131I治疗对甲状腺乳头状癌全切术后患者涎腺的影响:基于超声剪切波弹性成像
2024-10-30薛梦华李婷婷薛继平周林燕王丹李海康王瑞琪冯婷华

摘要:目的" 探讨实时剪切波弹性成像(SWE)技术在接受碘放射性同位素(131I)治疗后的甲状腺乳头状癌(PTC)全切术后患者腮腺、颌下腺病变的临床应用价值。方法" 选取2022年9月~2023年11月于山西白求恩医院核医学科门诊复诊的60例接受131I治疗1年以上有口干症状的PTC全切术后患者作为治疗组,另选取同期本院年龄性别相匹配的30例健康志愿者作为对照组。应用Supersonic Aixplorer超声诊断仪对所有受试者双侧腮腺及颌下腺进行常规超声及SWE检查。分别测量对照组、治疗组腮腺厚度、颌下腺体积及其杨氏模量平均值(Emean)。结果" 两组腮腺厚度与颌下腺体积的差异无统计学意义(Pgt;0.05);对照组及治疗组腮腺、颌下腺Emean值分别为:8.56±0.71、8.41±1.00 kPa及13.25±2.98、11.92±2.06 kPa,组间相同部位两两比较差异有统计学意义(Plt;0.001);组内不同部位比较,治疗组腮腺Emean大于颌下腺Emean(Plt;0.05),对照组腮腺、颌下腺Emean的差异无统计学意义(Pgt;0.05);所有受试者腮腺和颌下腺Emean双侧比较差异均无统计学意义(Pgt;0.05);腮腺Emean、颌下腺Emean均与随访时间、累计用药剂量及用药频次呈线性相关(Plt;0.001);多元线性回归分析提示,累计用药剂量均与腮腺Emean、颌下腺Emean呈独立正相关(Plt;0.001)。结论" SWE作为一种无创、无辐射、简便、可重复的检查方法,可定量评估经131I治疗的PTC全切术后患者的腮腺和颌下腺的硬度。累计用药剂量越大,腮腺及颌下腺Emean值越高,组织硬度越大,组织受损程度可能越大。SWE可能为临床评估经131I治疗的PTC全切术后患者的腮腺、颌下腺的组织损伤提供定量监测参考指标。
关键词:碘放射性同位素;甲状腺乳头状癌;剪切波弹性成像;腮腺;颌下腺
Assessing salivary gland hardness in postoperative papillary thyroid cancer patients after 131I treatment: a study based on shear wave elastography
XUE Menghua, LI Tingting, XUE Jiping, ZHOU Linyan, WANG Dan, LI Haikang, WANG Ruiqi, FENG Tinghua
Department of Ultrasound, Shanxi Bethune Hospital (Shanxi Academy of Medical Sciences), Third Hospital of Shanxi Medical University, Tongji Shanxi Hospital, Taiyuan 030032, China
Abstract: Objective To preliminarily investigate the clinical application value of real‑time shear wave elastography (SWE) technology in parotid and submandibular gland lesions in post-total resection patients with papillary thyroid carcinoma (PTC) after receiving iodine radioisotope (131I) therapy. Methods Sixty postoperative PTC patients who underwent total thyroidectomy and experienced dry mouth symptoms after receiving 131I therapy for over 1 year during their follow‑up visits at outpatient clinic of Department of Nuclear Medicine, Shanxi Bethune Hospital from September 2022 to November 2023 were included as treatment group. Control group was formed by selecting 30 healthy volunteers with matching age and gender from our hospital during the same period. Supersonic Aixplorer ultrasonic diagnostic instrument was applied to perform routine ultrasound and SWE examination of bilateral parotid and submandibular glands of all subjects. The parotid gland thickness, submandibular gland volume and its mean Young's modulus (Emean) were measured in the control and treatment groups, respectively. Results There was no significant difference in the thickness of parotid gland and the volume of submandibular gland between the group(Pgt;0.05). The Emean values of the parotid and submandibular glands in the control group were 8.56±0.71 and 8.41±1.00 kPa, respectively, while in the treatment group they were 13.25±2.98 and 11.92±2.06 kPa, respectively; There were significant differences in the same parts between the two groups (Plt;0.001); When comparing different locations within groups, the treatment group had a higher Emean value in the parotid gland compared to the submandibular gland (Plt;0.05), while there was no statistically significant difference in Emean values between the parotid and submandibular glands in the control group (Pgt;0.05). There was also no statistically significant difference in bilateral comparison of Emean values for both glands among all subjects (Pgt;0.05). The Emean of parotid gland and submandibular gland was found to have a linear correlation with the follow‑up duration, cumulative dose, and drug administration frequency (Plt;0.001). Multiple linear regression analysis showed that the cumulative dose was independently and positively correlated with Emean of parotid gland and submandibular gland (Plt;0.001). Conclusion As a non‑invasive, radiation‑free, straightforward, and replicable examination, SWE can offer quantitative evaluations of the hardness of parotid and submandibular glands in patients who have undergone total resection of PTC and subsequently undergone therapy with 131I. An increase in the cumulative dose results in higher Emean values for both parotid and submandibular glands, indicative of increased tissue hardness, and potentially, a greater extent of tissue damage. SWE may serve as a valuable index in the clinical appraisal of tissue damage in the parotid and submandibular glands of patients following total PTC resection and 131I treatment, providing a quantitative means for monitoring.
Keywords: iodine radioisotope; papillary thyroid carcinoma; shear wave elastography; parotid gland; submandibular gland
甲状腺乳头状癌(PTC)是最常见的甲状腺恶性肿瘤,碘放射性同位素(131I)治疗是甲状腺癌全切术后综合治疗的主要措施之一,能有效去除甲状腺癌术后残余甲状腺组织和可能存在的残留或转移病灶,降低PTC复发率及死亡率,但同时也会引起涎腺的损伤,其发生率为18.7%~64.7%[1-4],临床表现为涎腺肿胀、疼痛及口干等症状。故临床治疗应以预防为主[5, 6],定期评估腮腺及颌下腺的组织受损情况尤为重要。既往有研究通过常规超声及唾液腺核素显像观察PTC患者131I治疗后涎腺的大小、回声、血供、摄取和分泌功能等判断唾液腺的损伤程度,并发现131I治疗后涎腺损伤的发生率和损伤程度与131I剂量相关[7-9]。但常规超声无法定量判断早期涎腺损伤;唾液腺核素现象具有放射性,可重复性低,限制了临床对涎腺损伤的定期随访观察。剪切波弹性成像(SWE)是通过非侵入性测量杨氏模量值来定量评价组织硬度的一种超声新技术,具有实时、定量、无辐射及重复性好的优点。已有研究者应用SWE技术评估正常成人涎腺弹性模量值及干燥综合征患者涎腺硬度[10-13];近年来也有研究者评价了SWE技术在头颈部肿瘤放疗后涎腺损伤的应用价值[14-17]。但SWE在评估经131I治疗PTC全切术后患者的涎腺损伤的硬度变化的相关研究极少。本研究是初步应用SWE技术评估经131I治疗的PTC全切术后患者的腮腺和颌下腺组织硬度变化信息,并分析杨氏模量值与累计用药剂量之间的相关性,以期SWE对临床诊断涎腺损伤提供一定的参考价值。
1" 资料与方法
1.1" 一般资料
收集2022年9月~2023年11月在山西白求恩医院核医学科门诊复诊的PTC全切术后并接受131I治疗后1年以上且有口干症状的患者60例,其中男性23例,女性37例,年龄23~68(44.97±12.06)岁。纳入标准:PTC全切术后;接受131I治疗1年以上(所有患者131I治疗后均服用维生素C 3 d);有口干症状;由耳鼻喉专家确诊的口腔黏膜干燥。排除标准:干燥综合征;涎腺炎、涎石症及涎腺肿瘤;头颈部放疗病史;糖尿病;图像质量差。另收集年龄、性别相匹配的健康志愿者30例,其中男性12例,女性18例,年龄21~58(40.80±10.79)岁。本研究已获得山西白求恩医院伦理委员会的批准(审批号:YXLL-2020-030),所有受试者均知情研究内容并签署知情同意书。
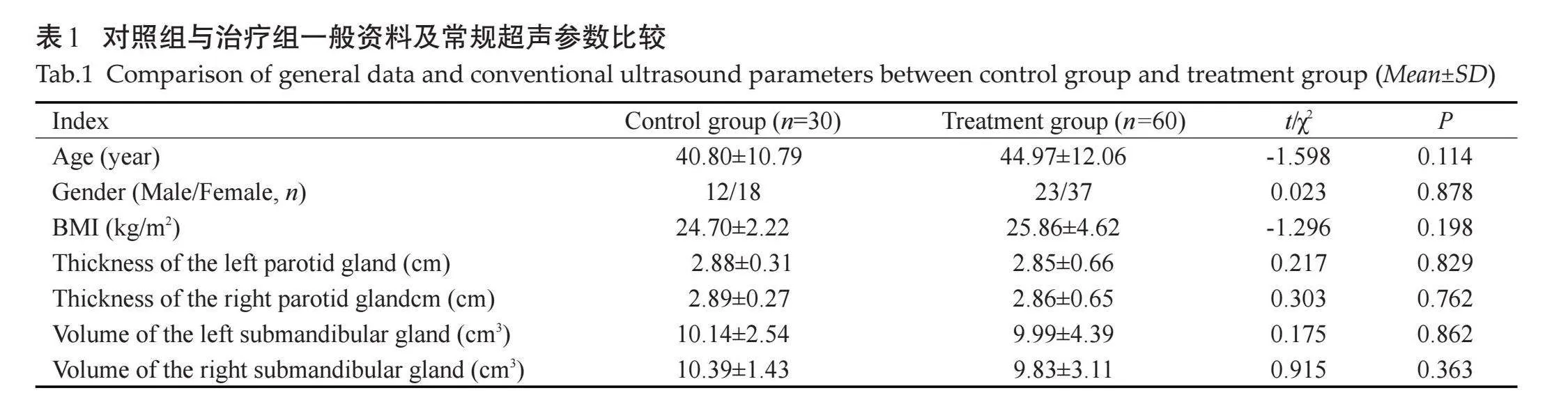
治疗组中接受131I治疗的平均剂量为202.25[±]85.13 mCi(100~400 mCi),34例接受1次131I治疗,25例接受2次131I治疗,1例接受3次131I治疗。随访时间(首次接受131I治疗到首次图像采集的时间)12~76(27.41±17.25)月。对照组与治疗组年龄、性别、BMI的差异均无统计学意义(Pgt;0.05)。治疗组腮腺厚度及颌下腺体积与对照组比较,差异无统计学意义(Pgt;0.05,表1)。
1.2" 仪器与方法
1.2.1" 仪器" "使用Supersonic Image Aix Plorer 型全数字化彩色多普勒超声诊断仪,L5~4线阵探头,频率4~15 MHz,SC6-1凸阵探头,频率1~6 MHz。
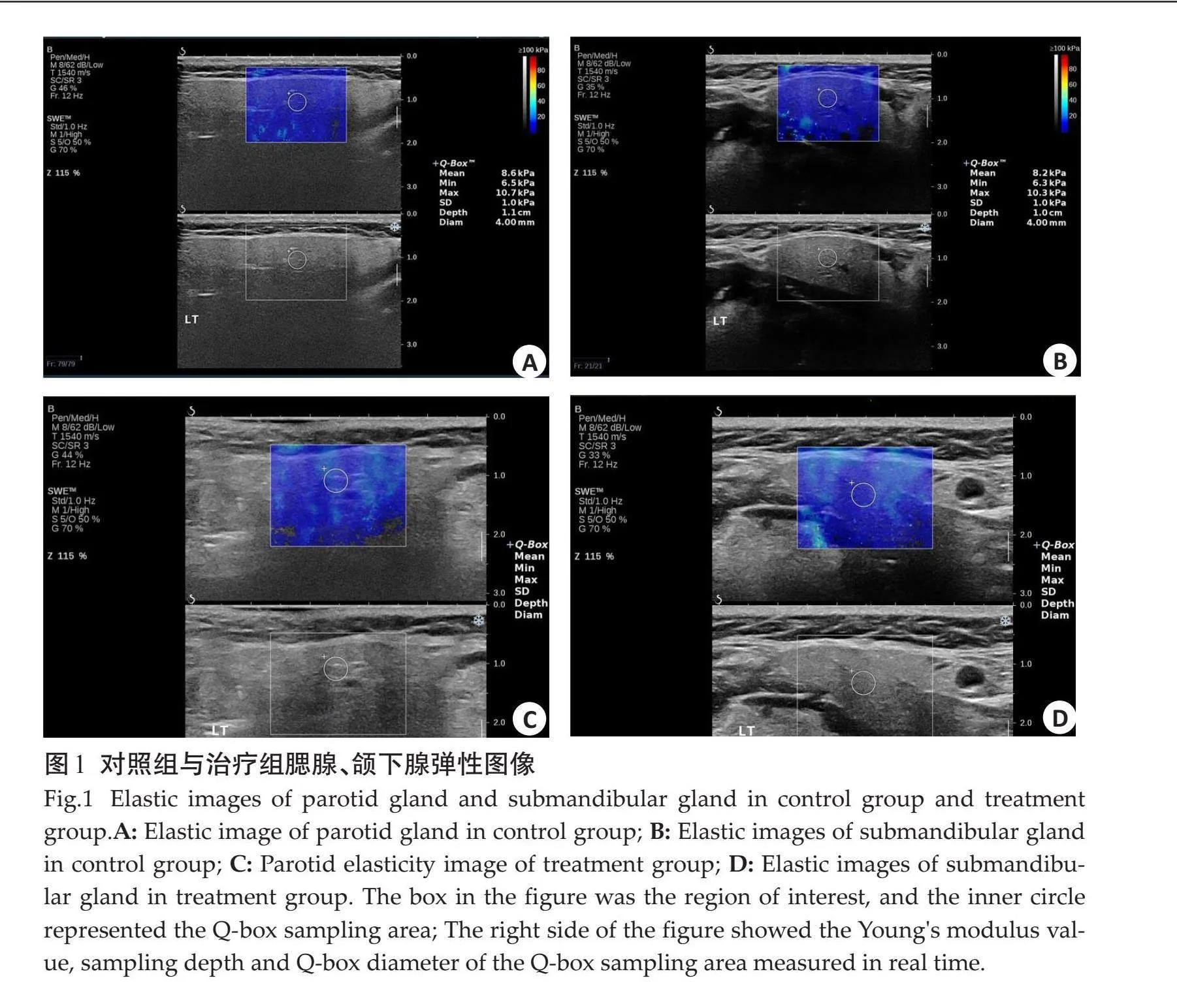
1.2.2" 图像采集及分析" "常规超声和弹性成像检查由1位有5年工作经验的超声科医生进行。所有受试者取仰卧位,充分暴露检查区域,头部略转向对侧,避免过度仰伸颈部,嘱受试者平静呼吸,充分放松颈部及面部肌肉,避免吞咽活动。首先用二维超声SC6-1凸阵探头测量腮腺厚度,后用L5-4探头观察腮腺及颌下腺形态、回声,测量颌下腺体积(颌下腺体积=内外径×前后径×上下经×0.52)[18],随即选择SWE模式,将探头轻放且垂直皮肤表面,避免施力加压,将感兴趣区取样框(取样框放置于腺体中央,大小约1 cm×1 cm)内颜色完全充填并稳定3 s后定帧进行测量。Q-Box置于取样框内,避开明显血管,Q-box直径约4 mm,分别测量双侧腮腺及颌下腺中部的杨氏模量平均值(Emean)(图1),每部位连续测量3次,记录并计算平均值。
1.3" 统计学分析
应用SPSS25.0软件进行统计分析,计量资料以均数±标准差表示,两组间计量资料的比较采用独立样本t检验;计数资料以n(%)表示,组间比较采用χ2检验;采用Pearson相关分析法分析治疗组一般临床资料、随访时间(首次接受131I治疗到首次图像采集的时间)、首次用药剂量、累计用药剂量与腮腺、颌下腺Emean的相关性;采用多元线性回归分析腮腺、颌下腺Emean的独立相关因素。以Plt;0.05为差异有统计学意义。
2" 结果
2.1" 左、右侧腮腺及颌下腺弹性参数比较
对照组左、右侧腮腺Emean值分别为8.77±1.24、8.35±0.85 kPa;左、右侧颌下腺Emean值分别为8.21±1.32、8.61±1.32 kPa;同一部位左、右侧Emean值差异无统计学意义(Pgt;0.05)。治疗组左、右侧腮腺Emean值分别为13.36±3.34、13.14±3.28 kPa;左、右侧颌下腺Emean值分别为11.81±2.18、12.03±2.32 kPa;同一部位左、右侧Emean值差异无统计学意义(Pgt;0.05)。
2.2" 治疗组与对照组平均腮腺、颌下腺弹性参数比较
对照组与治疗组腮腺、颌下腺的平均Emean值分别为8.56±0.71、8.41±1.00、13.25±2.98、11.92±2.06 kPa。组间相同部位两两比较差异有统计学意义(Plt;0.001);组内不同部位比较:治疗组腮腺Emean大于颌下腺Emean(Plt;0.05),对照组腮腺、颌下腺Emean比较差异无统计学意义(Pgt;0.05,表2)。
2.3" 涎腺弹性参数与BMI、性别、随访时间、累计用药剂量、用药次数的相关分析及多元线性回归分析
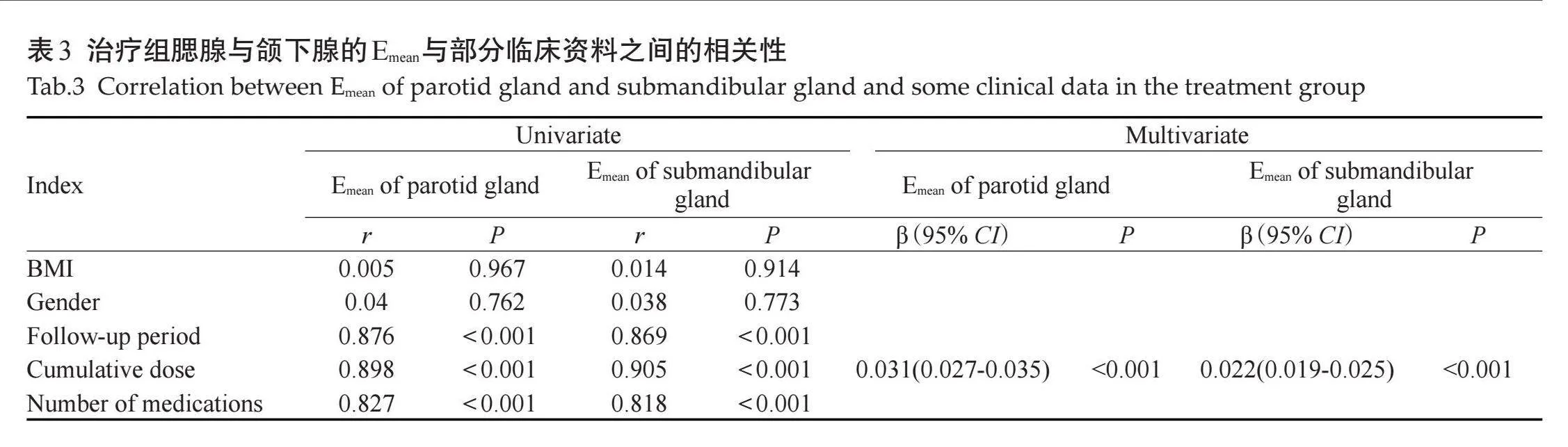
Pearson相关分析结果提示,腮腺Emean、颌下腺Emean均与随访时间、累计用药剂量及用药次数呈线性相关(Plt;0.001);多元线性回归分析显示累计用药剂量与腮腺Emean、颌下腺Emean均呈独立相关(Plt;0.001,表3)。
3" 讨论
涎腺辐射损伤是 PTC 患者术后行131I 治疗的常见不良反应。其作用机制为甲状腺滤泡上皮细胞基膜上的钠/碘同向转运体与131I结合,释放β射线消除术后残留甲状腺或可疑转移病灶,而腮腺和颌下腺小叶导管上皮细胞的细胞膜也有钠/碘同向转运体表达,治疗后涎腺中碘浓度为血浆碘浓度的30~40倍[17],引起涎腺导管扩张、炎性细胞浸润、腺泡细胞变形凋亡、腺体萎缩、纤维化[19-21]。涎腺组织损伤越重,组织纤维化程度越高。有研究发现组织纤维化程度与剪切波杨氏模量值呈正相关[22],说明剪切波杨氏模量值可以反映组织纤维化程度,进而反映组织损伤程度。本研究首次应用SWE测量131I治疗后患者的腮腺和颌下腺的杨氏模量值,判断其纤维化程度,为临床判断涎腺损伤提供一个新的、简便的、无创、无辐射、定量、可重复性高的影像学方法。
有报道显示经131I治疗后涎腺体积明显减小[23];也有研究报道了从低到中剂量的131I治疗后,腮腺体积增加,进一步增加131I的剂量后,腮腺体积萎缩[24]。本研究结果显示治疗组腮腺的厚度与颌下腺体积较对照组均减小,但差异无统计学意义,这与既往研究结果有差异,是因为炎症早期导管堵塞引起的腺体体积增大,病程进展出现腺体功能退化导致腺体萎缩;且不同研究中炎症时期不同、用药剂量不同,研究对象数量不同等都可引起此类差异。
本研究结果发现,治疗组腮腺、颌下腺Emean大于对照组,这与既往研究[23]应用声辐射脉冲弹性成像评估131I治疗后涎腺的弹性变化的结果一致,说明131I治疗1年后有口干症状的PTC患者涎腺组织受损,实质纤维化。本研究中治疗组涎腺体积较对照组减小,差异无统计学意义,但治疗组Emean值较对照组增高,说明涎腺损伤组织硬度改变早于形态学改变;因此SWE可能为临床较早期的判断涎腺腺损伤提供一个定量指标。
有学者提出腮腺是纯浆液性腺体,而颌下腺是含有浆液性和黏液性腺泡的混合腺,黏液性腺泡中的黏蛋白能有效降低辐射影响,因此腮腺对辐射最为敏感[25, 26]。既往有学者应用全身核素显像通过观察131I治疗后腮腺和颌下腺的摄取及排泌功能证实了腮腺比颌下腺受放射性碘的影响更大[27]。本研究结果显示131I治疗后腮腺Emean大于颌下腺,说明131I治疗后腮腺较颌下腺组织纤维化程度更严重。本研究结果与既往研究结果一致,但全身核素显像具有放射性,且可重复性低。因此SWE作为一种无创、无辐射、可重复的超声检查新技术在评估131I治疗后涎腺损伤有一定临床价值。
本研究结果显示,累计用药剂量与Emean呈独立正相关。131I累计用药剂量增加,腮腺及颌下腺Emean值增大,组织纤维化程度增加,组织损伤加重。既往国内外学者用超声、核素动态显像及计算机断层扫描等技术分别对131I治疗后涎腺的超声形态学变化及功能损伤程度进行评价,结果均显示131I治疗剂量与涎腺的体积和腺体摄取及排泌功能相关,即与腺体损伤程度相关[7, 28, 29]。但常规超声成像不能定量评估腺体损伤情况,核素显像及计算机断层扫描具有放射性,限制其应用于涎腺的随访观察。本研究结果与既往研究结果基本一致,说明SWE可作为一种定量、便捷、无辐射、可重复的影像检查方法为临床评估经131I治疗PTC全切后患者涎腺的组织损伤。
本研究尚存在一定的局限性:本研究样本量相对较小且为横断面研究,尚没有纳入相关随访,在后续的研究中可进行队列研究,进一步探讨相同剂量131I治疗前、后不同时间段患者涎腺的杨氏模量值的变化,进一步应用SWE行诊断性分析;因样本量有限,本研究未对用药剂量进行分组并评估不同剂量涎腺杨氏模量值之间的差异;未对口干症状进行分级来评估口腔症状和涎腺杨氏模量值之间的相关性。
综上所述,SWE作为一种无创、无辐射、简便、可重复的影像学检查方法,可为临床131I治疗后腮腺和颌下腺损伤的观察诊疗提供一个定量监测参考指标。
参考文献:
[1]" " 中华医学会核医学分会. 131I治疗分化型甲状腺癌指南(2021版)[J]. 中华核医学与分子影像杂志, 2021, 41(4): 218-41.
[2]" "Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review, 1975-2017. Bethesda, MD: National Cancer Institute[EB/OL]. [2020-09-20]. http://seer.cancer.gov/csr/19752017/.
[3]" "Ho AS, Luu M, Barrios L, et al. Incidence and mortality risk spectrum across aggressive variants of papillary thyroid carcinoma[J]. JAMA Oncol, 2020, 6(5): 706-13.
[4]" "Clement SC, Peeters RP, Ronckers CM, et al. Intermediate and long-term adverse effects of radioiodine therapy for differentiated thyroid carcinoma: a systematic review[J]. Cancer Treat Rev, 2015, 41(10): 925-34.
[5]" " 彭" "东, 刘学芬, 刘徽婷, 等. 甲状腺根治术后不同剂量131I清甲治疗对分化型甲状腺癌患者唾液流率、骨代谢和生活质量的影响[J]. 现代生物医学进展, 2021, 21(3): 537-40, 449.
[6]" " 赵佳雄, 南欣荣, 孟" 兵, 等. 甲状腺癌131I治疗后相关唾液腺炎的诊疗进展[J]. 中华口腔医学研究杂志: 电子版, 2022, 16(3): 199-202.
[7]" "Tsur N, Avishai G, Alkan U, et al. Ultrasonographic features of salivary glands after radioiodine therapy in patients with thyroid cancer[J]. Laryngoscope, 2023, 133(5): 1271-5.
[8]" " 王贵玲, 刘光晖, 李德顺, 等. 131I治疗后全身显像预测分化型甲状腺癌患者放射性唾液腺损伤[J]. 中华核医学与分子影像杂志, 2018, 38(3): 164-7.
[9]" "Simões Lima GA, López RVM, de Freitas RMC, et al. Evaluation of parotid salivary gland echo texture by ultrasound examinations and correlation with whole‑body scintigraphy after radioiodine therapy in patients with differentiated thyroid carcinoma[J]. J Ultrasound Med, 2020, 39(9): 1811-8.
[10] Herman J, Sedlackova Z, Vachutka J, et al. Shear wave elastography parameters of normal soft tissues of the neck[J]. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub, 2017, 161(3): 320-5.
[11]" 金" 亚, 彭玉兰, 赵海娜, 等. 正常成人腮腺和颌下腺实时剪切波弹性成像的初步研究[J]. 华西医学, 2015, 30(4): 692-5.
[12]" 陈" 娟, 谢明星, 王" 静, 等. 实时剪切波弹性成像评价干燥综合征患者涎腺弹性模量的初步临床研究[J]. 中华超声影像学杂志, 2018, 27(3): 220-5.
[13]" 唐益勇, 施燕芸, 范光磊, 等. 剪切波弹性成像与涎腺超声评分法诊断干燥综合征涎腺病变的临床价值[J]. 中华超声影像学杂志, 2021, 30(8): 709-14.
[14]" 游小慧, 薛" 敏, 卢" 颖, 等. ARFI在头颈部肿瘤放疗后腮腺损伤评估中的应用[J]. 南京医科大学学报: 自然科学版, 2018, 38(12): 1816-8.
[15]" Kałużny J, Kopeć T, Szczepanek-Parulska E, et al. Shear wave elastography: a new noninvasive tool to assess the intensity of fibrosis of irradiated salivary glands in head and neck cancer patients[J]. Biomed Res Int, 2014, 2014: 157809.
[16] Horvath E, Skoknic V, Majlis S, et al. Radioiodine-induced salivary gland damage detected by ultrasonography in patients treated for papillary thyroid cancer: radioactive iodine activity and risk[J]. Thyroid, 2020, 30(11): 1646-55.
[17]" Oh JM, Kalimuthu S, Gangadaran P, et al. Reverting iodine avidity of radioactive-iodine refractory thyroid cancer with a new tyrosine kinase inhibitor (K905-0266) excavated by high-throughput NIS (sodium iodide symporter) enhancer screening platform using dual reporter gene system[J]. Oncotarget, 2018, 9(6): 7075-87.
[18]" Badea AF, Tamas Szora A, Ciuleanu E, et al. ARFI quantitative elastography of the submandibular glands. Normal measurements and the diagnosis value of the method in radiation submaxillitis[J]. Med Ultrason, 2013, 15(3): 173-9.
[19]" 李审绥, 吴沉洲, 乔翔鹤, 等. 辐射损伤唾液腺机制及治疗的研究进展[J]. 华西口腔医学杂志, 2021, 39(1): 99-104.
[20]" Prendes BL, Orloff LA, Eisele DW. Therapeutic sialendoscopy for the management of radioiodine sialadenitis[J]. Arch Otolaryngol Head Neck Surg, 2012, 138(1): 15-9.
[21]nbsp; Peng XH, Wu Y, Brouwer U, et al. Cellular senescence contributes to radiation-induced hyposalivation by affecting the stem/progenitor cell niche[J]. Cell Death Dis, 2020, 11(10): 854.
[22]" Jiang TA, Tian G, Zhao QY, et al. Diagnostic accuracy of 2D-shear wave elastography for liver fibrosis severity: a meta-analysis[J]. PLoS One, 2016, 11(6): e0157219.
[23] Rahatli FK, Turnaoglu H, Iyidir OT, et al. Assessment of parotid and submandibular glands with shear wave elastography following radioactive iodine therapy for papillary thyroid carcinoma[J]. J Ultrasound Med, 2019, 38(2): 357-62.
[24]" Brozzi F, Rago T, Bencivelli W, et al. Salivary glands ultrasound examination after radioiodine‑131 treatment for differentiated thyroid cancer[J]. J Endocrinol Invest, 2013, 36(3): 153-6.
[25] Wu JQ, Feng HJ, Ouyang W, et al. Systematic evaluation of salivary gland damage following 131I therapy in differentiated thyroid cancer patients by quantitative scintigraphy and clinical follow-up[J]. Nucl Med Commun, 2015, 36(8): 819-26.
[26]" da Fonseca FL, Yamanaka PK, Mazoti L, et al. Correlation among ocular surface disease, xerostomia, and nasal symptoms in patients with differentiated thyroid carcinoma subjected to radioiodine therapy: a prospective comparative study[J]. Head Neck, 2017, 39(12): 2381-96.
[27]" Jeong SY, Kim HW, Lee SW, et al. Salivary gland function 5 years after radioactive iodine ablation in patients with differentiated thyroid cancer: direct comparison of pre‑and postablation scintigraphies and their relation to xerostomia symptoms[J]. Thyroid, 2013, 23(5): 609-16.
[28]" 周" 科, 贾志云. 核素动态显像对131Ⅰ治疗分化型甲状腺癌患者唾液腺损伤程度的评价[J]. 解放军预防医学杂志, 2019, 37(1): 83-5, 99.
[29]" Lee HN, An JY, Lee KM, et al. Salivary gland dysfunction after radioactive iodine (I-131) therapy in patients following total thyroidectomy: emphasis on radioactive iodine therapy dose[J]. Clin Imaging, 2015, 39(3): 396-400.
(编辑:郎" 朗)