前均有显著提高(P=0.00),但2组患者生活质量平均改善情况差异无统计学意义(P=0.235)。结论:Ajust治疗SUI操作简便,安全有效。与TVT-OTM相比手术简便快捷,术中出血少,术后疼痛程度轻,恢复时间短。
尿失禁,压力性;疼痛,手术后;手术后并发症;前瞻性研究
(J Int Obstet Gynecol,2015,42:511-514)
压力性尿失禁(SUI)是围绝经期妇女发生尿失禁的最常见类型,其发病率高达50%。保守治疗包括盆底肌肉锻炼(pelvic floor muscle training,PFMT)、生物反馈以及电刺激。伴随着近年来手术方式的不断改进,手术治疗已趋于门诊化手术。降低围手术期发生率、减少住院时间、减少术后疼痛,并使患者更快地恢复正常生活,是目前手术发展的方向。
1 对象与方法
1.1研究对象研究2012年1月—2013年5月于中国医科大学附属盛京医院妇科盆底疾病病房单纯行抗SUI手术的患者共计327例,行完全随机分组,其中163例患者接受Ajust手术治疗,164例接受TVT-OTM治疗,随访12个月,随访期间无患者失访。所有参与者均被告知目前尚缺乏关于Ajust?的长期随访结果。入选标准:尿动力提示SUI,行PFMT失败或拒绝者。排除标准:盆腔器官脱垂定量分度法(pelvic organ prolapse quantitation,POP-Q)≥2,既往行尿控手术、盆腔放疗病史者。
1.2方法
1.2.1疗效评定标准①术前评估,包括详细病史、体质量指数(BMI)、盆底检查和尿动力评估(3 d的排尿日记)。②术后评估,应用视觉模拟量表(visual analog scale,VAS)测量患者术后1 d、1周、2周及1个月的疼痛情况,VAS>5分视为严重疼痛;术后24 h拔出尿管后,嘱患者锻炼自行排尿,并应用膀胱容量测量仪(BladderScan BVI9400)行残余尿量(postvoid residual volume,PVRV)测定,本研究中将术后 24 h PVRV>100 mL视为排尿困难;术后12个月行咳嗽压力实验(standing cough stress test),并填写PGI-I及ICIQ-SF量表,PGI-I量表中患者认为尿失禁症状较术前显著提高或者提高者视为主观治愈。
1.2.2手术方式
1.2.2.1Ajust®手术方式于阴道前壁注射生理盐水,在尿道口下方至尿道下沟之间纵形切开阴道前壁,在阴道尿道间隙层面向两侧分离至闭孔,推动固定锚栓于右侧组织中,直到超过坐骨耻骨支,向闭孔内肌方向转动手柄,推动固定锚栓穿过闭孔内肌及闭孔膜,使吊带中线标记与尿道中段基本对齐,向前推锚栓释放杆,释放固定锚栓,移出导引器,轻拉吊带确定锚栓完全固定,将对侧锚栓装入固定器,左侧同法操作穿入及固定锚栓,调节吊带于适当位置将柔性探针置入带柄,将吊带锁推至可调节锚栓处,移出探针,剪除多余网片,2-0号可吸收线连续锁边缝合阴道前壁切口,查无活动性出血,阴道填塞安尔碘纱布2块,24 h后取出。
1.2.2.2TVT-OTM手术方式于阴道前壁黏膜下注射生理盐水,在尿道口下方至尿道下沟之间纵形切开阴道前壁,在阴道尿道间隙层面向两侧分离至闭孔,在导引器指示下,穿入吊带左翼,出口为平尿道口水平约3 cm,其下方1 cm处。同法穿出吊带右翼。调整吊带松紧度。可吸收线连续缝合阴道前壁。缝合皮肤穿刺点切口,阴道内置安尔碘纱布2块,24 h后取出。
1.3统计学方法采用SPSS19.0软件进行统计学分析。定量资料符合正态分布数据用均数±标准差(x±s)表示,组间比较采用t检验,不符合正态分布数据用中位数(M)和四分位数(P25,P75)表示,组间比较采用秩和检验,定性资料采用卡方检验,P<0.05为差异有统计学意义。
2 结果
2.1术前基本情况2组患者年龄、BMI、每天尿垫数、病程、术前残余尿量、激素替代治疗、既往行全子宫切除术、吸烟等基本情况比较差异均无统计学意义(P>0.05),见表1。
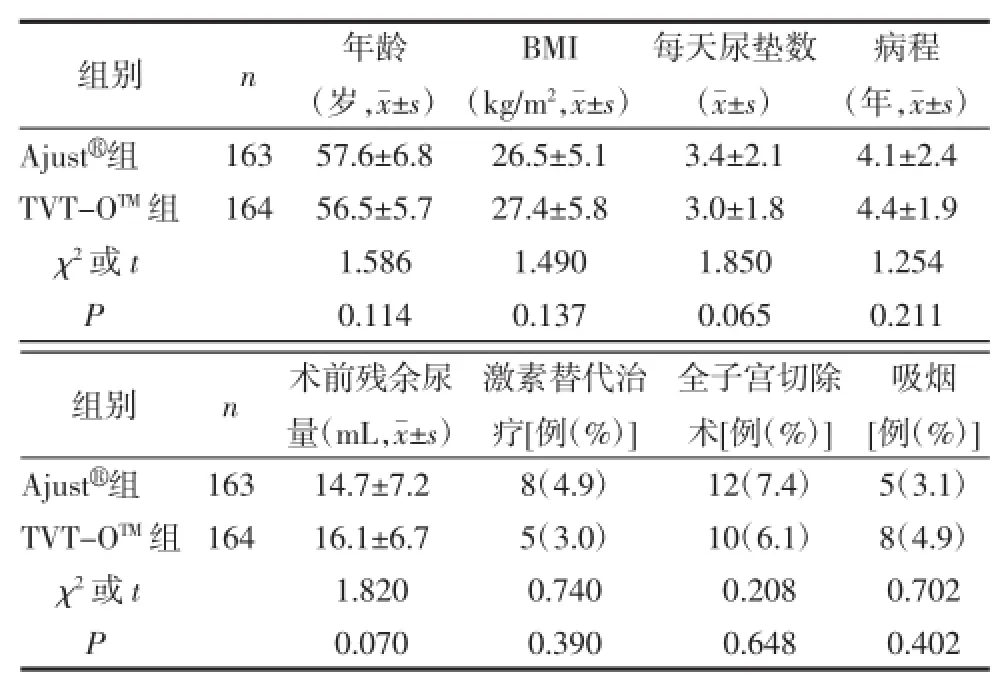
表1 患者术前基本信息

表2 术中情况及围手术期并发症
2.3术后疼痛及随访
2.3.1术后疼痛情况术后1 d、1周、2周、1个月分别测量患者术后疼痛情况,结果显示术后2周内Ajust组疼痛感低于TVT-OTM组,1个月后2组患者疼痛感基本消失,2组间差异无统计学意义,见表3。
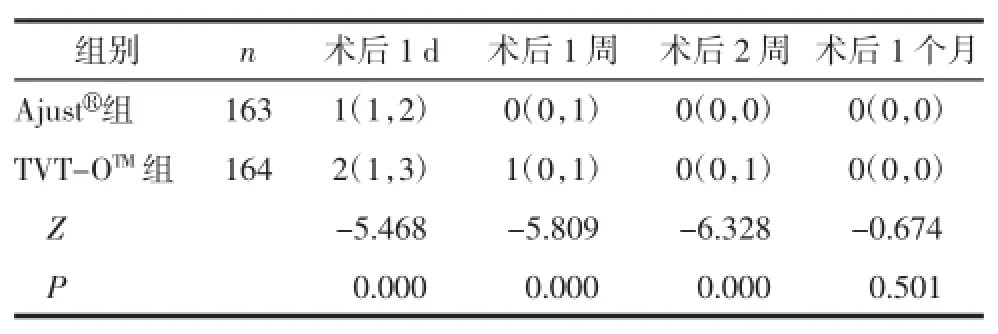
表3 术后VAS疼痛评分(M(P25,P75))
2.3.2术后随访情况及治愈率术后12个月随访,发现Ajust组与TVT-OTM组主观治愈率及客观治愈率差异均无统计学意义。Ajust组患者术后住院时间较TVT-OTM组有缩短趋势,但差异无统计学意义(P>0.05),术后恢复正常生活所需时间显著减少(P<0.05),见表4。
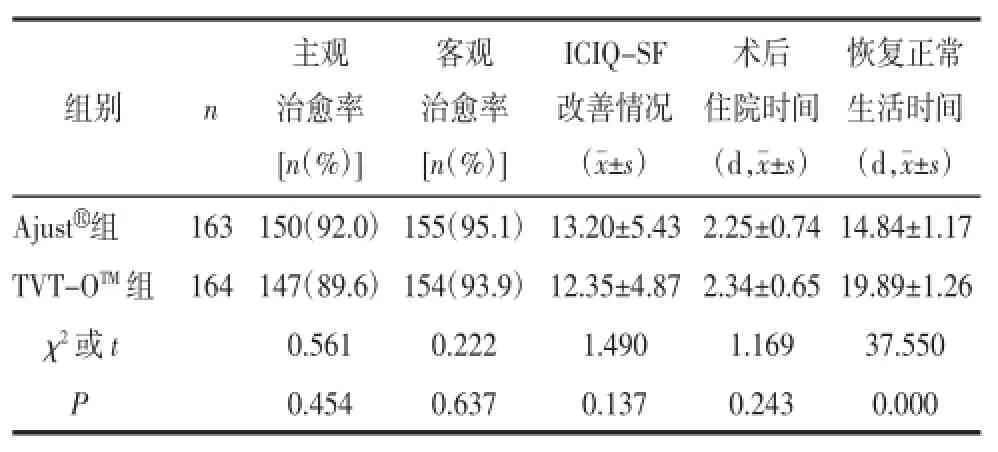
表4 术后随访结果
3 讨论
3.1治疗SUI的相关术式SUI目前多采用手术治疗,并可以取得较好疗效。手术治疗SUI最常用的术式为标准尿道中段悬吊术(standard mid-urethral slings,SMUS),包括经耻骨后无张力尿道悬吊术(retropubic tension-free vaginal tape,RP-TVT)和经闭孔无张力尿道悬吊术(transobturator tension-free vaginal tape,TO-TVT)[1-3]。由于微小切口尿道中段悬吊术(minimally invasive midurethral slings)的引入,改变了手术治疗SUI的方式[4]。可调节单切口吊带(ajust sling)是目前较为先进的治疗SUI的手术方式。吊带为不可吸收的聚丙烯材料,宽约1.2 cm,通过阴道前壁的单一切口置入并悬吊于尿道中段,通过锚定技术将吊带强有力地锚定在闭孔膜上,术中根据患者具体情况调节吊带松紧度以获得合适的张力。此术式优点是损伤小,耐受性好,手术时间短,可以在局部麻醉下完成手术,固定牢固,术后疼痛发生率低,住院时间短,恢复快[5]。
3.2术后主、客观治愈率关于RP-TVT和TOTVT的系统回顾及Meta分析并未证明两者的主、客观治愈率有显著差别[6-7]。但是RP-TVT更容易损伤膀胱,导致术后排尿困难(voiding dysfunction,VD),然而TO-TVT术后腹股沟及大腿疼痛发生率显著提高。
3.3术后疼痛情况国外一项多中心前瞻性研究共入选137例SUI患者,分别随机行Ajus(t69例)或TVT-OT(M68例)手术,术后随访发现术后4周内Ajust组患者的疼痛感显著低于TVT-OTM组[9]。本研究提示与TVT-OTM相比,Ajust手术可显著改善术后2周内的疼痛情况,且患者能更早地活动并恢复正常生活。这些研究结果与之前报道的结果一致[5-6,8,10-11]。TVT-OTM术后疼痛程度重,时间长,面积较大,常伴有下肢疼痛,并且下肢活动后疼痛加重,考虑与内收肌腱受损有关。Ajust术后疼痛程度轻,时间短,术后可更早下床活动,考虑与穿刺局限于闭孔膜,并未穿过闭口外肌、无肌腱损伤有关。
本研究2组术后阴道吊带侵蚀的发生率差异无统计学意义,但显著低于以往报道的早期类型SIMS[13-14]。
3.5术后生活质量以往国外多中心大样本前瞻性研究发现行Ajust术后可明显提高患者生活质量(quality of life,QOL)[4,8-9]。本研究通过ICIQ-SF及PGI-I调查表明2组患者术后生活质量均显著提高。
本研究通过1年的术后随访显示,与传统TVT-OTM相比,Ajust术式具有术后疼痛轻,恢复快,手术简便快捷,术中出血少等诸多优点,但仍需要多中心大样本长期随访进一步证明其疗效。
[1]Ulmsten U,Henriksson L,Johnson P,et al.An ambulatory surgicalproce dure under local anesthesia for treatment of female urinary incontinence[J].Int Urogynecol J Pelvic Floor Dysfunct,1996,7(2):81-85.
[2]Delorme E.Transobturator urethral suspension:mini-invasive procedure in the treatment of stress urinary incontinence in women[J].Prog Urol,2001,11(6):1306-1313.
[3]de Leval J.Novel surgical technique for the treatment of female stress urinary incontinence:transobturator vaginal tape inside-out[J].Eur Urol,2003,44(6):724-730.
[4]Naumann G,Hagemeier T,Zachmann S,et al.Long-term outcomes of the Ajust Adjustable Single-Incision Sling for the treatment of stress urinary incontinence[J].Int Urogynecol J,2013,24(2):231-239.
[5]Abdel-Fattah M,Agur W,Abdel-All M,et al.Prospective multicentre study of adjustable single-incision mini-sling(Ajust)in the management of stress urinary incontinence in women:1-year followup study[J].BJU Int,2012,109(6):880-886.
[6]Novara G,Artibani W,Barber MD,et al.Updated systematic review and metaanalysis of the comparative data on colposuspensions,pubovaginal slings,and midurethral tapes in the surgical treatment of female stress urinary incontinence[J].Eur Urol,2010,58(2):218-238.
[7]Ogah J,Cody DJ,Rogerson L.Minimally invasive synthetic suburethral sling operations for stress urinary incontinence in women:a short version Cochrane review[J].Neurourol Urodyn,2011,30(3):284-291.
[8]Meschia M,Barbacini P,Baccichet R,et al.Short-term outcomes with the AjustTMsystem:a new single incision sling for the treatment of stress urinary incontinence[J].Int Urogynecol J,2011,22(2):177-182.
[9]Mostafa A,Agur W,Abdel-All M,et al.A multicentre prospective randomised study of single-incision mini-sling(Ajust1)versus tension-free vaginal tape-obturator(TVT-OTM)in the management of female stress urinary incontinence:pain profile and short-term outcomes[J].Eur J Obstet Gynecol Reprod Biol,2012,165(1):115-121.
[10]Wang YJ,Li FP,Wang Q,et al.Comparison of three midurethral tension-free tapes(TVT,TVT-O,and TVT-Secur)in the treatment of emale stress urinary incontinence:1-year follow-up[J].Int Urogynecol J,2011,22(11):1369-1374.
[11]Abdel-Fattah M,Ramsay I,Pringle S,et al.Randomised prospective single-blinded study comparing‘inside-out’versus‘outside-in’transobturatortapesinthemanagementofurodynamicstress incontinence:1-year outcomes from the E-TOT study[J].BJOG,2010,117(7):870-878.
[12]Mostafa A,Agur W,Abdel-All M,et al.Multicenter prospective randomized study of single-incision mini-sling vs tension-free vaginal tape-obturator in management of female stress urinary incontinence:a minimum of 1-year follow-up.[J].Urology,2013,82(3):552-559.
[13]Hinoul P,Vervest HA,Den Boon J,et al.A randomized,controlled trialcomparinganinnovativesingleincisionslingwithan established transobturator sling to treat female stress urinary incontinence[J].J Urol,2011,185(4):1356-1362.
[14]Basu M,Duckett J.A randomised trial of a retropubic tension-free vaginal tape versus a mini-sling for stress incontinence[J].BJOG,2010,117(6):730-735.
The Prospective Study of Ajustand TVT-OTMin the Treatment of SUI
XIN Xing,SONG Yue,XIA Zhi-jun.
Pelvic Ward,Shengjing Hospital of China Medical University,Shenyang 110004,China
SONG Yue,E-mail:songy@sj-hospital.org;XIA Zhi-jun,E-mail:xiazj@sj-hospital.org
Objective:To compare the patient-reported and objective cure rates,postoperative pain,postoperative complications,and postoperative quality of life of Adjustable Single-incision Sling(Ajust)versus Tension-free Vaginal Tapeobturator(TVT-OTM)in the treatment of female stress urinary incontinence(SUI).Methods:A randomised trial was conducted in the period between January 2012 and May 2013,with the 327 SUI female patients randomised to either Ajustgroup(163 cases)or TVT-OTMgroup(164 cases).Evaluations were performed to compare the patient-reported and objective cure rates,postoperative complications,postoperative pain profile using Visual Analogue Scale(VAS),Patient Global Impression of Improvement Scale(PGI-I)and International Consultation on Incontinence Questionnaire-Short Form(ICIQ-SF)of these two groups.Results:Compared with the TVT-OTMgroup,patients in the Ajustgroup had a significantly lower postoperative pain(P<0.05),shorter operative duration,and less intraoperative blood loss(P=0.00).No significant difference in peri-operative complications was shown between these two groups.Patient-reported and objective cure rates between the Ajustand TVT-OTMgroups were:92.0%versus 89.6%and 95.1%versus 93.9%respectively,but this did not reach statistical significance(P>0.05).In comparison with the TVT-OTMgroup,the Ajustgroup showed an earlier recovery to normal activities(P=0.00).It is proved in PGI-I that both Ajustand TVT-OTMgroups had a significant improvement of life quality(P=0.00),but no significant difference was shown about the average improvement of life quality between these two groups(P=0.235).Conclusions:Ajustprocedure is simple,safe and effective treatment of SUI.Compared with TVT-OTM,Ajustis simpler and faster,less intraoperative blood loss, generates less postoperative pain and quicker recovery.
Urinary incontinence,stress;Pain,postoperative;Postoperative complications;Prospective studies
2014-12-28)
[本文编辑李淑杰]
110004中国医科大学附属盛京医院妇科盆底疾病病房
宋悦,E-mail:songy@sj-hospital.org
夏志军,E-mail:xiazj@sj-hospital.org
