Evaluation of surgical procedure selection based on intraoperative free portal pressure measurement in patients with portal hypertension
2010-07-05
Shanghai, China
Evaluation of surgical procedure selection based on intraoperative free portal pressure measurement in patients with portal hypertension
Yong-Wei Sun, Wei Chen, Meng Luo, Rong Hua, Wei Liu, Yan-Miao Huo, Zhi-Yong Wu and Hui Cao
Shanghai, China
BACKGROUND: Various surgical procedures can be used to treat liver cirrhosis and portal hypertension. How to select the most appropriate procedure for patients with portal hypertension has become a difficult problem. This study aimed to analyze the relationship between the value of intraoperative free portal pressure (FPP) and postoperative complications, and to explore the significance of intraoperative FPP measurement with respect to surgical procedure selection.
METHODS: The clinical data of 187 patients with portal hypertension who received pericardial devascularization and proximal splenorenal shunt combined with devascularization (combined operation) at the Department of General Surgery in our hospital from January 2001 to September 2008 were retrospectively analyzed. Among the patients who received pericardial devascularization, those with a postoperative FPP≥22 mmHg were included in a high-pressure group (n=68), and those with FPP <22 mmHg were in a low-pressure group (n=49). Seventy patients who received the combined operation comprised a combined group. The intraoperative FPP measurement changes at different times, and the incidence of postoperative complications in the three groups of patients were compared.
RESULTS: The postoperative FPP value in the high-pressure group was 27.5±2.3 mmHg, which was significantly higher than that of the low-pressure (20.9±1.8 mmHg) or combined groups (21.7±2.5 mmHg). The rebleeding rate in the high-pressure group was significantly higher than that in the low-pressure and combined groups. The incidence rates of postoperative hepatic encephalopathy and liver failure were not statistically different among the three groups. The mortality due to rebleeding in the low-pressure and combined groups (0.84%) was significantly lower than that of the high-pressure group.
CONCLUSIONS: The study demonstrates that FPP is a critical measurement for surgical procedure selection in patients with portal hypertension. A FPP value ≥22 mmHg after splenectomy and devascularization alone is an important indicator that an additional proximal splenorenal shunt needs to be performed.
(Hepatobiliary Pancreat Dis Int 2010; 9: 269-274)
hypertension, portal; hemodynamics; devascularization; splenorenal shunt, surgical
Introduction
Portal hypertension is the most common complication of cirrhosis accounting for significant morbidity and mortality mainly because of variceal hemorrhage, ascites, bacterial infection, hepatic encephalopathy, and hepatorenal syndrome.[1]Its surgical treatment has mainly focused on the esophageal and gastric fundus varicose rupture hemorrhage caused by portal hypertension. The application of a simple shunt has been very rare because the shunt has potentially serious shortcomings such as higher incidence of hepatic encephalopathy and liver failure.[2]Although the surgical procedure for devascularization is relatively simple, the postoperative rebleeding rate is as high as 11% to 21.1%.[3-5]The hemostatic effect of a proximal splenorenal shunt combined with devascularization is satisfactory,[6]but the procedure is relatively complex, the technical requirement of the surgery is high, and the operation time is relatively long.
Hyperdynamic circulation plays a critical role in the development and maintenance of portal hypertension. It is not only the main pathophysiological change in patients with portal hypertension, but also the initiating event of variceal bleeding.[7]The most prominent hemodynamic manifestation of portal hypertension is increased portal vein pressure, whichis the major factor that causes esophageal and gastric fundus varicosis. Preoperative hemodynamic research methods include Doppler ultrasound, endoscopy, magnetic resonance portal venography (MRPVG), and transarterial portography,[8]but none of these methods measure portal pressure directly. The direct measurement of intraoperative free portal pressure (FPP) is the most reliable method reflecting the actual portal pressure, and is an objective and quantitative indicator. It is generally believed in China that when the portal pressure is ≥22 mmHg (30 cmH2O), rupture and hemorrhage of the varicose veins may occur.[9]With the in-depth research into portal hypertension that has already occurred, many recognize that the ideal surgical procedure for the treatment of portal hypertension with rupture or hemorrhage of varicosis of the esophagus and fundus of the stomach should be able to reduce the portal pressure effectively and maintain portal blood flow to the liver while also protecting liver function to the maximum extent. Therefore, both intraoperative FPP measurement and preoperative hemodynamic assessment play an important role in the reasonable selection of surgical procedure and the improvement of surgical treatment effects.
Currently, clinical reports are very few on selecting the appropriate surgical procedure based on direct measurement of intraoperative FPP changes. Therefore, we summarized the clinical data of patients with portal hypertension who received pericardial devascularization and the combined operation in our hospital during the past eight years. We analyzed the relationship between the intraoperative FPP values and postoperative rebleeding, hepatic encephalopathy, liver failure, and mortality, and explored the guiding significance of intraoperative FPP measurement and its relationship to surgical procedure selection.
Methods
General information
The clinical data were collected from 187 patients with portal hypertension who received a pericardial devascularization operation (the devascularization group) and proximal splenorenal shunt combined with pericardial devascularization (the combined group) at the Department of General Surgery of Renji Hospital from January 2001 to September 2008. Among them, 118 were male and 69 were female. Their median age was 53 years (38-75). There were 174 patients with liver cirrhosis due to hepatitis B, 10 with liver cirrhosis due to schistosomiasis, and 3 with alcoholic cirrhosis. According to the Child-Pugh classification, 79 patients were of class A, 92 class B and 16 class C. Preoperative hematemesis and (or) black stool occurred in 165 patients. Before the surgery, all patients were confirmed to have medium to severe esophageal and gastric varices by gastroscopy or upper gastrointestinal barium meal examination.
Research methods
Selective surgery was scheduled for the patients. After opening the abdominal cavity, the presence of varices, degree of liver cirrhosis, and ascites volume were ascertained. After exploration, the gastrocolic ligament was cut off along the transverse colon and the portal pressure measurement tube was placed. Then the splenic artery trunk was found on the upper edge of the pancreatic body and a double ligation was performed. The devascularization aimed to: 1) ligate and cut off the left-side of the hepatogastric and gastrocolic ligaments, and the arteries and veins in the splenogastric ligament, 2) cut off the branches of the left gastric artery and the gastric branch, and the esophageal branch of the gastric coronary vein, and 3) cut off and ligate the varicose veins around the cardia and in the abdominal esophagus 6 to 8 cm below the level of the esophageal hiatus (including allotopia or perch rami oesophagei). A splenorenal end-to-side shunt was performed after the splenectomy in the combined group. Usually the splenic vein stump was used for anastomosis with the left renal vein. If the diameter of the splenic vein was too large, the anastomotic stoma was appropriately decreased so that it could be controlled within 0.8-1.2 cm. The devascularization was performed after completion of the splenorenal vein anastomosis.
The FPP value was measured during the operation. To analyze the relationship between the FPP values and postoperative complications, we divided the patients into three groups: a high-pressure group with a postoperative FPP ≥22 mmHg after devascularization, a low-pressure group with a postoperative FPP <22 mmHg after devascularization, and a combined group with a shunt plus devascularization. The preoperative liver function indicators and the Child-Pugh classification of the three groups of patients were compared.
The postoperative complications refer to rebleeding, encephalopathy, liver failure, and death. Postoperative rebleeding refers to hematemesis or hematochezia-black stool detected by an occult blood test (++) two or more weeks after surgery. Portal hypertensive gastropathy (PHG) is defined as follows: the disease is called PHG when the gastric mucosa of portal hypertension patients shows pathological changes in mucous membranes andsubmucosal vessel dilation under a gastroscope without histological inflammation. When mucous erosion is found to be extensive and serious, or either diffuse bleeding or acute ulcer formation exists in combination with bleeding, then PHG should be considered as the cause of the bleeding.[10,11]Postoperative encephalopathy is defined as the manifestation of personality and behavior disorders. Patients seriously affected may have confusion, sleep disorders, loss of orientation, and decreased comprehension. Drowsiness and mental disorders, or even loss of consciousness and coma may occur in patients with serious conditions.[12]Liver failure is defined as serious liver damage after operation, resulting in serious disorders or decompensation of liver functions including synthesis, detoxification, excretion, and biotransformation, and causing a group of clinical symptoms with major manifestations of clotting disorder, jaundice, hepatic encephalopathy, and ascites. The diagnostic criteria for liver failure have been elucidated in the position paper of the American Association for the Study of Liver Disease (AASLD), and the diagnostic and treatment guidelines of the Chinese Society of Hepatology.[13,14]The deaths of patients due to postoperative complications or diseases caused by liver dysfunction were included in this study in the mortality statistics.
The postoperative follow-up rates for the highpressure, low-pressure, and combined groups were 83%, 75%, and 78%, respectively. All 187 patients were followed for an average of 48 months (range 6-86). The average follow-up duration for the high-pressure, lowpressure, and combined groups was 50, 45, and 46 months, respectively.
Measurement of intraoperative FPP
After opening the abdominal cavity, the gastrocolic ligament was cut off along the transverse colon. A 0.3 cm diameter silica tube was selected and inserted from the right branch of the midcolonic vein in the anterior mesocolon transversum into the portal vein via the superior mesenteric vein (about 15 cm long) and was fixed. Its end was connected to a transducer (Biosensors International, Singapore) and the FPP values were read directly and consecutively using a multi-function monitor (Hewlett-Packard, USA). The FPP values were recorded at 5 time points: when the abdominal cavity was opened, the splenic artery was ligated, the splenectomy was completed, the shunt was finished, and the devascularization was completed. Patients were in the supine position, and the zero point was set at a level 1 cm above the first lumbar vertebra (approximately at the start of the portal vein).[15,16]
Statistical analysis
The data were analyzed using the SPSS 11.0 statistical software package. The results are shown as mean±SD. The statistical analyses included variance analysis, nonpairedttest and the Chi-square test. Statistical values ofP<0.05 were considered to be significant.
Results
Preoperative liver function
There were no significant differences in liver function (serum albumin, serum total bilirubin and prothrombin time) or the Child-Pugh classification between the highpressure, low-pressure, and combined groups.
Dynamic changes of intraoperative FPP values in the three groups of patients
The dynamic changes of the intraoperative FPP in the three groups of patients are shown in Table 1. After opening the abdominal cavity, there was no significant difference in the FPP among the three groups. The FPP in all groups decreased significantly after the splenic artery ligation compared with the value when the abdominal cavity was opened. The FPP decreased by an average of 4.1 mmHg (13.9%), 7.6 mmHg (26.6%), and 5.9 mmHg (20.0%) in the high-pressure, low-pressure, and combined groups, respectively. Changes in the FPP were not evident in the three groups after the splenectomy. Compared with the value after splenectomy, the FPP in the high-pressure group increased an average of 2.7 mmHg after devascularization, reaching 27.5 mmHg. There was no difference in FPP values from those after the abdominal cavity was opened, while the value in the low-pressure group did not change significantly. The FPP of the combined group decreased to 18.2 mmHg after completion of the shunt and increased from 3.5 mmHg to 21.7 mmHg after devascularization. That value was significantly lower than that found after opening the abdominal cavity and the value after devascularization in the high-pressure group, but it was not significantly different from the value after devascularization in the low-pressure group.

Table 1. Dynamic changes of intraoperative FPP in the three groups at different times (mmHg, mean±SD)
Postoperative complications
A total of 18 patients had rebleeding in the devascularization group giving a rebleeding rate of 15.4% (18/117) (Table 2). The rebleeding rate in the high-pressure group was 22.1%, which was significantly higher than that of the low-pressure group (6.1%) and the combined group (4.3%). The average rebleeding time was 33.6 months after surgery in the high-pressure group. Gastroscopic examination showed that this was caused by the reappearance of esophageal and gastric varices in 8 patients, by PHG in 5, and by unknown reasons in 2 in the high-pressure group. Rebleeding occurred at an average of 26.8 months after surgery in the low-pressure group. This was caused by the reappearance of esophageal and gastric varices in one patient and by unknown reasons in 2. Three patients in the combined group had rebleeding one year after surgery. MRPVG examination after hemorrhage controlshowed thrombosis at the splenorenal anastomotic stoma and reformation of esophageal and gastric varices.
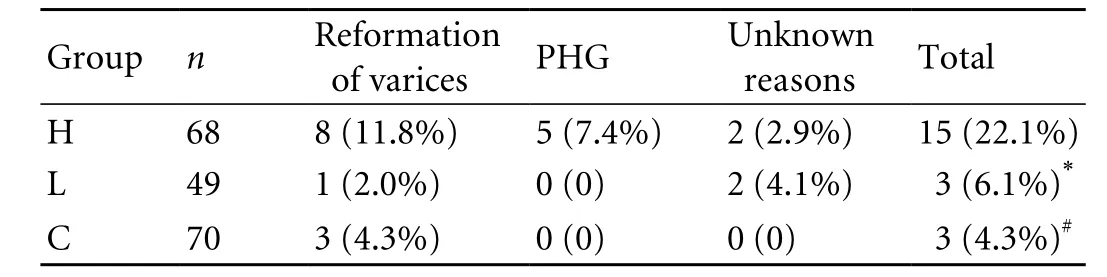
Table 2. Analysis of the causes of postoperative rebleeding in the three groups
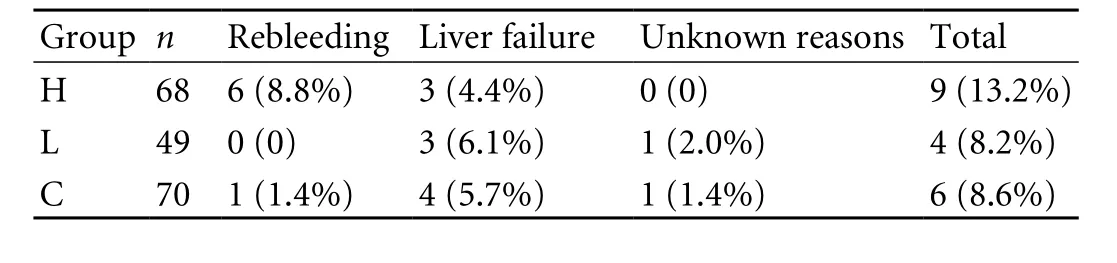
Table 3. Analysis of causes of postoperative death in the three groups
The numbers and incidence rates of postoperative encephalopathy were 2 (2.9%), 3 (6.1%), and 7 (10.0%) in the high-pressure, low-pressure, and combined groups, respectively, but there were no significant differences. All the patients with encephalopathy in the combined group were controlled, except one patient with repeated coma after the shunt and a fracture of the femur, who was cured by ligation of the anastomotic stoma at last. Most symptoms of encephalopathy disappeared within six months to one year after medication including dietary regulation and drug treatment, which did not cause any serious clinical problems.
Three patients each in the high-pressure and lowpressure groups experienced liver failure. Among them, 5 had the failure two years after the surgery, and 1 in the high-pressure group had the failure one year after surgery because of rebleeding on the end-to-side mesocaval shunt. Four patients in the combined group experienced liver failure in the period of follow-up. There was no significant difference in the incidence rate of liver failure among the three groups. All the patients who experienced liver failure did not respond to liver protection treatment and died.
There were 9 deaths in the high-pressure group (13.2%), of which 6 were due to postoperative rebleeding, and 3 due to liver failure (Table 3). In 4 deaths (8.2%) in the low-pressure group, 3 were attributable to liver failure, and 1 was ascribed to unknown reasons. Six deaths (8.6%) in the combined group were due to postoperative rebleeding (1), liver failure (4), and unknown reasons (1). There was no significant difference in the mortality rate among the three groups. However, only one death in the 119 patients of the low-pressure and combined groups was caused by postoperative rebleeding, with an incidence rate of only 0.84%, which was lower than that of the high-pressure group (χ2=5.60,P<0.05).
Discussion
Pericardial devascularization is a commonly used surgical method for the treatment of portal hypertension, but the incidence of postoperative rebleeding is still high.[17-19]The reason may be related to re-emergence of the collateral circulation of the portal system due to the continuous portal hypertension status after devascularization, and the reoccurrence of hemorrhage caused by rupture of esophageal and gastric varices and PHG.[20]The results of the present study show that to a large extent, the level of portal pressure afterdevascularization determines whether postoperative rebleeding will occur. The risk of rebleeding in our patients with a FPP ≥22 mmHg after devascularization was significantly higher than that in patients with a FPP <22 mmHg. Therefore, no matter which surgical procedure is adopted, the goal of surgery is to decrease the FPP to less than 22 mmHg. In our study, the FPP decreased by an average of 4.8 mmHg after the splenorenal shunt, and increased after devascularization, indicating that devascularization can force some blood to enter the collateral circulation of the portal vein and flow to the liver, maintaining a certain amount of portal blood flow to the liver. Therefore, although the incidence rate of postoperative hepatic encephalopathy in the combined group (10%) was higher than that of the low-pressure group (6.1%) and the high-pressure group (2.9%), there were no significant differences. In addition, compared with the patients of the other two groups, the symptoms of patients with postoperative encephalopathy in the combined group were easily controlled and did not cause serious problems, and they were gradually alleviated and finally disappeared within six months to one year after surgery. This may be related to the gradual tolerance of the liver to decreased portal blood flow or a compensatory increase of arterial blood. In fact, the symptoms of encephalopathy were easier to control in the combined group than in the highpressure or low-pressure groups. The portosystemic shunt indicated why encephalopathy symptom control was easier in the former group, and lack of symptom control in the latter two may have been caused by the deterioration of liver function itself.
The results of the present study showed that the effects of conservative treatment were not good for patients with liver cirrhosis and portal hypertension who experienced liver failure, and all these patients eventually died except those who underwent liver transplantation. Follow-up revealed that the main causes of death in the high-pressure group were postoperative rebleeding and liver failure; the main cause in the low-pressure and combined groups was liver failure, rebleeding being rare. No significant differences in the incidence rate of postoperative liver failure among the three groups suggest that the combined operation can maintain a certain amount of blood perfusion to the liver and does not additionally influence liver function compared with devascularization. The postoperative mortality was 13.2%, 8.2% and 8.6% in the high-pressure, low-pressure, and combined groups, respectively, with no significant difference. Therefore, the combined operation did not cause the increase of mortality because of the increase of operation time and surgical trauma. However, only one patient died from postoperative rebleeding in the low-pressure and combined groups, and the incidence rate was significantly different from that of the high-pressure group. It is clear that the selection of an appropriate surgical procedure based on the results of intraoperative FPP changes can significantly decrease the postoperative mortality due to rebleeding.
The operation sequence of devascularization and shunt is different in different reports, with some operators performing the shunt first and then the devascularization. Some operators perform splenectomy and devascularization before the shunt. If the FPP value is used as a reference for surgical procedure selection, the devascularization should be performed before the shunt. But in fact, the FPP decrease after splenic artery ligation is the clearest indication of the pressure decrease during the entire surgical process (Table 2). If the FPP cannot be decreased to be within the bleeding threshold after the splenic artery ligation, especially when the value remains unchanged or even increases after splenectomy, or if the splenic vein tension remains high, an additional shunt should be performed. That is why the latter operation will not decrease the portal pressure; rather, it may increase the portal pressure slightly. Usually, an additional splenorenal shunt is a reasonable option. The pressure-decreasing effects of that surgery are satisfactory, and not only can relieve the rupture and hemorrhage of the varicosis and bleeding caused by PHG, but also can prevent splenic vein thrombosis and possible spread to the portal vein after the splenectomy and devascularization. In practice, we usually perform the shunt before additional devascularization, the advantage of which is that the dissociation of the splenic vein is relatively simple when the spleen is present, and devascularization after the shunt and the pressure decrease is relatively easy. If the sequence is reversed, sometimes the duration of the devascularization operation is relatively long, and clamping of the splenic vein stump can easily cause splenic vein thrombosis. Recently, for those patients whose need for a shunt could not be accurately estimated after the completion of splenectomy, we determined the necessity of an additional shunt according to the FPP value after devascularization and splenic vein tension.
The hemodynamics of portal hypertension is very complex. As reflected in clinical practice, the surgical procedures are numerous. However, hemodynamic research is attracting more and more attention to the treatment of portal hypertension, particularly in the selection of surgical procedure. We chose FPP as the indicating parameter for selection of the surgicalprocedure. If the FPP decreases greatly after splenic artery ligation and the value is below the bleeding threshold (22 mmHg) after devascularization, the surgery can be finished. Otherwise, an additional shunt needs to be performed. This not only reduces the high rebleeding rate caused by an unchanged high portal pressure after devascularization, but also prevents unnecessary surgical trauma and risk. It may be used as a simple method to determine the surgical procedure. If more in-depth and extensive research can be conducted to determine the relationship between the FPP threshold and other hemodynamic indicators and their significance for surgical procedure selection, a more scientific method can be found in accordance with the pathological and physiological changes of the patients, and thereby the best therapeutic effects will be achieved.
Funding: None.
Ethical approval: Not needed.
Contributors: SYW proposed the study and wrote the first draft. CW analyzed the data. All authors contributed to design and interpretation of the study and to further drafts. CH is the guarantor.
Competing interest: No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
1 Cárdenas A, Ginès P. Portal hypertension. Curr Opin Gastroenterol 2009;25:195-201.
2 Zhou GW, Li HW. Surgical therapy for portal hypertension in patients with cirrhosis in China: present situation and prospects. Chin Med J (Engl) 2009;122:1483-1485.
3 Xu XB, Cai JX, Leng XS, Dong JH, Zhu JY, He ZP, et al. Clinical analysis of surgical treatment of portal hypertension. World J Gastroenterol 2005;11:4552-4559.
4 Burak KW, Lee SS, Beck PL. Portal hypertensive gastropathy and gastric antral vascular ectasia (GAVE) syndrome. Gut 2001;49:866-872.
5 Liu B, Lin N, Xu RY. Splenectomy combined with endoscopic variceal ligation in treating portal hypertension. Zhong Nan Da Xue Xue Bao Yi Xue Ban 2004;29:87-89.
6 Cao H, Hua R, Wu ZY. Effects of combined splenorenal shunt devascularization and devascularization only on hemodynamics of the portal venous system in patients with portal hypertension. Hepatobiliary Pancreat Dis Int 2005;4: 385-388.
7 Wu ZY. Hemodynamic study of portal hypertension. Hepatobiliary Pancreat Dis Int 2007;6:457-458.
8 Liu H, Cao H, Wu ZY. Magnetic resonance angiography in the management of patients with portal hypertension. Hepatobiliary Pancreat Dis Int 2005;4:239-243.
9 Hua R, Wu ZY, Sun YW, Qiu JF, Luo M, Xu Q, et al. A study on the relationship post-devascularization portal pressure and rebleeding in portal hypertensive patients. Zhonghua Pu Tong Wai Ke Za Zhi 2007;3:194-196.
10 Primignani M, Carpinelli L, Preatoni P, Battaglia G, Carta A, Prada A, et al. Natural history of portal hypertensive gastropathy in patients with liver cirrhosis. The New Italian Endoscopic Club for the study and treatment of esophageal varices (NIEC). Gastroenterology 2000;119:181-187.
11 Xu R, Ling Y, Qiu W. The different influences of splenectomy plus ligation of pericardial vein and shunt on portal hypertensive gastropathy. Zhonghua Wai Ke Za Zhi 1997;35: 515-517.
12 Mullen KD. Review of the final report of the 1998 Working Party on definition, nomenclature and diagnosis of hepatic encephalopathy. Aliment Pharmacol Ther 2007;25:11-16.
13 Polson J, Lee WM; American Association for the Study of Liver Disease. AASLD position paper: the management of acute liver failure. Hepatology 2005;41:1179-1197.
14 Liver Failure and Artificial Liver Group, Chinese Society of Infectious Diseases, Chinese Medical Association; Severe Liver Diseases and Artificial Liver Group, Chinese Society of Hepatology, Chinese Medical Association. Diagnostic and treatment guidelines for liver failure. Zhonghua Gan Zang Bing Za Zhi 2006;14:643-646.
15 Groszmann R, Vorobioff JD, Gao H. Measurement of portal pressure: when, how, and why to do it. Clin Liver Dis 2006; 10:499-512, viii.
16 Bosch J, Garcia-Pagán JC, Berzigotti A, Abraldes JG. Measurement of portal pressure and its role in the management of chronic liver disease. Semin Liver Dis 2006; 26:348-362.
17 Lee SW, Lee TY, Chang CS. Independent factors associated with recurrent bleeding in cirrhotic patients with esophageal variceal hemorrhage. Dig Dis Sci 2009;54:1128-1134.
18 Elwood DR, Pomposelli JJ, Pomfret EA, Lewis WD, Jenkins RL. Distal splenorenal shunt: preferred treatment for recurrent variceal hemorrhage in the patient with wellcompensated cirrhosis. Arch Surg 2006;141:385-388.
19 Turnes J, García-Pagán JC, González M, Aracil C, Calleja JL, Ripoll C, et al. Portal hypertension-related complications after acute portal vein thrombosis: impact of early anticoagulation. Clin Gastroenterol Hepatol 2008;6:1412-1417.
20 Zhang Y, Wen T, Yan L, Chen Z, Yang H, Deng X, et al. The changes of hepatic hemodynamics and functional hepatic reserve after splenectomy with periesophagogastric devascularization. Hepatogastroenterology 2009;56:835-839.
Received December 29, 2009
Accepted after revision April 2, 2010
Author Affiliations: Department of General Surgery, Renji Hospital, Shanghai Jiaotong University School of Medicine, Shanghai 200127, China (Sun YW, Chen W, Luo M, Hua R, Liu W, Huo YM, Wu ZY and Cao H)
Hui Cao, MD, PhD, Department of General Surgery, Renji Hospital, Shanghai Jiaotong University School of Medicine, Shanghai 200127, China (Tel: 86-21-68383751; Email: caohuishcn@ hotmail.com)
© 2010, Hepatobiliary Pancreat Dis Int. All rights reserved.
杂志排行
Hepatobiliary & Pancreatic Diseases International的其它文章
- Gallbladder cancer with tumor thrombus in the superior vena cava
- Budd-Chiari syndrome secondary to caval recurrence of renal cell carcinoma
- A prospective study on radiofrequency ablation locally advanced pancreatic cancer
- Liver graft vascular variant with 3 extra-hepatic arteries
- An effective model for predicting acute kidney injury after liver transplantation
- Pancreas transplantation in the mouse