Optimal central venous pressure during partial hepatectomy for hepatocellular carcinoma
2013-06-01
Nanning, China
Optimal central venous pressure during partial hepatectomy for hepatocellular carcinoma
Cheng-Xin Lin, Ya Guo, Wan Yee Lau, Guang-Ying Zhang, Yi-Ting Huang, Wen-Zheng He and Eric CH Lai
Nanning, China
BACKGROUND:Low central venous pressure (CVP) affects hemodynamic stability and tissue perfusion. This prospective study aimed to evaluate the optimal CVP during partial hepatectomy for hepatocellular carcinoma (HCC).
METHODS:Ninety-seven patients who underwent partial hepatectomy for HCC had their CVP controlled at a level of 0 to 5 mmHg during hepatic parenchymal transection. The systolic blood pressure (SBP) was maintained, if possible, at 90 mmHg or higher. Hepatitis B surface antigen was positive in 90 patients (92.8%) and cirrhosis in 84 patients (86.6%). Pringle maneuver was used routinely in these patients with clamp/unclamp cycles of 15/5 minutes. The average clamp time was 21.4±8.0 minutes. These patients were divided into 5 groups based on the CVP: group A: 0-1 mmHg; B: 1.1-2 mmHg; C: 2.1-3 mmHg; D: 3.1-4 mmHg and E: 4.1-5 mmHg. The blood loss per transection area during hepatic parenchymal transection and the arterial blood gas before and after liver transection were analyzed.
RESULTS:With active fl uid load, a constant SBP ≥90 mmHg which was considered as optimal was maintained in 18.6% in group A (95% CI: 10.8%-26.3%); 39.2% in group B (95% CI: 29.5%-48.9%); 72.2% in group C (95% CI: 63.2%-81.1%); 89.7% in group D (95% CI: 83.6%-95.7%); and 100% in group E (95% CI: 100%-100%). The blood loss per transection area during hepatic parenchymal transection decreased with a decrease in CVP. Compared to groups D and E, blood loss in groups A, B and C was signi fi cantly less (analysis of variance test,P<0.05). Compared with the baseline, the blood oxygenation decreased signi fi cantly when the CVP was reduced. Base excess and Hin groups A and B were signi fi cantly decreased compared with those in groups C, D and E (P<0.05).
CONCLUSION:In consideration of blood loss, SBP, base excess and, a CVP of 2.1-3 mmHg was optimal in patients undergoing partial hepatectomy for HCC.
(Hepatobiliary Pancreat Dis Int 2013;12:520-524)
central venous pressure; hepatectomy; blood loss
Introduction
Pringle maneuver, when combined with a low central venous pressure (CVP), signif i cantly reduces blood loss during hepatic parenchymal transection.[1-6]The amount of blood loss during hepatectomy is signif i cantly correlated with the inferior vena cava pressure,[7]and the lower the pressure, the less the blood loss. There is a close relationship between the inferior vena cava pressure and CVP.[8]On the other hand, an extremely low CVP affects hemodynamic stability and tissue perfusion. Fawcett et al,[9]on one hand using furosemide, remifentanil and glyceryl trinitrate to reduce the CVP to≤1 mmHg; and on the other hand using phenylephrine to maintain an arterial blood pressure found a decrease in central postoperative venous oxygen saturation and an increase in blood lactate and base excess (BE). What is the optimal CVP which can be maintained during hepatic parenchymal transection to minimize blood loss, and meanwhile to maximize tissue perfusion? This study aimed to fi nd out the optimal CVP during liver transection.
Methods
Subjects
From January to October, 2008, 97 patients with hepatocellular carcinoma (HCC) who underwent elective liver resection at the First Aff i liated Hospital of GuangxiMedical University were prospectively studied. The cohort comprised 87 males and 10 females who were 48.6±8.7 years old. The operation was carried out by a single surgeon (Guo Y). The types of operation included wedge resection, segmentectomy, and hemihepatectomy. Exclusion criteria included hypertension, diabetes mellitus, coagulopathy, portal hypertension, preoperative anemia (Hb <110 g/L), cardiopulmonary dysfunction, liver and kidney dysfunction, reoperation and patients with blood loss of more than 500 mL before liver parenchymal transection. The study protocol was approved by the Ethics Review Committee of the First Aff i liated Hospital of Guangxi Medical University.
Randomization
The patients were randomly allocated into 5 groups by generating a random number from a computer in the operating theater by a nurse who was not involved in this research: group A: numbers 0, 5; group B: 1, 6; group C: 2, 7; group D: 3, 8; and group E: 4, 9.
Anesthesia
Premedication, consisting of diazepam 10 mg and atropine 0.5 mg, was injected intramuscularly 30 minutes before anesthesia. On arrival to the operating room, an intravenous line was set up in the left median cubital vein of the patient for fl uid and drug administration. A HP M1205A monitor (HP, USA) was used to continuously monitor the electrocardiogram, peripheral oxygen saturation (SpO2), direct arterial pressure (left radial artery), and CVP (right internal jugular vein cannulation) of the patient. Urine output was measured through a urinary catheter. CVP was set at zero by a pressure transducer at the left midaxillary line at the level of the right atrium. General anesthesia was induced with midazolam 0.04 mg/kg, fentanyl 4 μg/kg, etomidate 0.3 mg/kg, and lidocaine 1.5 mg/kg followed by vecuronium 0.1 mg/kg for muscle relaxation. Anesthesia was maintained with infusion of propofol (4 mg/kg per hour), inhalation of 1% isof l urane, and bolus doses of fentanyl 0.1 mg and vecuronium 4 mg to provide adequate analgesia and muscle relaxation. After endotracheal intubation, respiration was controlled by mechanical ventilation at 50% oxygen concentration, at a frequency of 10-13 L/min and a tidal volume of 10 mL/kg. All patients were mechanically ventilated to maintain an end-tidal carbon dioxide concentration in the range of 30 to 35 mmHg.
Acquisition and maintenance of low CVP
All patients received lactated Ringer's solution before induction of anesthesia and during the operation at a rate of 1 mL/kg per hour. The CVP levels of the patients ranged from 6 to 10 mmHg at the start of the operation. The CVP was initially lowered by using intravenous furosemide 5-10 mg and intravenous infusion of nitroglycerin at an initial dose of 0.5 μg/kg per minute. The dose of nitroglycerin was gradually increased at a rate of 0.1 μg/kg per minute to per 5 minutes until the CVP dropped to a desirable level. If the CVP could be maintained at the desired level, parenchymal transection was started using a cavitational ultrasonic surgical aspirator (CUSA, Valleylab, Boulder CO., USA). As far as possible, the SBP was maintained at ≥90 mmHg by infusing boluses of lactated Ringer's solution. After completion of liver parenchymal transection, intravenous nitroglycerin was stopped and the CVP was brought up to 5-9 mmHg with crystalloid, 6% hydroxyethyl starch or plasma. Packed red cells were transfused when the blood loss was more than 1 liter or the Hb fell to below 80 g/L. Each patient gave informed consent to participate in the study.
Data collection
The patients were divided into 5 groups as previously described. The amount of fl uid transfusion and the blood loss during liver parenchymal transection were recorded. The CVP, SBP, diastolic blood pressure (DBP), mean arterial pressure (MAP), and heart rate (HR) were recorded before induction of anesthesia, during liver parenchymal transection and at the end of the operation. The arterial blood gas was analyzed before and at the end of the operation. The transfusion volume and blood loss per transection area (blood loss during transection/cross sectional area of the liver) were recorded and calculated. Blood loss was estimated by measuring blood in the suction bottle and by weighing all the blood-stained gauzes. An AutoCAD software was used to measure the cross sectional area of the liver parenchymal transection.
Statistical analysis
The data were expressed as mean±SD. SPSS software package version 13.0 was used for statistical analysis. Analysis of variance, S-N-K for multiple comparisons of the means of the groups, pairedttest and the Chisquare test were used. Statistical signif i cance was def i ned asP<0.05.
Results
The demographic data are shown in Table 1. There was no signif i cant difference between the 5 groups in age, body weight, gender, percentage of patients with livercirrhosis, types of liver resection, operative time, portal triad clamping time, and duration of liver parenchymal transection.
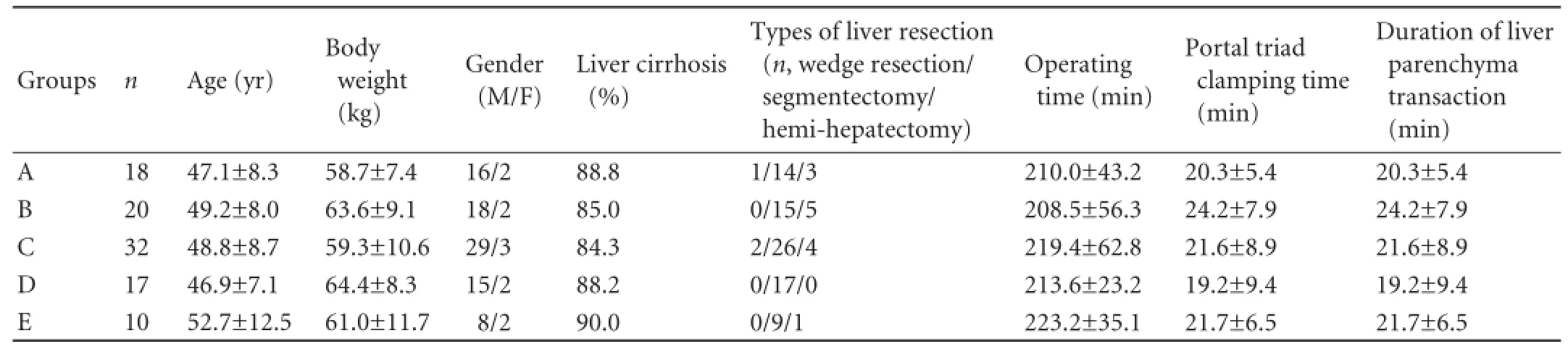
Table 1.Demographic data
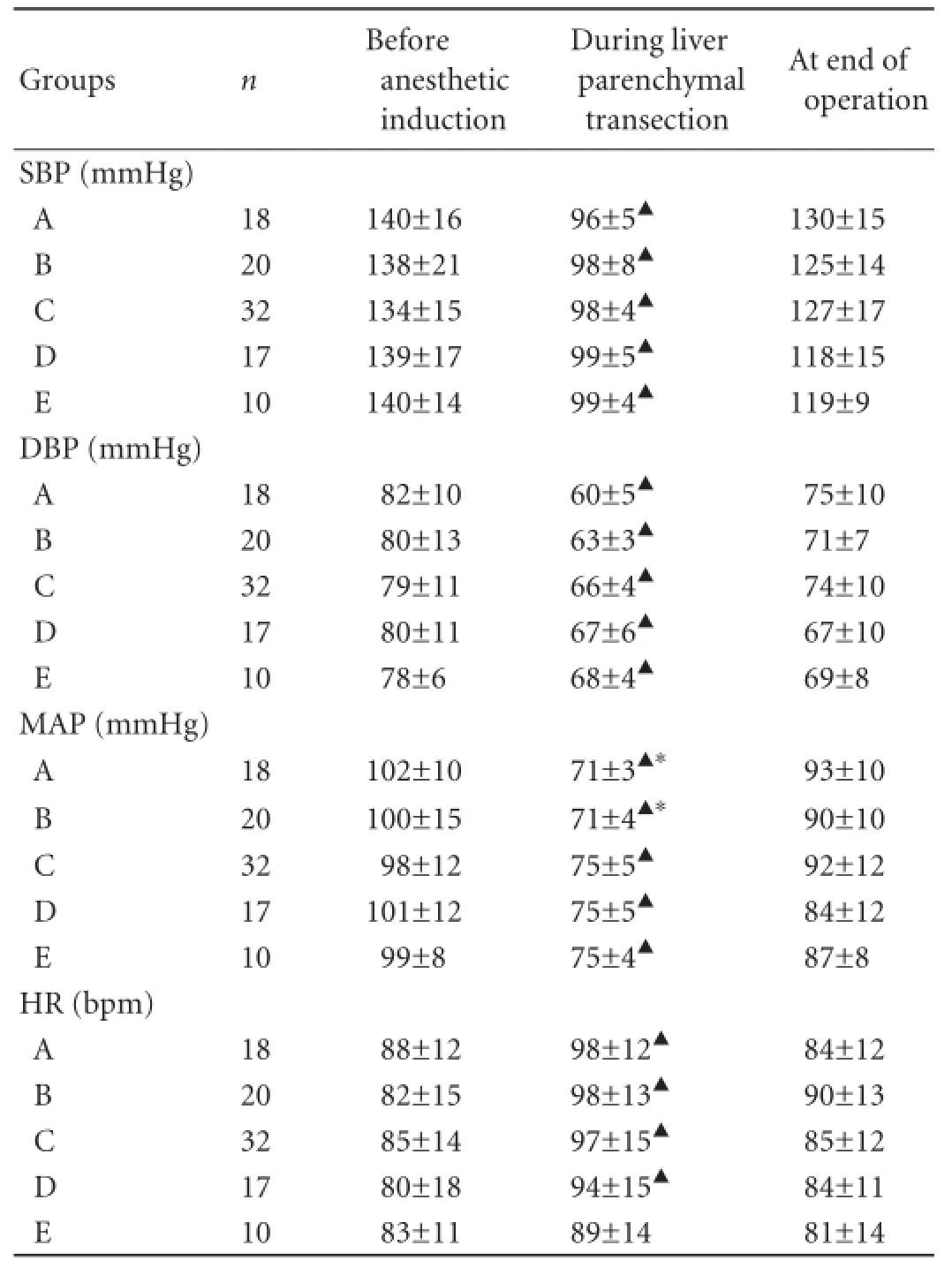
Table 2.The SBP, DBP, MAP, HR changes at different levels of CVP
With active fl uid load, a SBP >90 mmHg which was considered as optimal was maintained as far as possible. This optimal blood pressure was maintained in 18.6% in group A (95% CI: 10.8%-26.3%); 39.2% in group B (95% CI: 29.5%-48.9%); 72.2% in group C (95% CI: 63.2%-81.1%); 89.7% in group D (95% CI: 83.6%-95.7%);and 100% in group E (95% CI: 100%-100%).

Table 3.Blood loss per transection area during hepatic parenchymal transection
There was no signif i cant difference in the hemodynamics parameters of SBP, DBP, MAP, and HR at the time before induction of anesthesia and at the end of operation in the fi ve groups of patients. Compared with the parameters before induction of anesthesia, the SBP, DBP, and MAP were signif i cantly decreased during liver transection in all the groups (analysis of variance test,P<0.05) and the HR was signif i cantly faster except in group E (analysis of variance test,P<0.05). Compared with groups C, D and E, the SBP, DBP and MAP were signif i cantly decreased in groups A and B during liver transection (analysis of variance test,P<0.05) (Table 2). As hepatic parenchymal transection was carried out during clamping of the porta hepatis, the duration of hepatic parenchyma transection was the same as theclamping time of the portal triad (Table 2). As hepatic parenchymal transection was carried out during clamping of the porta hepatis, the duration of hepatic parenchyma transection was the same as the clamping time of the portal triad (Table 2).

Table 4.Intravenous infusion volumes at different periods
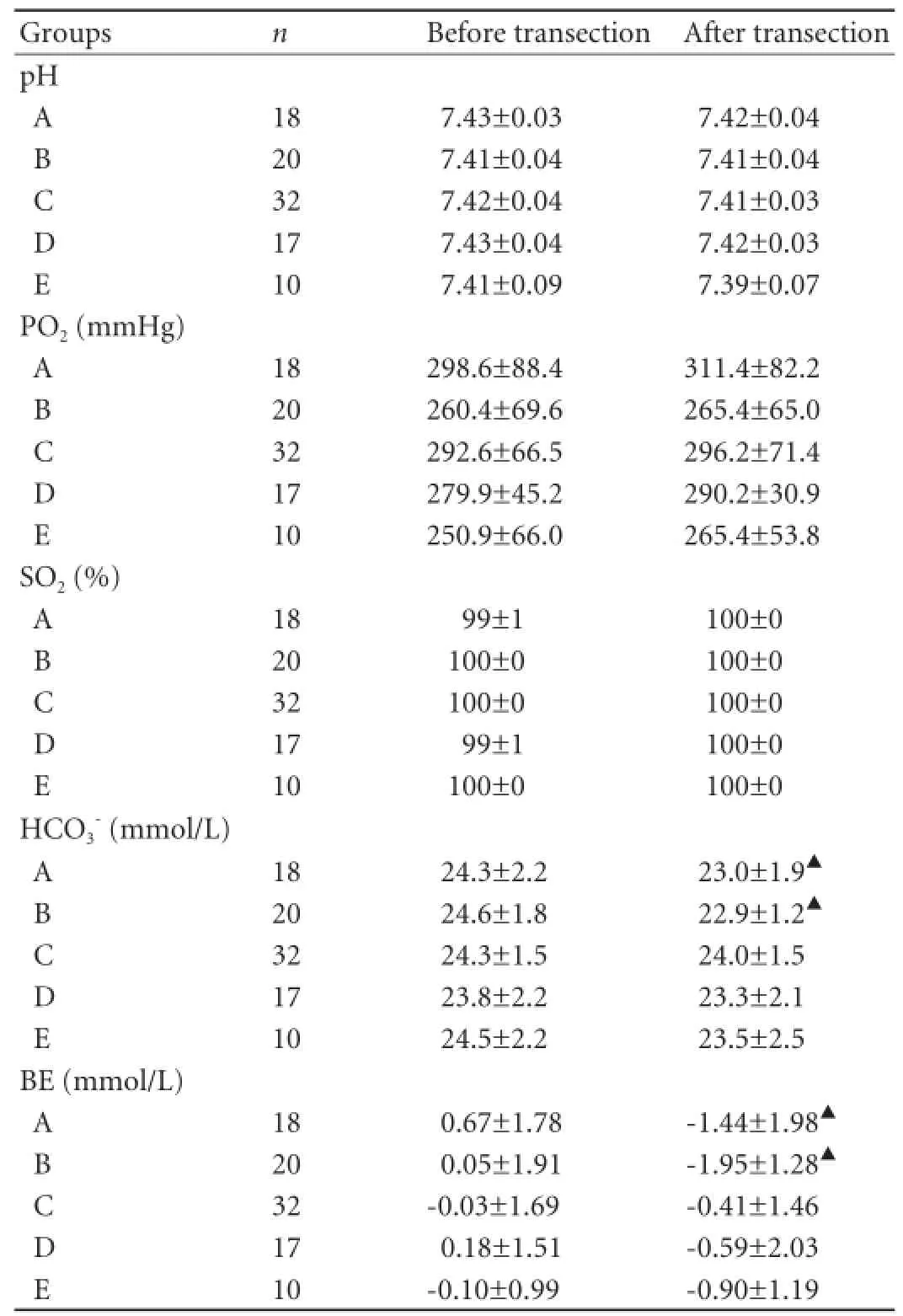
Table 5.Arterial blood gas analysis before and after liver transection
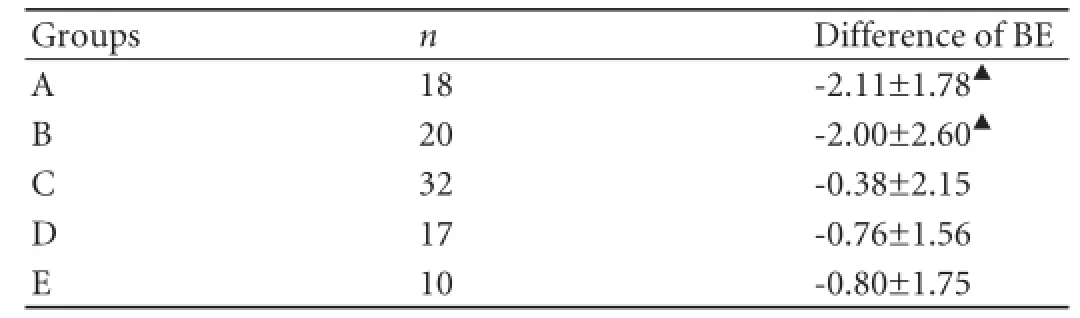
Table 6.Difference of base excess (BE) before and after liver transection
Compared with the baseline, arterial blood oxygenation signif i cantly decreased with a decrease of CVP (Table 5). BE andin groups A and B were signif i cantly lower than those in groups C, D and E (pairedttest,P<0.05) (Table 6).
Discussion
A low CVP can be achieved by limiting the infusion volume, using diuretic and/or vasoactive drugs. The mean arterial pressure (MAP)=cardiac output (CO) × systemic vascular resistance (SVR), and the cardiac output=stroke volume×heart rate. As the stroke volume is related to the preload (Starling's Law), a low CVP affects cardiac output, resulting in systemic hypotension. In most individuals, blood pressure can be maintained by a faster HR or by peripheral vascular constriction. In patients with cardiovascular diseases, a decrease in CVP leads to a decrease in blood pressure, especially when the patient has blood loss. This study showed that most patients could maintain their SBP at an optimal level (≥90 mmHg) when hepatic parenchymal transection was carried out at a CVP of 3-5 mmHg.
Most surgeons now carry out hepatic parenchymal transection at a CVP below 5 mmHg[5,9-11]or 5 cmH2O (1 cmH2O=0.74 mmHg).[12-14]Reduction of the CVP decreases the pressure in the hepatic sinusoids, thus mitigating blood loss during liver transection. In this study, blood loss during liver transection in patients with a CVP of 0-3 mmHg was signif i cantly less than that in those with a CVP of 4-5 mmHg. A further drop in CVP (<2 mmHg) did not result in a signif i cant decrease in blood loss. This is probably because of the vigorous attempts to maintain the SBP to ≥90 mmHg. As the blood volume increased, the diameter of the hepatic vein was enlarged. According to the formula Q=Δpr4, both the difference in the exterior and interior pressureof the vessel wall and the radius of the hepatic vein affect blood loss per transection area during hepatic parenchymal transection. By half blocking the inferior vena cava, Uchiyama et al[15]signif i cantly decreased CVP and the diameter of the right hepatic vein and thus, they reduced the blood loss in their hepatectomy. Fawcett et al,[9]by using auxiliary phenylephrine to maintain the arterial blood pressure at a CVP ≤1 mmHg, found that central venous oxygen saturation decreased signif i cantly, while blood lactate and BE increased signif i cantly after operation. These observations were supported by our previous study on pigs.[16]The current study on patients showed that when compared with the baseline, pH, SO2and PO2were not signif i cantly changed after surgery in all of the patients. However, BE andvalues were signif i cantly decreased in patients whose CVP was lower than 2 mmHg. This might be due to the low MAP which caused poor tissue perfusion in these patients. This study also showed that patients with a CVP of 3-5 mmHg, the oxygenation status and acid-base balance were normal. The CVP could not be lowered to the target level in some patients and these patients were excluded.
In conclusion, an optimal SBP of ≥90 mmHg could be maintained with a CVP of >3 mmHg during hepatic parenchymal transection in most patients. Maintaining the CVP at 2.1-3 mmHg signif i cantly reduces blood loss, and the adverse effects on tissue perfusion are signif i cantly lower than those of a CVP of <2 mmHg. A CVP of 2.1-3 mmHg, therefore, is proposed to be optimal during liver transection.
Contributors:GY and LWY proposed the study. GY wrote the fi rst draft. LCX, GY, ZGY, HYT, HWZ and LECH analyzed the data. All authors contributed to the design and interpretation of the study and to further drafts. GY is the guarantor.
Funding:This research was supported by a grant from the Guangxi Natural Science (GKZ0447066).
Ethical approval:The study protocol was approved by the Ethics Review Committee of the First Aff i liated Hospital of Guangxi Medical University.
Competing interest:No benef i ts in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
采用EpiData 3.1进行数据录入,SPSS 20.0软件进行统计分析。使用构成比、均数、标准差等进行统计描述。疫苗及安全接种知信行得分不服从正态分布,组间比较采用Mann-Whitney U检验和Kruskal-Wallis H检验;采用Logistic逐步回归法(剔选界值α入=0.05,α出=0.10)分析疫苗及安全接种知识、态度、行为得分分组的影响因素;KAP相关性分析采用Spearman秩相关。
1 Cunningham JD, Fong Y, Shriver C, Melendez J, Marx WL, Blumgart LH. One hundred consecutive hepatic resections. Blood loss, transfusion, and operative technique. Arch Surg 1994;129:1050-1056.
2 Child TJ, MacKenzie IZ, Rees M. Terminations of pregnancy, not unplanned deliveries, increased as result of pill scare. BMJ 1996;313:1005.
3 McCall J, Koea J, Gunn K, Rodgers M, Jarvis J. Liver resections in Auckland 1998-2001: mortality, morbidity and blood product use. N Z Med J 2001;114:516-519.
4 Jarnagin WR, Gonen M, Fong Y, DeMatteo RP, Ben-Porat L, Little S, et al. Improvement in perioperative outcome after hepatic resection: analysis of 1,803 consecutive cases over the past decade. Ann Surg 2002;236:397-407.
5 Hamady ZZ, Kotru A, Nishio H, Lodge JP. Current techniques and results of liver resection for colorectal liver metastases. Br Med Bull 2004;70:87-104.
6 Smyrniotis V, Kostopanagiotou G, Theodoraki K, Tsantoulas D, Contis JC. The role of central venous pressure and type of vascular control in blood loss during major liver resections. Am J Surg 2004;187:398-402.
7 Johnson M, Mannar R, Wu AV. Correlation between blood loss and inferior vena caval pressure during liver resection. Br J Surg 1998;85:188-190.
8 Yung M, Butt W. Inferior vena cava pressure as an estimate of central venous pressure. J Paediatr Child Health 1995;31:399-402.
9 Fawcett WJ, Quiney NF, Karanjia ND. Central venous oxygen saturation, base excess and lactate changes during induced hypovolaemic liver resection. Anesthesia 2007;62:312-313.
10 Furrer K, Deoliveira ML, Graf R, Clavien PA. Improving outcome in patients undergoing liver surgery. Liver Int 2007; 27:26-39.
11 Chen H, Merchant NB, Didolkar MS. Hepatic resection using intermittent vascular inf l ow occlusion and low central venous pressure anesthesia improves morbidity and mortality. J Gastrointest Surg 2000;4:162-167.
12 Stanziale SF, Fong Y. Current surgical therapy of hepatic colorectal metastasis. Eur Surg 2002;34:18-24.
13 Lin CC, Chen CL, Cheng YF, Chiu KW, Jawan B, Hsaio CC. Major hepatectomy in children: approaching blood transfusion-free. World J Surg 2006;30:1115-1119.
14 Imamura H, Seyama Y, Kokudo N, Maema A, Sugawara Y, Sano K, et al. One thousand fi fty-six hepatectomies without mortality in 8 years. Arch Surg 2003;138:1198-1206.
15 Uchiyama K, Ueno M, Ozawa S, Hayami S, Kawai M, Tani M, et al. Half clamping of the infrahepatic inferior vena cava reduces bleeding during a hepatectomy by decreasing the central venous pressure. Langenbecks Arch Surg 2009;394: 243-247.
16 Guo Y, Lin CX, Lau WY, Long D, Lao CY, Wen Z, et al. Hemodynamics and oxygen transport dynamics during hepatic resection at different central venous pressures in a pig model. Hepatobiliary Pancreat Dis Int 2011;10:516-520.
Received March 15, 2012
Accepted after revision March 5, 2013
AuthorAff i liations:Department of Anesthesiology (Lin CX, Zhang GY, Huang YT and He WZ) and Department of Hepatic and Biliary Surgery (Guo Y and Lau WY), First Aff i liated Hospital of Guangxi Medical University, Nanning 530021, China; Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong, China (Lau WY and Lai ECH)
Ya Guo, MD, Department of Hepatic and Biliary Surgery, First Aff i liated Hospital of Guangxi Medical University, Nanning 530021, China (Tel: 86-771-5356528; Fax: 86-771-5350031; Email: guoya2000 @medmail.com.cn)
© 2013, Hepatobiliary Pancreat Dis Int. All rights reserved.
10.1016/S1499-3872(13)60082-X
猜你喜欢
杂志排行
Hepatobiliary & Pancreatic Diseases International的其它文章
- Simultaneous recovery of dual pathways for ammonia metabolism do not improve further detoxif i cation of ammonia in HepG2 cells
- Risk factors and clinical characteristics of portal vein thrombosis after splenectomy in patients with liver cirrhosis
- Fine needle aspirating and cutting is superior to Tru-cut core needle in liver biopsy
- Diagnostic accuracy of enhanced liver fi brosis test to assess liver fi brosis in patients with chronic hepatitis C
- Mattress sutures for the modif i cation of end-toend dunking pancreaticojejunostomy
- Retrohepatic vena cava deroof i ng in living donor liver transplantation for caudate hepatocellular carcinoma