Outcomes and mechanisms of ischemic preconditioning in liver transplantation
2010-12-14ShengYanLiMingJinYuanXingLiuLinZhouHaiYangXieandShuSenZheng
Sheng Yan, Li-Ming Jin, Yuan-Xing Liu, Lin Zhou, Hai-Yang Xie and Shu-Sen Zheng
Hangzhou, China
Outcomes and mechanisms of ischemic preconditioning in liver transplantation
Sheng Yan, Li-Ming Jin, Yuan-Xing Liu, Lin Zhou, Hai-Yang Xie and Shu-Sen Zheng
Hangzhou, China
(Hepatobiliary Pancreat Dis Int 2010; 9: 346-354)
liver regeneration;ischemia/reperfusion injury;ischemic preconditioning;hepatectomy;liver transplantation
Introduction
Liver transplantation is so far the most effective therapeutic modality for end-stage liver diseases.Several non-immunological elements such as blood loss, ischemia/reperfusion (I/R) injury and regeneration capacity are associated with the outcome of liver transplantation. Hepatic in fl ow occlusion,termed as Pringle's maneuver,[1]represents an effective strategy to reduce blood loss and transfusion requirements in liver surgery, thus facilitating the technical development of liver transplantation.[2,3]However, this surgical strategy may contribute to hepatic I/R injury which impairs remnant liver/reducedsize-graft regeneration[4-7]as well as graft dysfunction after liver transplantation.[8-11]On the other hand, liver regeneration should be considered as a fundamental factor for partial liver transplantation including living donor liver transplantation (LDLT) and split liver transplantation. Ischemic preconditioning (IPC) as a practical strategy in theory not only protects the liver against I/R injury[12,13]but also enhances the capacity of liver regeneration.[14-17]IPC, which was described initially by Murry et al[18]in an animal model, refers to a brief period of I/R which can render an organ resistant to a more prolonged episode of ischemia, and it is generally evidenced with controversy.[4,13,19-24]Although investigators have attempted to explore the mechanism of IPC, the exact mechanism of IPC in liver transplantation is still not fully understood. In this article we reviewed a series of clinical and experimentalstudies in an attempt to investigate the protective effect and mechanism of IPC in liver transplantation.
Mechanisms of IPC
The protective mechanisms of IPC against hepatic I/R injury include alterations in energy metabolism,neutrophil accumulation, microcirculatory disturbances,liver regeneration, and formation of pro-in fl ammatory mediators.
Effect of IPC on energy metabolism
Mitochondria are the main energy production source for cells relevant to glutamate-/malate- or succinate oxidation.[25]Mitochondrial permeability transition leads to a rising permeability of the inner mitochondrial membrane, and consequently results in ATP depletion.[25]IPC might directly inhibits the negative effects of nonesteri fi ed fatty acids on β-oxidation or on the respiratory chain of mitochondria by protection of the mitochondrial permeability transition.[25,26]Among various protective mechanisms, the preservation of hepatic ATP contents plays an important role in mitigating I/R injury. A randomized controlled trial showed that IPC reduced metabolic cost of repairing more severe injuries.[27]IPC preserves hepatic energy metabolism via the downregulation of cellular ATP metabolism, thus enhancing nitric oxide (NO) synthesis and lowering arginase activity and lipid peroxidation.[28,29]Recent studies have shown that ATP-preserving effect of IPC is associated with increased expression of hepatic ATP synthase and its beta subunit.[25,30]
IPC and reactive oxygen species (ROSs)
ROSs deriving from activated Kupffer cells and neutrophils are one of the major detrimental elements in hepatic I/R injury. Xanthine dehydrogenase is converted to the oxygen radical-producing form xanthine oxidase(XOD) by I/R. Meanwhile, there is an accumulation of the substrate for XOD, xanthine. IPC is able to reduce the accumulation of xanthine and the conversion of xanthine dehydrogenase to XOD in liver grafts during cold ischemia. This endogenous protective mechanism has the capacity to block xanthine/XOD generation in liver grafts during cold ischemia.[31]Under reperfusion,XOD reacts with molecular oxygen to produce ROSs,which trigger a detrimental cascade, including cellular disintegration and microcirculatory dysfunction.Oxidative stress directly causes hepatocyte and/or sinusoidal endothelial cell (SEC) damage, whereas the soluble factors are largely responsible for the recruitment and activation of leukocytes. IPC can increase the hepatic tolerance to I/R injury by attenuating ROS production and oxidative stress.[32-34]By decreasing GSH depletion, IPC could be more effective in resisting ROS responses during hepatic ischemia.[35]A recent study suggested that IPC response is associated with the upregulation of mitochondrial superoxide dismutase and the decrease of ROS production.[36]
Effective role of IPC on hepatic microcirculation NO and endothelin
Hepatic microcirculation was modulated by vasoactive substances such as NO and endothelin, which balance a perfect intrahepatic microcirculation status via regulation of detailed vascular caliber and mediation of the sinusoidal perfusion.[37,38]Hepatic I/R imbalances the endogenous production of NO and endothelin,therefore distorts the sinusoidal lumen with consequently decreased leukocyte velocity and decreased perfusion.[9,39]The blockade of endogenous NO can aggravate microvascular and hepatocellular injury during the period of post-ischemic reperfusion.[40-42]IPC provides a better preservation of hepatic microcirculation,[43]with the effect similar to that induced by administering L-arginine and L-NAME, indicating that NO plays an important role in improving microcirculation.[37]After the blockade of NO, the remission of microcirculatory disturbance obliterated.[35,44]
SEC and adhesion molecules
The alteration of hepatic microcirculation is regarded as a critical target after hepatic I/R injury.[39,45]The underlying mechanisms of microcirculatory failure include narrowing of the sinusoid lumens due to the swelling of Kupffer cell, SEC[39]and hepatocyte.[37]Microcirculatory failure after I/R characterized by "nore fl ow" in sinusoids and "re fl ow-paradox" is associated with activation of Kupffer cell and release of in fl ammatory cytokines.[46]The over-expression of adhesion molecules(ICAM-1, VCAM-1, LFA, β2 integrin, E-selectin, etc) after I/R induces rolling of leukocytes along the endothelium of post-sinusoidal venules, which subsequently adhere to the SEC.[46,47]Kupffer cell and neutrophils are activated and release a series of in fl ammatory cytokines such as IL-1, IL-2, IL-4, IL-6 and TNF-α, which in turn activate leukocytes and increase the release of ROSs.[48-51]Studies have shown that the down-regulation of adhesion molecules can attenuate hepatic I/R injury.[51-55]
In 1999, Sawaya et al[56]found that IPC attenuated the status of rolling and adhesion of leukocyte, which decreases neutrophil in fi ltration in the liver. Indeed,the protection of IPC is closely related to the decrease of endothelial-leukocyte interaction.[57]Koti et al[58]found that the transient preconditioning episodes with hydrogen peroxide inhibited the expression of adhesion molecules and in fl ammatory factors by blockade of the NF-κB and mitogen-activated protein kinases(MAPK) signal transcription pathways.[59,60]Similarly,two in vitro studies of SEC suggested that the effect of IPC attributes to a decreased adhesion of neutrophils,secondary to a decreased production of endothelial adhesion molecules.[61,62]Although Peralta et al[63]suggested that neutrophil accumulation in the liver at 90 minutes of reperfusion after IPC did not induce the upregulation of ICAM-1, endothelial preconditioning may well explain the anti-adhesive effect of IPC.[64]
Mechanism of liver regeneration of IPC
Liver regeneration is a complex biological process,including numerous cellular components and mediators such as IL-6, TNF-α, signal transducer and activator of transcription (STAT)-3, stellate cells, and platelets.[65,66]Among these components and mediators, IL-6 and TNF-α are a sort of pleiotropic cytokine, which plays a central role in the process of in fl ammation and regeneration.[15,17,67,68]TNF-α promotes cell proliferation by inducing IL-6 production, and the regeneration is activated via the up-regulation of NF-κB,[67]while activating STAT-3.[68-70]STAT-3 is crucial for cell cycle progression in hepatocytes during liver regeneration.After STAT-3 and MAPK cascade are activated by the binding of cytokines like TNF-α and IL-6, the control of the intracellular signal transduction pathway is involved in liver regeneration. For instance, upon nuclear shuttling, STAT-3 binds to the promoter of immediate early genes and activates the MAPK pathway,like MAPK (p38) and c-Jun N-terminal kinase,[71-73]which in turn triggers the production of DNA synthesis proteins, like proliferating cell nuclear antigen (PCNA)protein.[74]The p38 directly regulates cell proliferation and differentiation, and is indirectly involved in the regulation of NF-κB-dependent transcriptional activity.[75,76]Thus, IPC inhibits the production of TNF-α at the early phase after reperfusion, but not IL-6 at the late phase of reperfusion in rats. Bedirli et al[17]suggested that IPC ameliorates hepatic I/R injury, and stimulates liver regeneration by a TNF-α/IL-6-dependent pathway as well. IPC improves the regeneration of small-for-size liver grafts, which involves in energy metabolism most likely by up-regulating mitochondrial superoxide dismutase and decreasing ROS production.[36,77]The facilitation of IPC for liver regeneration will be an option for the development of new strategies in LDLT.
Application of IPC in liver transplantation Whether is IPC a friendly strategy to LDLT?
LDLT as an established alternative to deceased donor liver transplantation (DDLT), has additional risk for the donor.[78,79]In almost all liver transplant centers donor hepatectomy has been performed in LDLT in the absence of hilar occlusion to avoid I/R injury.[80-85]A number of clinical trials, however, con fi rmed that in fl ow occlusion can be applied to living donor hepatectomy without graft injury.[86,87]Moreover transaction surface remains blood free, which decreases the risk to the donor in LDLT.[87]Thus in fl ow occlusion technique is used in a number of cases in which part of the graft can be completely ischemic during liver parenchymal dissection, and it has been con fi rmed that Pringle's technique does not elevate postoperative AST levels and can be used in donor hepatectomy. This technique makes hepatectomy more precisely and meticulously with least surgical injuries and anatomical complications.[86]In 2000, Clavien et al[88]initiated IPC strategy in clinical practice, indicating that IPC was promising in hepatectomy for preventing bleeding and lowering the risk of surgery in healthy donors. In fact,IPC not only prevents the liver from I/R injury but also decreases the intraoperative blood loss. Nuzzo et al[89]have evaluated the safety of IPC in a prolonged period of clamping in 42 consecutive patients with healthy liver for hepatectomy. The results indicated that IPC with Pringle's maneuver controls intraoperative bleeding. Thus IPC is considered effective to control bleeding and protect donors and grafts function during the procurement of LDLT. In fact many surgeons often delineate some lines of demarcation via clamping the entire hepatoduodenal ligament or the lobar in fl ow vessels for a brief period before liver resection, including LDLT. Fung[90]also support that this clamping invokes the same protective responses of IPC in liver surgery.
Increasingly successful hepatectomy documents using IPC strategy[21,88,91-94]also imply the potential bene fi ts of IPC to the harvesting from the living donor. Arai et al[95]suggested that it is feasible to precondition liver tissue before liver donation in LDLT.Most recently, Chouker et al[93]reported that IPC offers a better intraoperative hemodynamic stability by lowering the need for catecholamine. Furthermore,the simple strategy offers further advantages and brings preconditioning closer to organ harvesting.[13]Therefore, IPC as a modi fi ed Pringle's maneuver should not be hesitatedly used by surgeons during LDLT, at least it should be conducted in a series of clinical trials.However, evidence is insuf fi cient for the establishment of a protective theory of IPC against donor and graft injury during LDLT (Tables 1-3).
IPC and partial liver transplantation
The capacity of regeneration after partial liver transplantation is an elementary contributor to the clinical outcome.[96,97]The effect of IPC on liver cell cycle is associated with the production of IL-6.[67,68]Matsumoto et al[15]found that the liver regeneration mechanism of IPC against total hepatic I/R injury was induced by the modulation of the IL-6/STAT-3 signaling pathway.
The adverse effect on liver regeneration is thought to be induced by drastic reduction in the hepatic microvascular bed, leading to excessive portal perfusion injury in a small-for-size liver graft.[98-101]As mentioned, IPC is potentially able to improve liver regeneration after LDLT. Franco-Gou et al[6]suggested that IPC promoted liver regeneration by increasing PCNA indices and hepatocyte growth factor levels. In addition, IPC decreases liver injury after reperfusion and improves graft survival after whole and partial liver transplantation.[95,102]This may be a bene fi cial IPC effect on reduced-size liver transplantation via blocking mitochondrial depolarization. Although a clinical observation revealed that IPC was likely to be ineffective in case of hepatic volume loss above 50%,[103]most experimental studies claimed that IPC can improve hepatic proliferation if hepatectomy is not more than 70%.[17,99,104]In addition, other supplementary strategies plus IPC may induce liver regeneration with a graft size of 30% or less in LDLT.[104]Arai et al[77]indicated that IPC enhances the capacity of liver regeneration after 70% hepatectomy.
Besides, the duration of liver ischemic injury may impair its regeneration. Yamada et al[105]foundthat IPC with 40 minutes ischemia had a better regenerative capacity than that with 2-hour ischemia.Another study also showed that IPC maintains liver regeneration capacity by enhancing survival signals but fails to prevent I/R injury in the liver subjected to warm ischemia for more than 60 minutes.[16]However,unilateral IPC prior to graft procurement does not produce any bene fi cial clinical effect or trigger any signi fi cant protective effect on tissue (Tables 1-3).[106]

Table 1. Liver regeneration of IPC after partial hepatectomy in rodents
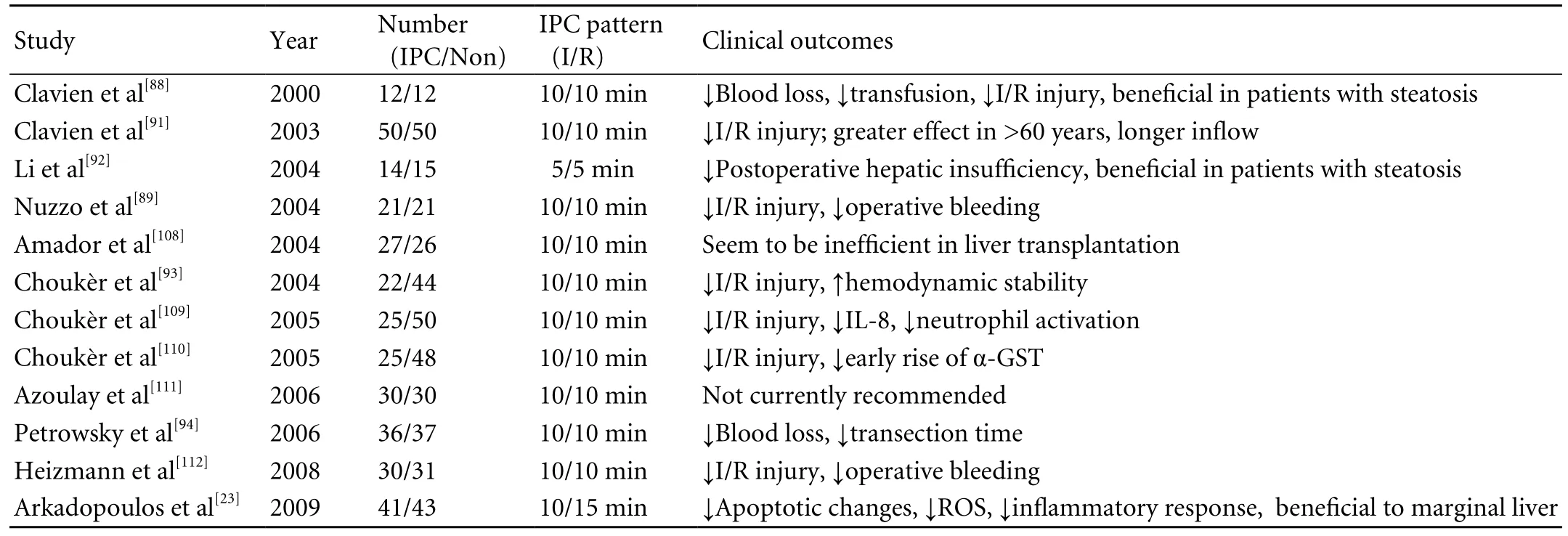
Table 2. Clinical studies of IPC in hepatectomy

Table 3. Prospective clinical trials of IPC in LDLT and DDLT
IPC and DDLT
To our knowledge, Azoulay et al[115]fi rst demonstrated the protective effect of IPC in DDLT. Although various basic and clinical studies of IPC were performed, the role of IPC or its protective effect in DDLT remains controversial.[8,119]IPC has the potential to ameliorate graft injury and decrease morbidity after liver transplantation. However, Koneru et al[114]observed that deceased donor liver with 5-minute I/R does not induce a response to IPC, showing two possibilities:5-minute preconditioning interval is too short to induce protection; and protective response is too slender. Two years later, however, they found that a trend towards fewer moderate/severe rejections is related to IPC via upregulating the expression of IL-10 after DDLT.[117]Similarly, Jassem et al[116,120]reported that IPC confers protection against in fl ammatory responses, which are associated with the impairment of cadaveric liver graft function in a long period.
Although IPC causes an early decreased allograft function, a previous clinical trial[115]indicated that IPC provides a better tolerance to ischemia. Subsequently,Cescon et al[121]found that 10-minute IPC has a signi fi cant bene fi cial effect on reduction of ALT in a deceased donor allograft, but it has no clinical bene fi t.A recent randomized clinical trial showed that IPC decreases postoperative liver enzymes, improves signi fi cantly biochemical markers of liver function, and reduces the probability of reoperation (Table 3).[22]
Funding: This study was supported by grants from the National Key Technology R&D Program in the Eleventh Five-Year Plan of China (No. 2008BAI60B02 and 2008BAI60B06), and the National Natural Science Foundation of China (No. 30700769).
Ethical approval: Not needed.
Contributors: YS wrote the fi rst draft of this paper. All authors contributed to the intellectual context and approved the fi nal version. ZSS is the guarantor.
Competing interest: No bene fi ts in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
1 Pringle JH. V. Notes on the arrest of hepatic hemorrhage due to trauma. Ann Surg 1908;48:541-549.
2 Nakajima Y, Shimamura T, Kamiyama T, Matsushita M, Sato N, Todo S. Control of intraoperative bleeding during liver resection: analysis of a questionnaire sent to 231 Japanese hospitals. Surg Today 2002;32:48-52.
3 Breitenstein S, Apestegui C, Petrowsky H, Clavien PA."State of the art" in liver resection and living donor liver transplantation: a worldwide survey of 100 liver centers.World J Surg 2009;33:797-803.
4 Suzuki S, Inaba K, Konno H. Ischemic preconditioning in hepatic ischemia and reperfusion. Curr Opin Organ Transplant 2008;13:142-147.
5 Selzner M, Camargo CA, Clavien PA. Ischemia impairs liver regeneration after major tissue loss in rodents: protective effects of interleukin-6. Hepatology 1999;30:469-475.
6 Franco-Gou R, Peralta C, Massip-Salcedo M, Xaus C, Serafín A, Roselló-Catafau J. Protection of reduced-size liver for transplantation. Am J Transplant 2004;4:1408-1420.
7 Watanabe M, Chijiiwa K, Kameoka N, Yamaguchi K, Kuroki S,Tanaka M. Gadolinium pretreatment decreases survival and impairs liver regeneration after partial hepatectomy under ischemia/reperfusion in rats. Surgery 2000;127:456-463.
8 DeOliveira ML, Graf R, Clavien PA. Ischemic preconditioning:promises from the laboratory to patients--sustained or disillusioned? Am J Transplant 2008;8:489-491.
9 Banga NR, Homer-Vanniasinkam S, Graham A, Al-Mukhtar A, White SA, Prasad KR. Ischaemic preconditioning in transplantation and major resection of the liver. Br J Surg 2005;92:528-538.
10 Strasberg SM, Howard TK, Molmenti EP, Hertl M. Selecting the donor liver: risk factors for poor function after orthotopic liver transplantation. Hepatology 1994;20:829-838.
11 Heaton N. Small-for-size liver syndrome after auxiliary and split liver transplantation: donor selection. Liver Transpl 2003;9:S26-28.
12 Furrer K, Deoliveira ML, Graf R, Clavien PA. Improving outcome in patients undergoing liver surgery. Liver Int 2007;27:26-39.
13 Ambros JT, Herrero-Fresneda I, Borau OG, Boira JM.Ischemic preconditioning in solid organ transplantation:from experimental to clinics. Transpl Int 2007;20:219-229.
14 Kerem M, Bedirli A, O fl uoglu E, Deniz K, Turkozkan N,Pasaoglu H, et al. Ischemic preconditioning improves liver regeneration by sustaining energy metabolism after partial hepatectomy under ischemia in rats. Liver Int 2006;26:994-999.
15 Matsumoto T, O'Malley K, Efron PA, Burger C, McAuliffe PF, Scumpia PO, et al. Interleukin-6 and STAT3 protect the liver from hepatic ischemia and reperfusion injury during ischemic preconditioning. Surgery 2006;140:793-802.
16 Yamada F, Saito T, Abe T, Tsuchiya T, Sato Y, Kenjo A, et al.Ischemic preconditioning enhances regenerative capacity of hepatocytes in long-term ischemically damaged rat livers. J Gastroenterol Hepatol 2007;22:1971-1977.
17 Bedirli A, Kerem M, Pasaoglu H, Erdem O, O fl uoglu E,Sakrak O. Effects of ischemic preconditioning on regenerative capacity of hepatocyte in the ischemically damaged rat livers.J Surg Res 2005;125:42-48.
18 Murry CE, Jennings RB, Reimer KA. Preconditioning with ischemia: a delay of lethal cell injury in ischemic myocardium. Circulation 1986;74:1124-1136.
19 Montalvo-Jave EE, Pina E, Montalvo-Arenas C, Urrutia R, Benavente-Chenhalls L, Pena-Sanchez J, et al. Role of ischemic preconditioning in liver surgery and hepatic transplantation. J Gastrointest Surg 2009;13:2074-2083.
20 Zahler S, Kupatt C, Becker BF. Endothelial preconditioning by transient oxidativstress reduces in fl ammatory responses of cultured endothelial cells to TNF-alpha. FASEB J 2000;14:555-564.
21 Clavien PA, Petrowsky H, DeOliveira ML, Graf R. Strategies for safer liver surgery and partial liver transplantation. N Engl J Med 2007;356:1545-1559.
22 Amador A, Grande L, Martí J, Deulofeu R, Miquel R, Solá A, et al. Ischemic pre-conditioning in deceased donor liver transplantation: a prospective randomized clinical trial. Am J Transplant 2007;7:2180-2189.
23 Arkadopoulos N, Kostopanagiotou G, Theodoraki K,Farantos C, Theodosopoulos T, Stafyla V, et al. Ischemic preconditioning confers antiapoptotic protection during major hepatectomies performed under combined in fl ow and out fl ow exclusion of the liver. A randomized clinical trial.World J Surg 2009;33:1909-1915.
24 Franchello A, Gilbo N, David E, Ricchiuti A, Romagnoli R,Cerutti E, et al. Ischemic preconditioning (IP) of the liver as a safe and protective technique against ischemia/reperfusion injury (IRI). Am J Transplant 2009;9:1629-1639.
25 Rolo AP, Teodoro JS, Peralta C, Rosello-Catafau J, Palmeira CM. Prevention of I/R injury in fatty livers by ischemic preconditioning is associated with increased mitochondrial tolerance: the key role of ATPsynthase and mitochondrial permeability transition. Transpl Int 2009;22:1081-1090.
26 Murphy E, Steenbergen C. Preconditioning: the mitochondrial connection. Annu Rev Physiol 2007;69:51-67.
27 Patel A, van de Poll MC, Greve JW, Buurman WA, Fearon KC,McNally SJ, et al. Early stress protein gene expression in a human model of ischemic preconditioning. Transplantation 2004;78:1479-1487.
28 Selzner N, Selzner M, Jochum W, Clavien PA. Ischemic preconditioning protects the steatotic mouse liver against reperfusion injury: an ATP dependent mechanism. J Hepatol 2003;39:55-61.
29 O fl uoglu E, Kerem M, Pasaoglu H, Turkozkan N, Seven I, Bedirli A, et al. Delayed energy protection of ischemic preconditioning on hepatic ischemia/reperfusion injury in rats. Eur Surg Res 2006;38:114-121.
30 Xu C, Zhang X, Yu C, Lu G, Chen S, Xu L, et al. Proteomic analysis of hepatic ischemia/reperfusion injury and ischemic preconditioning in mice revealed the protective role of ATP5beta. Proteomics 2009;9:409-419.
31 Fernández L, Heredia N, Grande L, Gómez G, Rimola A,Marco A, et al. Preconditioning protects liver and lung damage in rat liver transplantation: role of xanthine/xanthine oxidase. Hepatology 2002;36:562-572.
32 Cutrn JC, Perrelli MG, Cavalieri B, Peralta C, Rosell Catafau J, Poli G. Microvascular dysfunction induced by reperfusion injury and protective effect of ischemic preconditioning. Free Radic Biol Med 2002;33:1200-1208.
33 Yuan GJ, Ma JC, Gong ZJ, Sun XM, Zheng SH, Li X.Modulation of liver oxidant-antioxidant system by ischemic preconditioning during ischemia/reperfusion injury in rats.World J Gastroenterol 2005;11:1825-1828.
34 Navarro-Sabaté A, Peralta C, Calvo MN, Manzano A, Massip-Salcedo M, Roselló-Catafau J, et al. Mediators of rat ischemic hepatic preconditioning after cold preservation identi fi ed by microarray analysis. Liver Transpl 2006;12:1615-1625.
35 Serafín A, Roselló-Catafau J, Prats N, Xaus C, Gelpí E,Peralta C. Ischemic preconditioning increases the tolerance of Fatty liver to hepatic ischemia-reperfusion injury in the rat. Am J Pathol 2002;161:587-601.
36 Rehman H, Connor HD, Ramshesh VK, Theruvath TP, Mason RP, Wright GL, et al. Ischemic preconditioning prevents free radical production and mitochondrial depolarization in smallfor-size rat liver grafts. Transplantation 2008;85:1322-1331.
37 Koti RS, Yang W, Dashwood MR, Davidson BR, Seifalian AM.Effect of ischemic preconditioning on hepatic microcirculation and function in a rat model of ischemia reperfusion injury.Liver Transpl 2002;8:1182-1191.
38 Murry CE, Richard VJ, Reimer KA, Jennings RB. Ischemic preconditioning slows energy metabolism and delays ultrastructural damage during a sustained ischemic episode.Circ Res 1990;66:913-931.
39 Serracino-Inglott F, Habib NA, Mathie RT. Hepatic ischemiareperfusion injury. Am J Surg 2001;181:160-166.
40 Ishikawa Y, Yamamoto Y, Kume M, Yamagami K, Yamamoto H, Kimoto S, et al. Heat shock preconditioning on mitochondria during warm ischemia in rat livers. J Surg Res 1999;87:178-184.
41 Pannen BH, Al-Adili F, Bauer M, Clemens MG, Geiger KK.Role of endothelins and nitric oxide in hepatic reperfusion injury in the rat. Hepatology 1998;27:755-764.
42 Wang Y, Mathews WR, Guido DM, Farhood A, Jaeschke H.Inhibition of nitric oxide synthesis aggravates reperfusion injury after hepatic ischemia and endotoxemia. Shock 1995;4:282-288.
43 Man K, Lo CM, Liu CL, Zhang ZW, Lee TK, Ng IO, et al.Effects of the intermittent Pringle manoeuvre on hepatic gene expression and ultrastructure in a randomized clinical study. Br J Surg 2003;90:183-189.
44 Caban A, Oczkowicz G, Abdel-Samad O, Cierpka L.In fl uence of ischemic preconditioning and nitric oxide on microcirculation and the degree of rat liver injury in the model of ischemia and reperfusion. Transplant Proc 2006;38:196-198.45 Menger MD, Vollmar B. Role of microcirculation in transplantation. Microcirculation 2000;7:291-306.
46 Liu YX, Jin LM, Zhou L, Xie HY, Jiang GP, Wang Y, et al.Mycophenolate mofetil attenuates liver ischemia/reperfusion injury in rats. Transpl Int 2009;22:747-756.
47 Ley K, Laudanna C, Cybulsky MI, Nourshargh S. Getting to the site of in fl ammation: the leukocyte adhesion cascade updated. Nat Rev Immunol 2007;7:678-689.
48 Donnahoo KK, Meng X, Ao L, Ayala A, Shames BD, Cain MP, et al. Differential cellular immunolocalization of renal tumour necrosis factor-alpha production during ischaemia versus endotoxaemia. Immunology 2001;102:53-58.
49 Nakao A, Neto JS, Kanno S, Stolz DB, Kimizuka K, Liu F, et al. Protection against ischemia/reperfusion injury in cardiac and renal transplantation with carbon monoxide, biliverdin and both. Am J Transplant 2005;5:282-291.
50 Carini R, Albano E. Recent insights on the mechanisms of liver preconditioning. Gastroenterology 2003;125:1480-1491.
51 Jaeschke H, Hasegawa T. Role of neutrophils in acute in fl ammatory liver injury. Liver Int 2006;26:912-919.
52 Dold S, Laschke MW, Lavasani S, Menger MD, Thorlacius H.Cholestatic liver damage is mediated by lymphocyte function antigen-1-dependent recruitment of leukocytes. Surgery 2008;144:385-393.
53 Rajesh M, Pan H, Mukhopadhyay P, Bátkai S, Osei-Hyiaman D, Haskó G, et al. Cannabinoid-2 receptor agonist HU-308 protects against hepatic ischemia/reperfusion injury by attenuating oxidative stress, in fl ammatory response, and apoptosis. J Leukoc Biol 2007;82:1382-1389.
54 Hafez T, Moussa M, Nesim I, Baligh N, Davidson B, Abdul-Hadi A. The effect of intraportal prostaglandin E1 on adhesion molecule expression, in fl ammatory modulator function, and histology in canine hepatic ischemia/reperfusion injury. J Surg Res 2007;138:88-99.
55 Teoh NC, Ito Y, Field J, Bethea NW, Amr D, McCuskey MK,et al. Diannexin, a novel annexin V homodimer, provides prolonged protection against hepatic ischemia-reperfusion injury in mice. Gastroenterology 2007;133:632-646.
56 Sawaya DE Jr, Brown M, Minardi A, Bilton B, Burney D,Granger DN, et al. The role of ischemic preconditioning in the recruitment of rolling and adherent leukocytes in hepatic venules after ischemia/reperfusion. J Surg Res 1999;85:163-170.
57 Howell JG, Zibari GB, Brown MF, Burney DL, Sawaya DE, Olinde JG, et al. Both ischemic and pharmacological preconditioning decrease hepatic leukocyte/endothelial cell interactions. Transplantation 2000;69:300-303.
58 Koti RS, Yang W, Glantzounis G, Quaglia A, Davidson BR,Seifalian AM. Effect of ischaemic preconditioning on hepatic oxygenation, microcirculation and function in a rat model of moderate hepatic steatosis. Clin Sci (Lond) 2005;108:55-63.
59 Li XC, Ma YF, Wang XH. Role of NF-kappaB as effector of IPC in donor livers before liver transplantation in rats.Transplant Proc 2006;38:1584-1587.
60 Teoh N, Dela Pena A, Farrell G. Hepatic ischemic preconditioning in mice is associated with activation of NF-kappaB, p38 kinase, and cell cycle entry. Hepatology 2002;36:94-102.
61 Beauchamp P, Richard V, Tamion F, Lallemand F, Lebreton JP, Vaudry H, et al. Protective effects of preconditioning in cultured rat endothelial cells: effects on neutrophil adhesion and expression of ICAM-1 after anoxia and reoxygenation.Circulation 1999;100:541-546.
62 Laude K, Beauchamp P, Thuillez C, Richard V. Endothelial protective effects of preconditioning. Cardiovasc Res 2002;55:466-473.
63 Peralta C, Fernández L, Panés J, Prats N, Sans M, Piqué JM,et al. Preconditioning protects against systemic disorders associated with hepatic ischemia-reperfusion through blockade of tumor necrosis factor-induced P-selectin upregulation in the rat. Hepatology 2001;33:100-113.
64 Jerome SN, Akimitsu T, Gute DC, Korthuis RJ. Ischemic preconditioning attenuates capillary no-re fl ow induced by prolonged ischemia and reperfusion. Am J Physiol 1995;268:H2063-2067.
65 Pereboom IT, Lisman T, Porte RJ. Platelets in liver transplantation: friend or foe? Liver Transpl 2008;14:923-931.66 Lesurtel M, Graf R, Aleil B, Walther DJ, Tian Y, Jochum W,et al. Platelet-derived serotonin mediates liver regeneration.Science 2006;312:104-107.
67 Taub R. Liver regeneration: from myth to mechanism. Nat Rev Mol Cell Biol 2004;5:836-847.
68 Cressman DE, Greenbaum LE, DeAngelis RA, Ciliberto G,Furth EE, Poli V, et al. Liver failure and defective hepatocyte regeneration in interleukin-6-de fi cient mice. Science 1996;274:1379-1383.
69 Kovalovich K, DeAngelis RA, Li W, Furth EE, Ciliberto G,Taub R. Increased toxin-induced liver injury and fi brosis in interleukin-6-de fi cient mice. Hepatology 2000;31:149-159.
70 Camargo CA Jr, Madden JF, Gao W, Selvan RS, Clavien PA. Interleukin-6 protects liver against warm ischemia/reperfusion injury and promotes hepatocyte proliferation in the rodent. Hepatology 1997;26:1513-1520.
71 Sato M, Cordis GA, Maulik N, Das DK. SAPKs regulation of ischemic preconditioning. Am J Physiol Heart Circ Physiol 2000;279:H901-907.
72 Crenesse D, Gugenheim J, Hornoy J, Tornieri K, Laurens M,Cambien B, et al. Protein kinase activation by warm and cold hypoxia- reoxygenation in primary-cultured rat hepatocytes-JNK(1)/SAPK(1) involvement in apoptosis. Hepatology 2000;32:1029-1036.
73 Nagy N, Shiroto K, Malik G, Huang CK, Gaestel M,Abdellatif M, et al. Ischemic preconditioning involves dual cardio-protective axes with p38MAPK as upstream target. J Mol Cell Cardiol 2007;42:981-990.
74 Michalopoulos GK, DeFrances MC. Liver regeneration.Science 1997;276:60-66.
75 Ono K, Han J. The p38 signal transduction pathway:activation and function. Cell Signal 2000;12:1-13.
76 Fausto N. Liver regeneration. J Hepatol 2000;32:19-31.
77 Arai M, Tejima K, Ikeda H, Tomiya T, Yanase M, Inoue Y,et al. Ischemic preconditioning in liver pathophysiology. J Gastroenterol Hepatol 2007;22:S65-67.
78 Surman OS. The ethics of partial-liver donation. N Engl J Med 2002;346:1038.
79 Beavers KL, Sandler RS, Shrestha R. Donor morbidity associated with right lobectomy for living donor liver transplantation to adult recipients: a systematic review. Liver Transpl 2002;8:110-117.
80 Fan ST, Lo CM, Liu CL, Yong BH, Chan JK, Ng IO. Safety of donors in live donor liver transplantation using right lobe grafts. Arch Surg 2000;135:336-340.
81 Bak T, Wachs M, Trotter J, Everson G, Trouillot T, Kugelmas M, et al. Adult-to-adult living donor liver transplantation using right-lobe grafts: results and lessons learned from a single-center experience. Liver Transpl 2001;7:680-686.
82 Miller CM, Gondolesi GE, Florman S, Matsumoto C, Munoz L, Yoshizumi T, et al. One hundred nine living donor liver transplants in adults and children: a single-center experience.Ann Surg 2001;234:301-312.
83 Millis JM, Cronin DC, Brady LM, Newell KA, Woodle ES,Bruce DS, et al. Primary living-donor liver transplantation at the University of Chicago: technical aspects of the fi rst 104 recipients. Ann Surg 2000;232:104-111.
84 Pomfret EA, Pomposelli JJ, Lewis WD, Gordon FD, Burns DL,Lally A, et al. Live donor adult liver transplantation using right lobe grafts: donor evaluation and surgical outcome.Arch Surg 2001;136:425-433.
85 Marcos A, Ham JM, Fisher RA, Olzinski AT, Posner MP.Single-center analysis of the fi rst 40 adult-to-adult living donor liver transplants using the right lobe. Liver Transpl 2000;6:296-301.
86 Imamura H, Kokudo N, Sugawara Y, Sano K, Kaneko J,Takayama T, et al. Pringle's maneuver and selective in fl ow occlusion in living donor liver hepatectomy. Liver Transpl 2004;10:771-778.
87 Imamura H, Takayama T, Sugawara Y, Kokudo N, Aoki T,Kaneko J, et al. Pringle's manoeuvre in living donors. Lancet 2002;360:2049-2050.
88 Clavien PA, Yadav S, Sindram D, Bentley RC. Protective effects of ischemic preconditioning for liver resection performed under in fl ow occlusion in humans. Ann Surg 2000;232:155-162.
89 Nuzzo G, Giuliante F, Vellone M, De Cosmo G, Ardito F, Murazio M, et al. Pedicle clamping with ischemic preconditioning in liver resection. Liver Transpl 2004;10:S53-57.
90 Fung JJ. Ischemic preconditioning: application in clinical liver transplantation. Liver Transpl 2001;7:300-301.
91 Clavien PA, Selzner M, Rüdiger HA, Graf R, Kadry Z, Rousson V, et al. A prospective randomized study in 100 consecutive patients undergoing major liver resection with versus without ischemic preconditioning. Ann Surg 2003;238:843-852.
92 Li SQ, Liang LJ, Huang JF, Li Z. Ischemic preconditioning protects liver from hepatectomy under hepatic in fl ow occlusion for hepatocellular carcinoma patients with cirrhosis. World J Gastroenterol 2004;10:2580-2584.
93 Choukèr A, Schachtner T, Schauer R, Dugas M, Lohe F, Martignoni A, et al. Effects of Pringle manoeuvre and ischaemic preconditioning on haemodynamic stability in patients undergoing elective hepatectomy: a randomized trial. Br J Anaesth 2004;93:204-211.
94 Petrowsky H, McCormack L, Trujillo M, Selzner M, Jochum W, Clavien PA. A prospective, randomized, controlled trial comparing intermittent portal triad clamping versus ischemic preconditioning with continuous clamping for major liver resection. Ann Surg 2006;244:921-930.
95 Arai M, Thurman RG, Lemasters JJ. Ischemic preconditioning of rat livers against cold storage-reperfusion injury: role of nonparenchymal cells and the phenomenon of heterologous preconditioning. Liver Transpl 2001;7:292-299.
96 Lee SG, Park KM, Hwang S, Lee YJ, Kim KH, Ahn CS, et al.Adult-to-adult living donor liver transplantation at the Asan Medical Center, Korea. Asian J Surg 2002;25:277-284.
97 Dahm F, Georgiev P, Clavien PA. Small-for-size syndrome after partial liver transplantation: de fi nition, mechanisms of disease and clinical implications. Am J Transplant 2005;5:2605-2610.
98 Man K, Lo CM, Ng IO, Wong YC, Qin LF, Fan ST, et al.Liver transplantation in rats using small-for-size grafts: a study of hemodynamic and morphological changes. Arch Surg 2001;136:280-285.
99 Eipel C, Glanemann M, Nuessler AK, Menger MD, Neuhaus P, Vollmar B. Ischemic preconditioning impairs liver regeneration in extended reduced-size livers. Ann Surg 2005; 241:477-484.
100 Nakatsuka H, Sato Y, Yamamoto S, Hirano K, Kobayashi T, Takeishi T, et al. Analysis of liver injury following adult small-for-size grafts in liver transplantation. Transplant Proc 2003;35:80-81.
101 Tanaka K, Ogura Y. "Small-for-size graft" and "small-forsize syndrome" in living donor liver transplantation. Yonsei Med J 2004;45:1089-1094.
102 Franco-Gou R, Roselló-Catafau J, Casillas-Ramirez A,Massip-Salcedo M, Rimola A, Calvo N, et al. How ischaemic preconditioning protects small liver grafts. J Pathol 2006;208:62-73.
103 Serafín A, Fernández-Zabalegui L, Prats N, Wu ZY, Roselló-Catafau J, Peralta C. Ischemic preconditioning: tolerance to hepatic ischemia-reperfusion injury. Histol Histopathol 2004;19:281-289.
104 Yao A, Li X, Pu L, Zhong J, Liu X, Yu Y, et al. Impaired hepatic regeneration by ischemic preconditioning in a rat model of small-for-size liver transplantation. Transpl Immunol 2007;18:37-43.
105 Yamada F, Abe T, Saito T, Tsuciya T, Ishii S, Gotoh M.Ischemic preconditioning enhances regenerative capacity of hepatocytes after prolonged ischemia. Transplant Proc 2001;33:956.
106 Testa G, Angelova V, Laricchia-Robbio L, Rondelli D, Chejfec G, Anthony T, et al. Unilateral ischemic preconditioning and heterologous preconditioning in living donor liver transplantation. Clin Transplant 2009 Aug 27;[Epub ahead of print].
107 Qian Y, Liu Z, Geng X. Lack of protection of ischaemic preconditioning in the rat model of major hepatectomy with ischaemia reperfusion injury. Asian J Surg 2008;31:140-147.
108 Amador A, Marti J, Rodriguez-Laiz G, Bombuy E, Alvarez G, Ferrer J, et al. Ischemic preconditioning during donor procurement in orthotopic liver transplantation:preliminutesary results of a prospective and randomized trial. J Hepatol 2004;40:S37.
109 Choukèr A, Martignoni A, Schauer RJ, Rau HG, Volk A,Heizmann O, et al. Ischemic preconditioning attenuates portal venous plasma concentrations of purines following warm liver ischemia in man. Eur Surg Res 2005;37:144-152.
110 Choukèr A, Martignoni A, Schauer R, Dugas M, Rau HG, Jauch KW, et al. Bene fi cial effects of ischemic preconditioning in patients undergoing hepatectomy: the role of neutrophils. Arch Surg 2005;140:129-136.
111 Azoulay D, Lucidi V, Andreani P, Maggi U, Sebagh M, Ichai P, et al. Ischemic preconditioning for major liver resection under vascular exclusion of the liver preserving the caval fl ow: a randomized prospective study. J Am Coll Surg 2006;202:203-211.
112 Heizmann O, Loehe F, Volk A, Schauer RJ. Ischemic preconditioning improves postoperative outcome after liver resections: a randomized controlled study. Eur J Med Res 2008;13:79-86.
113 Bombuy E, Fondevila C, Rodriguez-Laiz G, Ferrer J, Amador A, Valentini M, et al. Ischemic preconditioning in adult living donor liver transplantation, a pilot study. J Hepatol 2004;40:S39.
114 Koneru B, Fisher A, He Y, Klein KM, Skurnick J, Wilson DJ, et al. Ischemic preconditioning in deceased donor liver transplantation: a prospective randomized clinical trial of safety and ef fi cacy. Liver Transpl 2005;11:196-202.
115 Azoulay D, Del Gaudio M, Andreani P, Ichai P, Sebag M, Adam R, et al. Effects of 10 minutes of ischemic preconditioning of the cadaveric liver on the graft's preservation and function: the ying and the yang. Ann Surg 2005;242:133-139.
116 Jassem W, Fuggle SV, Cerundolo L, Heaton ND, Rela M.Ischemic preconditioning of cadaver donor livers protects allografts following transplantation. Transplantation 2006;81:169-174.
117 Koneru B, Shareef A, Dikdan G, Desai K, Klein KM, Peng B, et al. The ischemic preconditioning paradox in deceased donor liver transplantation-evidence from a prospective randomized single blind clinical trial. Am J Transplant 2007;7:2788-2796.
118 Jassem W, Fuggle S, Thompson R, Arno M, Taylor J, Byrne J, et al. Effect of ischemic preconditioning on the genomic response to reperfusion injury in deceased donor liver transplantation. Liver Transpl 2009;15:1750-1765.
119 Casillas-Ramírez A, Mosbah IB, Ramalho F, Roselló-Catafau J, Peralta C. Past and future approaches to ischemiareperfusion lesion associated with liver transplantation. Life Sci 2006;79:1881-1894.
120 Jassem W, Koo DD, Cerundolo L, Rela M, Heaton ND,Fuggle SV. Leukocyte in fi ltration and in fl ammatory antigen expression in cadaveric and living-donor livers before transplant. Transplantation 2003;75:2001-2007.
121 Cescon M, Grazi GL, Grassi A, Ravaioli M, Vetrone G,Ercolani G, et al. Effect of ischemic preconditioning in whole liver transplantation from deceased donors. A pilot study. Liver Transpl 2006;12:628-635.
BACKGROUND: Liver transplantation is so far the most effective therapeutic modality for end-stage liver diseases,but ischemia/reperfusion (I/R) injury represents a critical barrier to liver transplantation. Primary graft dysfunction and small-for-size syndrome are closely associated with I/R injury. Ischemic preconditioning (IPC) is de fi ned as a brief period of liver ischemia followed by reperfusion, and has demonstrated protections against a prolonged I/R injury and improved the capacity of regeneration. The article aimed to review IPC literatures for the understanding of the effects of IPC on I/R injury involving in the procurement of donor liver and protective mechanisms.
DATA SOURCES: A literature search of MEDLINE and Web of Science databases using "liver transplantation", "liver regeneration", "hepatectomy", "ischemia/reperfusion" and"ischemic preconditioning" was performed, and then a large amount of related data was collected.
RESULTS: The literature search provided a huge amount of evidence for the protective effects of IPC on I/R injury in liver transplantation, including reduction of blood loss in hepatectomy, intraoperative hemodynamic stability and its signi fi cant role in liver regeneration. The mechanism involves in balancing in fl ammatory cytokines, enhancing energy status and mitigating microcirculatory disturbance.CONCLUSION: IPC plays an essential role in hepatectomy before and after harvest of living donor liver and implantation of liver graft.
Author Af fi liations: Key Laboratory of Combined Multi-organ Transplantation, Ministry of Public Health, First Af fi liated Hospital, Zhejiang University School of Medicine, Hangzhou 310003, China (Yan S, Jin LM,Liu YX, Zhou L, Xie HY and Zheng SS)
Shu-Sen Zheng, MD, PhD, FACS, Key Laboratory of Combined Multi-organ Transplantation, Ministry of Public Health, First Af fi liated Hospital, Zhejiang University School of Medicine, Hangzhou 310003, China (Tel: 86-571-87236567; Fax: 86-571-87236884; Email:shusenzheng@zju.edu.cn)
© 2010, Hepatobiliary Pancreat Dis Int. All rights reserved.
October 8, 2009
Accepted after revision April 23, 2010
杂志排行
Hepatobiliary & Pancreatic Diseases International的其它文章
- Pancreatic duct stones in patients with chronic pancreatitis: surgical outcomes
- Methylprednisolone inhibits activated CD4+ T cell survival promoted by toll-like receptor ligands
- Endoscopic management of postcholecystectomy biliary leakage
- Magnetic resonance imaging-guided percutaneous cryoablation of hepatocellular carcinoma in special regions
- Radiofrequency ablation, heat shock protein 70 and potential anti-tumor immunity in hepatic and pancreatic cancers: a minireview
- Endoscopic retrograde cholangiopancreatography outcome from a single referral center in Iran