Relationship between alcohol consumption and clinical manifestation of patients with fatty liver:a single-center study
2011-06-11
Hangzhou,China
Introduction
Fatty liver is a common chronic liver disease worldwide.The morbidity of fatty liver has been increasing in recent years to 30% in Western countries and 20% in China.[1-4]It represents a spectrum of hepatic disorders ranging from simple steatosis to steatohepatitis,fibrosis and cirrhosis.[5]Generally,simple hepatic steatosis is a benign disease which does not progress to steatohepatitis,whereas steatohepatitis could develop progressively to liverfibrosis and liver cirrhosis.[6]The development and progression of fatty liver is closely associated with obesity,and it also attributes to excessive alcohol intake.[7,8]Long-term heavy consumption of alcohol has been found to be a high risk factor of fatty liver,but light to moderate consumption is associated with reduced risk of fatty liver,suggesting a dosedependent relationship between alcohol consumption and hepatic steatosis.Until now,the effect of alcohol consumption on clinical manifestation of fatty liver in the Chinese population remains unclear.Therefore,we investigated 669 patients with fatty liver,and analyzed the relationship between alcohol consumption and clinical manifestations of fatty liver in the Chinese population.
Methods
Subjects
The subjects of the study were employees from other companies taking annual health examination at our hospital between September 1,2009 and January 1,2010.They met the following criteria:(1) typical fatty liver manifestations shown by ultrasonography; and (2) no hepatotrophic virus infection nor history of other causes of chronic liver disease.In the 669 subjects enrolledfinally in the study,166 had a history of long-term alcohol consumption (alcohol consumption of more than 60 g per week for at least 2 years),and 503 had no history of long-term alcohol consumption.In the 669 subjects,539 were male and 130 female.Their mean age was 46.76 years (range from 30 to 70 years).The subjects without a history of long-term alcohol consumption were further divided into light drinking group (alcohol consumption less than 60 g per week,n=285),and non-drinking group(without any alcohol conusmption,n=218).
Clinical examination
Clinical examination was performed in the morning after overnight fasting as described previously.[9]Brie fly,the subjects were instructed to refrain from exercise during the day before examination.The examination included physical examination,blood taking,blood pressure measurement,anthropometry,and health habit inventory.Standing height and body weight without shoes and outer clothing were measured.Body mass index (BMI) as an index of body fat was calculated as weight in kg divided by height in meters squared.
Laboratory evaluation
Fasting blood samples taken from an antecubital vein were used for the analysis of routine blood counts and biochemical values.Routine blood counts were measured by Sysmex XE-2100 and a Beckman coulter LH780 autoanalyzer.The values of alanine transaminase (ALT),aspartate transaminase (AST),γ-glutamyl transpeptidase(GGT),triglyceride (TG),total cholesterol (TC),highdensity lipoprotein cholesterol (HDL-C) and fasting plasma glucose (FPG) were determined by a Hitachi 7600 auto-analyzer using standard methods.
Ultrasonography
Ultrasonography of the liver was conducted for all subjects by a trained ultrasonographist who was unaware of the clinical and laboratory data,using a Toshiba Nemio 20 sonography machine (Toshiba,Tokyo,Japan) with a 3.5-MHz Probe.Manifestations of hepatic steatosis included diffused enhancement of nearfield echo in the hepatic region relative to the kidney and spleen,gradual attenuation of the farfield echo,mild to moderate hepatomegaly,and unclear display of intrahepatic structures.
Statistical analysis
Statistical analyses were preformed with the software SPSS 13.0 (SPSS Inc.,Chicago,IL).Continuous variables were presented as the mean and standard deviation.The differential expression of continuous data between the two groups was determined by Student's t test.A P value less than 0.05 (two-tailed test) was considered statistically significant.
Results
There was no significant difference in age between the two groups,but males were more likely to be long-term alcohol consumers.The percentage of steatotic hepatitis defined in subjects with abnormal levels of serum ALT and/or AST was not significantly different between the two groups.
The clinical and laboratory data of the subjects in the two groups showed that the values of BMI,diastolic pressure,AST,GGT,TG,TC,FPG and hemoglobin in the long-term alcohol consumption group were significantly higher than those in the non long-term alcohol consumption group (P<0.05) (Table 1).
To understand the relationship between alcohol consumption and hepatic steatosis,the subjects in the non long-term alcohol consumption group were allocated to either light consumption group (drinking alcohol less than 60 g per week) or non consumption group.The clinical and laboratory data of the subjects were compared between the two groups,and the valuesof GGT and hemoglobin in the light consumption group were significantly higher than those in the non consumption group (P<0.05).In BMI,diastolic pressure,AST,TG,TC and FPG,no significant difference was observed between the two groups (P>0.05)(Table 2).
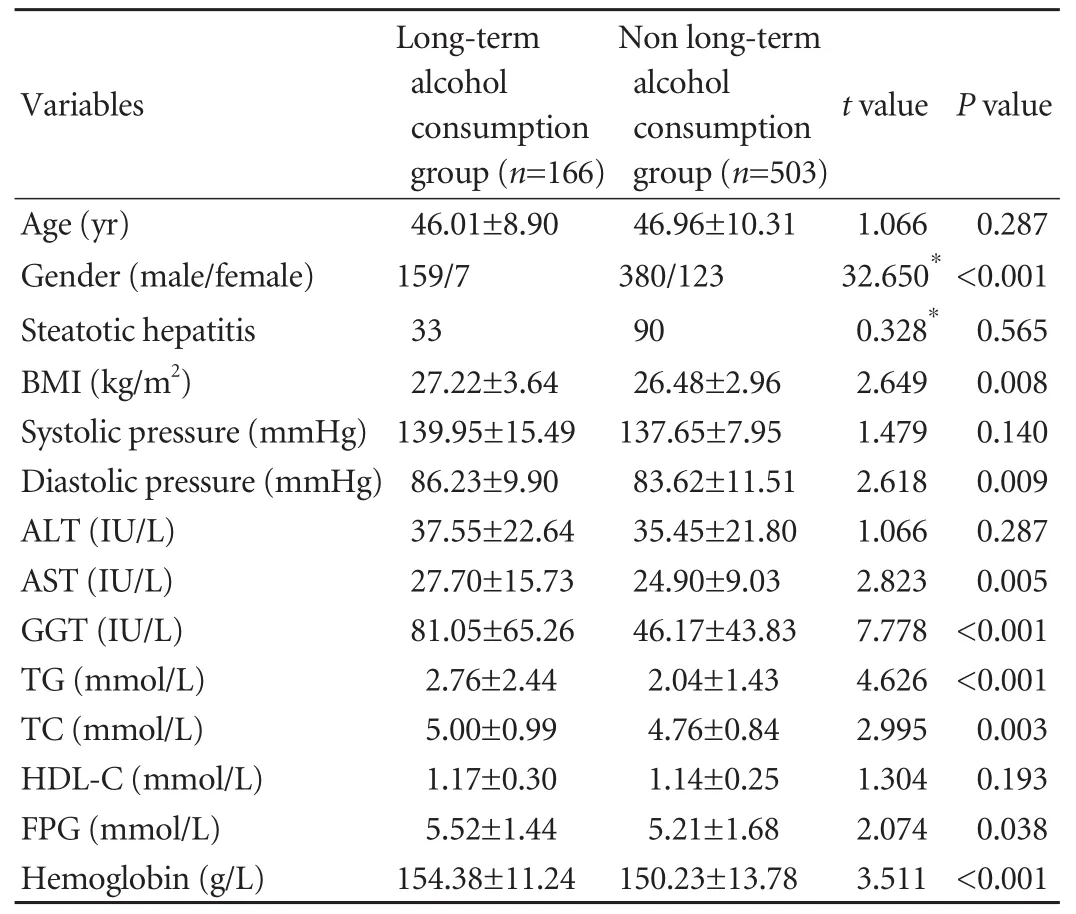
Table 1.Comparison of clinical and laboratory data between the long-term alcohol consumption group and non long-term alcohol consumption group
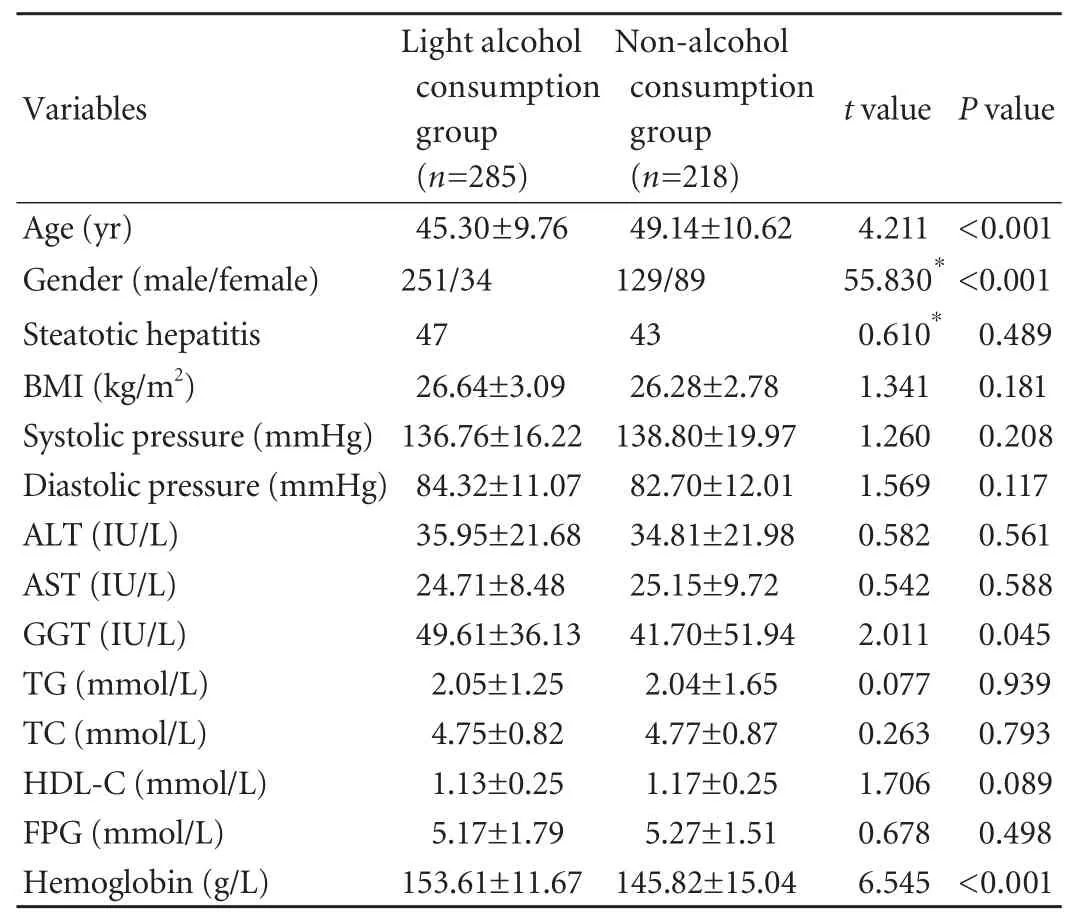
Table 2.Comparison of clinical and laboratory data between light alcohol consumption group and non-alcohol consumption group
Discussion
In this study alcohol consumption was found to be closely associated with clinical and laboratory data of patients with fatty liver.Patients with light alcohol consumption had higher levels of serum GGT and hemoglobin,and long-term heavy consumption could contribute to the elevation of BMI,diastolic pressure,AST,TG,TC,and FPG except GGT and hemoglobin.
There are less reports on the effect of alcohol consumption on the level of hemoglobin of patients with fatty liver,and whether alcohol consumption has direct impact on the level of hemoglobin is unknown.Studies[10-12]found that there were certain regular relations between the reference value of hemoglobin and geographical factors.It has been postulated that geographical factors affect the level of hemoglobin of people,for instance,atmospheric conditions,water quality,soil structure,and local dietary structure and habits.Thefive geographical factors including altitude,annual sunshine hours,relative humidity,annual average temperature and annual precipitation are significantly correlated with the hemoglobin levels of local residents.[12]The level of hemoglobin elevates along with the increase of altitude and annual sunshine hours.When altitude rises and oxygen content decreases gradually,red blood cells have a compensatory increase in hypoxic condition.In addition,high temperature usually causes hemodilution and reduction of blood viscosity,leading to an increased erythrocyte sedimentation rate and a decreased hemoglobin level.[13]In our study,the level of hemoglobin in patients with long-term alcohol consumption was remarkably higher than that in patients without long-term alcohol consumption.It is suggested that hemoglobin values are potential markers for estimating the level of alcohol consumption in patients with fatty liver.
Moreover,serum GGT level is significantly associated with the level of alcohol consumption in patients with fatty liver.It is suggested to be an early and sensitive enzyme related to oxidative stress.[14,15]Increased alcohol consumption may increase the severity of oxidative stress and thereby increase serum GGT levels.In addition,serum GGT level was found to be a surrogate marker of insulin resistance,in flammation and metabolic syndrome.[16]This may partially explain why the patients with higher GGT levels were associated with elevated BMI,diastolic pressure,TG,TC and FPG (Table 1).
The subjects in this study were the employees from other companies taking annual health examination at our hospital.Most of the subjects were apparently healthy,this is why the level of hemoglobin or GGT was not significantly different between the group with longterm alcohol consumption and the group without longterm alcohol consumption.Although the difference was not significant,our analysis suggested that mild change of serum hemoglobin or GGT level is also significantly associated with alcohol consumption in fatty liver patients.Studies with a large number of subjects are necessary to confirm these results and to identify the prognostic values of hemoglobin and GGT in fatty liver patients.
Funding:None.
Ethical approval:Not needed.
Contributors:WXF proposed the study.YM analyzed the data and wrote the first draft.Both authors contributed to the design and interpretation of the study and to further drafts.WXF is the guarantor.
Competing interest:No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
1 Angulo P.Nonalcoholic fatty liver disease.N Engl J Med 2002;346:1221-1231.
2 Jimba S,Nakagami T,Takahashi M,Wakamatsu T,Hirota Y,Iwamoto Y,et al.Prevalence of non-alcoholic fatty liver disease and its association with impaired glucose metabolism in Japanese adults.Diabet Med 2005;22:1141-1145.
3 Fan JG,Farrell GC.Epidemiology of non-alcoholic fatty liver disease in China.J Hepatol 2009;50:204-210.
4 Li Y,Xu C,Yu C,Xu L,Miao M.Association of serum uric acid level with non-alcoholic fatty liver disease:a crosssectional study.J Hepatol 2009;50:1029-1034.
5 Adams LA,Lymp JF,St Sauver J,Sanderson SO,Lindor KD,Feldstein A,et al.The natural history of nonalcoholic fatty liver disease:a population-based cohort study.Gastroenterology 2005;129:113-121.
6 Neuschwander-Tetri BA,Caldwell SH.Nonalcoholic steatohepatitis:summary of an AASLD Single Topic Conference.Hepatology 2003;37:1202-1219.
7 Marchesini G,Bugianesi E,Forlani G,Cerrelli F,Lenzi M,Manini R,et al.Nonalcoholic fatty liver,steatohepatitis,and the metabolic syndrome.Hepatology 2003;37:917-923.
8 Marchesini G,Brizi M,Bianchi G,Tomassetti S,Bugianesi E,Lenzi M,et al.Nonalcoholic fatty liver disease:a feature of the metabolic syndrome.Diabetes 2001;50:1844-1850.
9 Xu C,Yu C,Xu L,Miao M,Li Y.High serum uric acid increases the risk for nonalcoholic fatty liver disease:a prospective observational study.PLoS One 2010;5:e11578.
10 Miao G.Normal reference value of hemoglobin of older boys and geographical factors.Biosci Rep 2003;23:305-312.
11 Milman N,Pedersen AN,Ovesen L,Schroll M.Hemoglobin concentrations in 358 apparently healthy 80-year-old Danish men and women.Should the reference interval be adjusted for age? Aging Clin Exp Res 2008;20:8-14.
12 Miao G.The relationship between the reference value of erythrocyte sedimentation rate and geographical factors.Biosci Rep 2001;21:287-292.
13 Samaja M,Crespi T,Guazzi M,Vandegriff KD.Oxygen transport in blood at high altitude:role of the hemoglobinoxygen affinity and impact of the phenomena related to hemoglobin allosterism and red cell function.Eur J Appl Physiol 2003;90:351-359.
14 Lee DH,Blomhoff R,Jacobs DR Jr.Is serum gamma glutamyltransferase a marker of oxidative stress? Free Radic Res 2004;38:535-539.
15 Simao AN,Dichi JB,Barbosa DS,Cecchini R,Dichi I.In fluence of uric acid and gamma-glutamyltransferase on total antioxidant capacity and oxidative stress in patients with metabolic syndrome.Nutrition 2008;24:675-681.
16 Lee MY,Koh SB,Koh JH,Nam SM,Shin JY,Shin YG,et al.Relationship between gamma-glutamyltransferase and metabolic syndrome in a Korean population.Diabet Med 2008;25:469-475.
杂志排行
Hepatobiliary & Pancreatic Diseases International的其它文章
- Predictors of patient survival following living donor liver transplantation
- Hepatocellular carcinoma HepG2 cell apoptosis and caspase-8 and Bcl-2 expression induced by injectable seed extract of Coix lacryma-jobi
- A new scoring system for assessment of liver function after successful hepatectomy in patients with hepatocellular carcinoma
- Oncofetal antigen glypican-3 as a promising early diagnostic marker for hepatocellular carcinoma
- Necessity and indications of invasive treatment for Budd-Chiari syndrome
- Evaluation of hepatitis B viral replication and proteomic analysis of HepG2.2.15 cell line after knockdown of HBx