创伤性肘关节僵硬的围手术期护理及康复治疗
2015-06-24王红莉孔祥燕
王红莉 孔祥燕
·论著·
创伤性肘关节僵硬的围手术期护理及康复治疗
王红莉 孔祥燕
目的 探讨创伤性肘关节僵硬患者围手术期护理及康复治疗要点。方法 2010年1月至2014年12月,北京大学人民医院创伤骨科采用开放式肘关节松解结合铰链式外固定架治疗创伤性肘关节僵硬患者8例。非常严重僵硬(活动范围≤30°)2例,严重僵硬(活动范围30°~60°)6例。Mayo肘关节功能评分45~75分,平均53.8分。其中3例患者术前合并尺神经卡压症状。术前开始给予心理护理;术后给予患肢伤口护理、疼痛护理、外固定架针道护理及针对性功能锻炼治疗。结果 8例患者均得到11~61个月随访,平均随访时间35.4个月。患者肘关节活动度平均105°。Mayo评分70~95分,平均85.0分。3例患者合并尺神经卡压中的2例尺神经损伤症状完全缓解,1例残留部分手内在肌萎缩。所有8例患者均无肘关节不稳定现象,术后未出现其他并发症。结论 采用开放式肘关节松解结合铰链式外固定架治疗创伤性肘关节僵硬,要严格辅助围手术期各项护理及康复治疗,可以有效改善肘关节活动范围,可促进肘关节功能恢复。
创伤;肘关节;僵硬;护理;康复
肘关节是由肱尺、肱桡和上尺桡关节组成的复合关节。创伤后关节囊瘢痕挛缩、关节周围的异位骨化以及长期固定等是造成肘关节僵硬的常见原因[1]。早期肘关节僵硬可以采用保守治疗,而对于保守治疗无效的患者可行开放肘关节松解术。但由于患者术后往往会因为疼痛不能有效配合功能锻炼,即使术中进行了彻底松解,获得了满意的活动范围,也可能出现活动范围的再次丢失。辅助使用铰链式外固定架有助于防止术后关节囊挛缩,帮助患者术后进行早期功能锻炼,能有效预防肘关节僵硬术后复发。2010年1月至2014年3月,北京大学人民医院创伤骨科采用开放性肘关节松解结合铰链式外固定架治疗了创伤性肘关节僵硬8例患者,取得了满意的疗效,现将围手术期护理及康复报道如下。
资 料 与 方 法
一、一般资料
本组8例患者,其中男性3例,女性5例。年龄17~61岁,平均38.3岁。原始损伤肘关节脱位4例,桡骨头骨折1例,肱骨髁上骨折1例,髁间骨折2例。手术距离初次损伤时间10~36个月,平均18.2个月。根据肘关节僵硬的Morrey分型[2]:非常严重僵硬(活动范围≤30°)2例,严重僵硬(活动范围30°~60°)6例。根据Mayo肘关节功能评分[3]:45~75分,平均53.8分。其中3例患者术前合并尺神经卡压症状。
二、手术方法
本组患者均采用全身麻醉。手术经内、外侧联合入路,松解关节囊,肌腱及切除异位骨化。常规松解前置尺神经。透视下定位肘关节的旋转中心,于旋转中心打入2 mm克氏针。使用Stryker DJD II(dynamic joint distractor)外固定架,肱骨和尺骨侧各打入2枚外固定架螺针,螺针需与定位旋转中心的克氏针在同一平面且相互平行。使用夹钳将螺针和外固定架连接固定后,旋转外固定架的牵开螺钉装置牵开肘关节间隙。
三、护理要点
①术前心理护理:评估患者对疾病的认识,根据病情进行健康教育。告知患者手术的目的和效果,术后可能出现的不适及对策,讲解功能锻炼的重要性,制定康复计划。鼓励患者积极配合手术,术后护理及康复训练,以达到满意的治疗效果。②术后患肢护理:卧床期间,患者取平卧位,患肢用软枕抬高,辅以由远端向近端轻柔按摩患肢,以促进静脉回流,减轻肢体肿胀。下地活动时,给予患肢前臂吊带悬吊。评估患肢皮温、血运、感觉和运动状况,判断有无尺神经损伤症状。③术后疼痛护理:采取理疗与药物同时进行的长期镇痛措施。给予患肢手术部位冰袋冷敷,每日3次,每次20 min。同时本组患者术前无胃肠道溃疡病史,术后住院期间给予静脉输注氟比洛芬酯镇痛治疗,每日2次,每次50 mg。对于爆发痛,疼痛评分≥4分的患者,可肌注盐酸哌替啶50 mg。患者出院后口服赛来昔布,每日2次,每次200 mg。④术后针道护理:早期功能锻炼后会出现针道部位的渗出,应及时更换敷料。使用75%乙醇消毒针道周围皮肤,每日2次。告知患者要保持患肢及外固定架的清洁,不能随意触摸针道及外固定架,如果针道部位出现脓性渗出物或针道周围皮肤红肿,则可疑为针道感染,应及时向医生报告,以防外固定架松动。⑤术后功能锻炼:自术后第1天开始,每日移除外固定架的固定杆,帮助患者被动进行肘关节屈曲和伸直位的等长训练,每日3~5组,每组5~10次,鼓励患者进行主动的前臂旋转练习。锻炼前后配合使用止疼药和冷敷,以缓解疼痛。同时加强心理护理,给予患者充分的鼓励与肯定,有利于增强患者康复信心,提高康复效果。此外根据术前肘关节僵硬是屈曲型或伸直型,夜间可将肘关节固定于最大的伸直位或屈曲位[4]。还应重视肩关节、腕关节和手部各关节的主动活动,防止废用性肌萎缩和关节僵硬出现。术后4周,鼓励患者进行肘关节主动屈伸活动。术后6~8周,去除外固定架。
结 果
8例患者随访11~61个月(平均35.4个月)。患者关节活动度平均为105°。Mayo评分70~95分,平均85.0分。3例合并尺神经炎患者中2例症状完全缓解,1例残余部分手内在肌萎缩。8例患者均无肘关节不稳定表现。术后无其他并发症。典型病例,见图1~8。
讨 论
术前向患者交代手术的目的、效果、康复计划,使其了解疾病的治疗、护理及功能锻炼的方案,可以缓解紧张情绪、消除顾虑、树立康复信心。尤其要向患者说明术后早期积极的康复锻炼对日后关节功能恢复非常重要,最终的治疗效果一定程度上取决于患者自身,取决于其参加康复治疗的态度。同时,也要向患者及家属强调肘关节的康复过程的时间较长,往往需要3~6个月,使其做好思想准备。
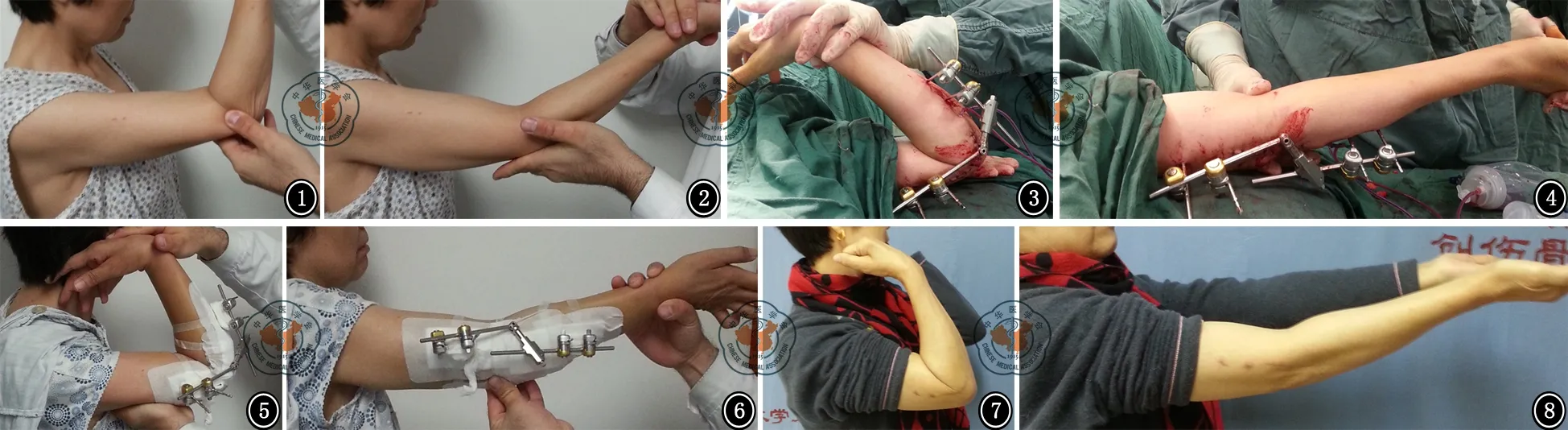
图1 术前屈曲 图2 术前伸直 图3 外架后屈曲 图4 外架后伸直 图5 术后2 d屈曲 图6 术后2 d伸直 图7 术后1年屈曲 图8 术后1年伸直
术后通过患肢抬高和手法按摩,可以促进静脉回流,减轻患肢肿胀,缓解疼痛。特别要评估尺神经的功能,观察是否存在前臂尺侧和环小指麻木或刺痛,并检查手部内在肌的功能。因为肘松解后出现尺神经卡压症状很常见,特别是术前屈肘严重受限,术后改善明显的,多数患者可逐渐缓解[5]。如果术后立即出现尺神经卡压症状,应立即通知医生,必要时手术探查。本组8例患者均在术中进行了尺神经松解前置,有效地预防了术后尺神经并发症的发生。肘关节松解术后患者疼痛一般比较剧烈,功能锻炼也会加重患者的疼痛和不适感,因此需要积极的镇痛治疗。采取冷敷与药物同时长期镇痛的措施,可以降低患者疼痛分值,减少爆发痛的发生频率。
当术后早期进行功能锻炼时,需要将关节间隙牵开,外固定架针道部位皮肤肌肉张力较大,活动后会出现针道部位渗出,应及时更换敷料。同时每日使用75%乙醇消毒针道周围皮肤,可以预防针道感染。通过健康教育,指导患者了解预防针道感染的重要性,提高预防针道感染的意识,学会预防针道感染的方法。
强调早期进行功能锻炼,同时要注意每次活动时应在患者可忍受的范围内达到肘关节最大的屈伸运动范围,争取与手术中所达到的范围基本相同。还要注意的是松解术后,关节周围软组织的延展性和顺应性需要长时间的牵拉和运动才能恢复,因此在夜间休息后经过锻炼获得的肘关节活动度会出现一定程度的丢失,可以在锻炼之间的间歇安装固定杆将肘关节交替固定于最大的屈曲位和伸直位。患者往往会因此出现焦虑和失望,应针对患者的心理状态给予及时的心理护理和专业知识的讲解。
小 结
肘关节是创伤后最易发生僵硬的关节之一,10%~15%的患者肘部创伤后出现肘关节僵硬[6]。肘关节僵硬治疗的目的是恢复肘关节功能,消除活动性疼痛。开放性松解术是治疗肘关节僵硬的常用方法,可明显改善肘关节的活动范围。护理重点是做好患者心理护理、患肢护理和针道护理,重视术后疼痛和外固定架的管理,同时指导并帮助患者做好院内、外的功能锻炼,定期复查。
[1] Myden C,Hildebrand K.Elbow joint contracture after traumatic injury[J].J Shoulder Elbow Surg,2011,20(1):39-44.
[2] Morrey BF.The posttraumatic stiff elbow[J].Clin Orthop Relat Res,2005(431):26-35.
[3] Morrey BF.Post-traumatic contracture of the elbow.Operative treatment,including distraction arthroplasty[J].J Bone Joint Surg Am,1990,72(4):601-618.
[4] Pennig D,Gausepohl T,Mader K.Transarticular fixation with the capacity for motion in fracture dislocations of the elbow[J].Injury,2000,31(Suppl 1):35-44.
[5] 查晔军,公茂琪,蒋协远.创伤后肘关节僵硬[J].中华创伤杂志,2013,29(5):474-478.
[6] Ring D,Hotchkiss RN,Guss D,et al.Hinged elbow external fixation for severe elbow contracture[J].J Bone Joint Surg Am,2005,87(6):1293-1296.
(本文编辑:李静)
王红莉,孔祥燕.创伤性肘关节僵硬的围手术期护理及康复治疗[J/CD].中华肩肘外科电子杂志,2015,3(2):102-105.
Perioperative nursing care and rehabilitation for patients with traumatic elbow joint stiffness
WangHongli,KongXiangyan.
DepartmentofTraumaticOrthopedics,PekingUniversityPeople′sHospital,PekingUniversitytrafficMedicinecenter,Beijing100044,China
KongXiangyan,Email:kxy1766@163.com
Background The elbow joint is a composite joint consisted of the humeroulnar joint,humeroradial joint,and proximal radioulnar joint.The causes for elbow joint stiffness include joint capsule scar contracture,ectopic ossification around the joint and long-term immobilization.The conservative treatment can be applied to early elbow joint stiffness.The open elbow release surgery is applicable for patients who do not respond to conservative therapy.Although satisfactory range of motion is obtained after complete release,the loss of range of motion may occur again if the patients don′t exercise due to pain.The assistance of hinged external fixator helps to prevent joint capsule scar contracture,promote early function exercise,and effectively prevent relapse of elbow joint stiffness.In this study,we reported the perioperative nursing care and rehabilitation in 8 cases who presented good outcomes after open release surgery combined with hinged external fixator for traumatic elbow joint stiffness in the department of traumatic orthopedics in the Peking University-affiliated People′s Hospital from January 2010 to March 2014.Methods General data:8 cases including 3 males and 5 females with a mean age of 38.3 years ranged from 17-61 years were included in the group.4 cases had primary injury caused by dislocation of elbow joint.1 case had radial head fracture.1 had supracondylar fracture of humerus.2 had intercondylar fracture.The time from the initial injury to the surgery ranged from 10-36 months,with a mean of 18.2 months.According to Morrey classification of elbow joint stiffness,2 cases had very severe stiffness (range of motion ≤30°); 6 cases had severe stiffness (range of motion 30°-60°).According to Mayo scale for elbow function,the score ranged from 45-75,with a mean of 53.8.Three cases of them had complicated entrapment of the ulnar nerve.Surgery method:All patients of the group were subject to general anesthesia.The surgery with medial and lateral approaches were performed to release the capsular ligament and tendon,and remove the ectopic ossification.Normal release was performed for the prepositioned ulnar nerve.The center of rotation of the elbow joint was positioned under fluoroscopy.2-mm Kirschner wire was inserted in the center of rotation.Stryker Dynamic Joint Distractor (DJD II) was used for external fixation.2 screws for external fixation were inserted from the humerus and ulna,respectively.The screws should be in parallel with the Kirschner wire in the same plane.The screws were connected with the external fixator using clamp.The elbow joint gap was open by rotating the retractor.Key points for nursing:(1) Psychological nursing before surgery:The patients were subject to health education based on the assessment of patients′ understanding of the condition.Patients were informed of the surgery objective and outcome,possible discomforts after surgery and relative measures and the importance of function exercise.Rehabilitation plan was made for patients.They are also motivated to cooperate during surgery,postoperative nursing care and rehabilitation so that good results could be obtained.(2) Postoperative nursing for affected extremity:During stay in bed,the patients were on the horizontal position with soft pillow elevating the affected extremity.The affected extremity was gently massaged from the distal to the proximal end to promote vein reflux.When the patients are able to get out of the bed,the forearm was supported by strap.The temperature,blood supply,feelings and mobility were assessed to determine whether symptoms of nerve injury developed.(3) Pain management after surgery:Long-term physical therapy and drugs were used to relieve pain.The cold pack was applied to the affected extremity three times per day,20 min once.The patients in the group had no history of gastrointestinal ulcer before surgery.The patients were intravenously administered with flurbiprofen axetil twice at a dose of 50 mg during stay after surgery.In case of flare of pain,people with pain score ≥4 were intramuscularly administered with 50 mg pethidine hydrochloride.After discharge,the patients were orally administered with celecoxib,200 mg once,twice per day.(4) Nursing of approaches after surgery:The dressings were immediately changed if exudate was observed after function exercise at early period.75% alcohol was used to sterilize skin around the approaches,twice per day.The patients were told to keep the affected extremity and external fixator clean.The approaches and external fixator should not be touched at will.If purulent exudate on the approach or red swelling around the approach skin was observed,it was suspected as approach infection.This should be immediately reported to the physician to avoid loosening of external fixator.(5) Function exercise after surgery:1 day after surgery,the fixing pole was removed from the external fixator to help patients to do passive isometric exercise at elbow joint flexion and extension,3 to 5 sets a day,5-10 repeats per set.The patients were motivated to do active forearm rotation exercise.The pain killers and cold packs were combined to ease pain before and after exercise.The psychological nursing was strengthened for patients.Adequate encouragement and positive assessment were provided to patients to increase their confidence in rehabilitation,thereby increasing rehabilitation benefits.Furthermore,based on the types of elbow joint stiffness such as flexion stiffness and extension stiffness,the elbow jont was immobilized at maximum extension or flexion position at night.Adequate attention should be attached to the active motion of the shoulder joint,wrist joint and other joints of the hand.4 weeks after the surgery,patients were motivated to do active elbow joint flexion activities.6-8 weeks after surgery,the external fixator was removed.Results 8 cases were followed up for 11-61 months (with a mean of 35.4 months).The mean range of joint was 105°.The score for Mayo was 70-95,with a mean of 85.0.Two of 3 cases with complicated ulnar neuritis had complete response,and the other one had contraction in the residual intrinsic muscle of hand.Instable characteristics were not observed in all 8 cases.There were no other complications after surgery.Conclusion The elbow joint is one of the joints that are most likely to develop post-traumatic stiffness.10%-15% patients develop joint stiffness after trauma.The aim of treatment for elbow joint stiffness is to recover the function of elbow joint and relive mobility-induced pain.The open release surgery is a common option for elbow joint stiffness.It can obviously imporve the range of motion of the elbow joint.The key for nursing is associated with psychological nursing and nursing of the affected extremity.Another important thing is pain management and nursing for approaches for the external fixator.Also,the patients should have exercise,regular follow-up during stay in the hospital or after discharge,thereby improving the outcome of surgery.
Trauma;Elbow;Stiffness;Nursing;Rehabilitation
10.3877/cma.j.issn.2095-5790.2015.02.007
国家自然科学基金(31371210);教育部创新团队项目(IRT1021);卫生公益性行业科研专项基金(201002014)
100044北京大学人民医院创伤骨科 北京大学交通医学中心
孔祥燕,Email:kxy1766@163.com
2015-04-12)
