Liver graft vascular variant with 3 extra-hepatic arteries
2010-07-05
New York, USA
Liver graft vascular variant with 3 extra-hepatic arteries
Paulo N Martins
New York, USA
Vascular anatomy of the liver is varied, and the "standard" anatomy is seen in 55%-80% of cases. It is very important that extrahepatic arteries are identified precisely at the time of graft procurement to avoid injuries that might compromise the liver function. In the present case the liver donor had the vascular anatomy of Michels type Ⅶ, e.g. a hepatic artery originating from the celiac trunk and going to the left lobe, an accessory left hepatic artery coming from the left gastric artery, and a replaced right hepatic artery coming from the superior mesenteric artery. This pattern of vascular supply is uncommon, representing less than 5% of cases. The replaced hepatic artery was reconstructed in the back-table with polypropylene suture 7.0 by connecting it to the stump of the splenic artery, and the celiac trunk of the graft was anastomosed to the recipient common hepatic artery.
liver transplantation; liver anatomy; vascular variations; right replaced artery; accessory artery
Introduction
The vascular anatomy of the liver is varied. The "normal" anatomy i.e. the common hepatic artery originating from the celiac trunk and branching close to the parenchyma into the left and right hepatic arteries is seen in 55%-80% of the cases.[1-4]It is important that extrahepatic arteries are identified precisely at the time of graft procurement to avoid injuries that might compromise the liver function.In 42% of cases of variant hepatic arterial anatomy a reconstruction was required before liver transplant.[5]
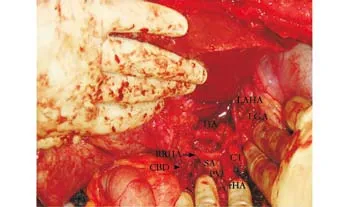
Fig. Liver graft vasculature with 3 extra-hepatic arteries. Hepatic artery (HA), left accessory hepatic artery (LAHA), left gastric artery stump (LGA), replaced right hepatic artery (RRHA, arrow showing the anastomosis), splenic artery (SA), celiac trunk (CT) common bile duct (CBD, arrow head), portal vein (PV), recipient common hepatic artery behind the finger (rHA).
Discussion
In our case (Fig.), the liver donor vascular anatomy was of Michels type Ⅶ, i.e., a hepatic artery originating from the celiac trunk and going to the left lobe, an accessory left hepatic artery originating from the left gastric artery, and a replaced right hepatic artery coming from the superior mesenteric artery (3 cm far from the origin of the superior mesenteric artery).[1]All branches supplying the liver were of similar diameter (>5 mm). This pattern of vascular supply is uncommon, specifically considering the large size of the variant arteries, and represents less than 5% of cases.[1-4]The replaced hepatic artery was shortened and reconstructed in the backtable with polypropylene suture 7.0 by connecting it to the stump of the splenic artery, and the celiac trunk of the graft was anastomosed to the recipient common hepatic artery. The left gastric artery stump was alsoligated (Fig.). The post-operative course of our case was unremarkable.
Funding: None.
Ethical approval: Informed consent was obtained from the patient.
Contributors: MPN wrote the whole article. MPN is the guarantor.
Competing interest: No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
1 Michels NA. Newer anatomy of the liver and its variant blood supply and collateral circulation. Am J Surg 1962;112:337-347.
2 Nelson TM, Pollak R, Jonasson O, Abcarian H. Anatomic variants of the celiac, superior mesenteric, and inferior mesenteric arteries and their clinical relevance. Clin Anat 1988;1:75-91.
3 Hiatt JR, Gabbay J, Busuttil RW. Surgical anatomy of the hepatic arteries in 1000 cases. Ann Surg 1994;220:50-52.
4 Covey AM, Brody LA, Maluccio MA, Getrajdman GI, Brown KT. Variant hepatic arterial anatomy revisited: digital subtraction angiography performed in 600 patients. Radiology 2002;224:542-547.
5 Melada E, Maggi U, Rossi G, Caccamo L, Gatti S, Paone G, et al. Back-table arterial reconstructions in liver transplantation: single-center experience. Transplant Proc 2005;37:2587-2588.
Received March 10, 2010
Accepted after revision April 5, 2010
A practical deed is more important than one dozen of programmes.
— Karl Marx
(Hepatobiliary Pancreat Dis Int 2010; 9: 319-320)
Author Affiliations: Department of Surgery, Division of Hepatobiliary Surgery and Transplantation, New York Medical College, New York, USA (Martins PN)
Paulo N Martins, MD, PhD, New York Medical College, Westchester Medical Center, Transplant Center, 95 Grassland Road, New York 10595, USA (Tel: +1 914-493-5930; Fax: +1 914-493-1097; Email: Paulo_Martins@nymc.edu)
© 2010, Hepatobiliary Pancreat Dis Int. All rights reserved.
杂志排行
Hepatobiliary & Pancreatic Diseases International的其它文章
- Gallbladder cancer with tumor thrombus in the superior vena cava
- Budd-Chiari syndrome secondary to caval recurrence of renal cell carcinoma
- A prospective study on radiofrequency ablation locally advanced pancreatic cancer
- An effective model for predicting acute kidney injury after liver transplantation
- Pancreas transplantation in the mouse
- Integrity of the pancreatic duct-acinar system in the pathogenesis of acute pancreatitis