Validation of the Portuguese version of the social isolation scale with a sample of community-dwelling older adults
2023-05-14JoTavarsAnaFariaDlphinGonalvsDianaMnsSofiaSilvaLilianaSousa
João Tavars ,Ana Faria ,Dlphin Gonçalvs ,Diana Mns ,Sofia Silva ,Liliana Sousa b,
a Health School, University of Aveiro, Aveiro, Portugal
b Center for Health Technology and Services Research (CINTESIS@RISE), Portugal
c Health Sciences Research Unit: Nursing (UICISA: E), Portugal
d Department of Education and Psychology, University of Aveiro, Aveiro, Portugal
e The Polytechnic Institute of Coimbra, Coimbra Education School, Coimbra, Portugal
Keywords: Aged Loneliness Portugal Psychometrics Social isolation
ABSTRACT Objectives: The aim of this study was to analyze the psychometric properties (reliability and validity) of the Social Isolation Scale (SIS) in a sample of Portuguese community-dwelling older adults.Methods:A transversal descriptive study was carried out with a convenience sample of 250 communitydwelling older adults(≥65 years).The survey comprised a sociodemographic questionnaire,SIS,Geriatric Depression Scale-4 (GDS-4),6-item Lubben Social Network Scale (LSNS-6),a loneliness self-assessment question,and Satisfaction with Life Scale (SWLS).Construct validity (confirmatory factor analysis) and convergent validity were analyzed,and ISI internal reliability (composite reliability),external reliability(test-retest,intraclass correlation coefficient) and inter-rater reliability (Cohen’s kappa coefficient) were evaluated.Results:Confirmatory factor analysis showed a two-factor model with an excellent index of fit.The SIS showed significant correlations with LSNS-6(rs=0.47),SWLS(rs=0.26),the loneliness self-assessment question (rs=0.35),and GDS-4 (rs=-0.16).SIS composite reliability was good (0.708).The inter-class correlation coefficient varied from 0.84 to 0.98.The Cohen’s kappa coefficient ranged from 0.936 to 1.Conclusions:SIS has been shown to be a valid and reliable instrument for assessing social isolation among Portuguese community-dwelling older adults.Healthcare professionals,particularly nurses working in community settings,can use SIS to assess social isolation in older adults to design,implement,and evaluate interventions.
What is known?
·Social isolation is a global social and health problem affecting many older adults.
·The Social Isolation Scale(SIS)is a brief(6-item)instrument that assesses both the objective and subjective components of social isolation,providing a quick appraisal of social isolation in older adults.
·Assessing social isolation in community-dwelling older adults with valid and reliable instruments is crucial for surveillance,prevention,and adequate intervention.
What is new?
·The psychometric properties of SIS,Portuguese version for community-dwelling older adults,show that the instrument is valid and reliable.
·To our knowledge,this is the first instrument validated for the Portuguese older adult population that assesses social isolation by considering both objective and subjective components.
·Having SIS validated for the Portuguese older adult population will allow healthcare professionals,including nurses,working in community settings to provide better assessments and thus design and implement more adequate interventions.
1.Introduction
Social isolation(SI)among older adults has been identified as a relevant public health issue in recent decades [1].This phenomenon has gained increasing relevance due to the social distancing measures introduced in response to the COVID-19 pandemic [2].The concept of SI has been inconsistently defined,demonstrating the complexity of the phenomenon[3].In the 1990s,Lien-Gieschen[4]defined SI as the experience of having the need for contact with other people but being unable to make that contact.This definition was the first to consider the feelings and perspectives of older adults.Nicholson [5] defined SI as the distancing of an individual,psychologically or physically or both,from their desired or needed network of relationships with other persons.This last definition of SI comprises two components:objective and subjective SI[3,6-8].Objective SI refers to physical separation and/or little interaction with other people,commonly measured by indicators such as living alone,having a small social network,being single,and being childless[9].Subjective SI encompasses the individual’s perception of their social relationships considering quality,integration,and involvement [10].The common indicators of this component include a perceived lack of social support,low involvement in social activities,and feelings of loneliness or not belonging.
SI may occur at any age;however,as people age,opportunities to socialize and form relationships tend to diminish.A known set of factors contributes to the decrease in social interaction among older adults [11]-namely,the retirement process,which leads to the loss of daily contact with co-workers[12];health problems and physical frailty,which limit the individual’s mobility [13];and possible mourning due to the loss of close relatives and friends[14].Thus,SI is more prevalent among older adults,with estimates ranging from 10% to 43% depending on historical background and living conditions[15,16].In industrialized countries,SI affects about one-third of older adults [17].A population-based study in the United States of America [18] found that 24% of older people reported SI,which corresponds to 7.7 million people,of which about 1.3 million (4%) had severe SI.In Portugal,theCensos S′eniorreported that 42,439 older adults were living alone and/or were isolated[19].
The ability to build and maintain relationships is a basic human need and one of the main functional abilities highlighted in the healthy aging paradigm [20].Being socially active and involved in social relationships has been shown to have a positive impact on mental and physical well-being and on increased longevity[21,22].In contrast,SI negatively impacts both physical (increases the risk of cardiovascular diseases,cognitive decline,morbidity,and mortality,as well as stress) [23-25] and mental health (depression,anxiety,and insomnia) [24-27].Research has shown that one in every 12 older adults suffers severe consequences from SI in terms of health and quality of life[17].Preventing the negative effects of SI requires healthcare professionals to make appropriate assessments to mitigate modifiable risk factors and develop interventions that can reduce SI among older adults.
Nicholson et al.[7] reported that instruments exist that assess either the objective or subjective aspects of SI,but there are no instruments that measure both components.Neglecting to assess both components may limit the understanding of SI,contributing to underestimating it [28].In 2020,Nicholson and colleagues published the Social Isolation Scale(SIS),a brief instrument(six items)that measures both components: objective connectedness and subjective belongingness [3,8].SI represents a global threat to the health,well-being,and quality of life of older adults,a population that is projected to grow exponentially in the coming decades.In Portugal,the fourth most aged country in the world (21.1% of the population is ≥65 years old [29]),SI among older adults must be addressed as a key issue.Therefore,a project titled“Social isolation in older community-dwelling adults in Portugal” was carried out with the aim of validating the SIS in two steps.The first was the translation,adaptation,and content validation for the Portuguese population[30].The second,reported in this study,is the analyses of validity (construct and convergent) and reliability (internal consistency,test-retest,and inter-rater) [31].Thus,this study was aimed at analyzing the psychometric properties (reliability and validity) of the Portuguese version of the SIS in a sample of Portuguese community-dwelling older adults.
2.Methods
2.1.Design
This is a quantitative descriptive study that adhered to the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) checklist [32].
2.2.Ethical approval
The study was approved by the Ethics Committee of the Nursing School of Coimbra: reference 711/09-2020.Participation was voluntary and anonymous.Aspects such as the right to refusal and the confidentiality and anonymity of participants were ensured through informed written consent.
2.3.Study settings and participants
Non-random convenience sampling of community-dwelling older adults living in Portugal was conducted.Inclusion criteria were being aged 65 years or older,community-dwelling,and having the ability to understand the questionnaire and answer the questions.Exclusion criteria were the inability to communicate verbally,living in a long-term care facility or intermediate care unit,using a day-care center (since social interaction tends to be structured around the center users and staff),and having a cognitive impairment(assessed through Mini-Cog).A sample size of at least 200 participants was targeted to make confirmatory factor analysis(CFA) feasible.This sample size was based on the number of participants per item,with at least 10 to 1.For CFA to determine the adequacy of the model,n≥200 [33].
2.4.Instruments
The sociodemographic questionnaire focused on sex,age,marital status,area of residence,type of dwelling (house or apartment),living arrangement (alone,with spouse/partner,extended family),family income,years of formal education,number of children,and professional status.
The SIS was developed by Nicholson and colleagues [7] for assessing SI among older adults(≥65 years).It has two dimensions:objective connectedness and subjective belongingness.The connectedness (3 items) questions ask participants to indicate certain frequencies(on a Likert scale from 0 to 6 or more)related to contact with family,friends,and neighbors.The belongingness (3 items) questions ask participants to rate agreement (on a Likert scale from strongly disagree to strongly agree) with questions regarding relationships and activities (being fulfilled,belonging,and time spent on social activities).In the original version,the CFA results revealed an excellent factor model fit (CFI=0.997,RMSEA=0.038) with good internal consistency (Cronbach’s α=0.77)[7].In this instrument,lower scores indicate higher levels of SI.After obtaining approval to translate and use SIS from the author,Dr.Nicholas R.Nicholson,the scale was translated,adapted,and content validated for the Portuguese older adult population by Tavares et al.[30](Appendix A)(content validity index ≥0.89 and a modified kappa,with values considered excellent,which ranged from 0.89 to 1) [30].
To analyze the convergent validity properties,we used the following instruments that were validated for the Portuguese older adult population.Loneliness in its subjective component was measured with a self-assessment question: “Do you often feel lonely?” This question was answered on a 4-point Likert scale(1=always to 4=never),with higher scores indicating less loneliness [34].
The six-item Lubben Social Network Scale (LSNS-6) is a brief version of this scale designed to measure objective social engagement in older adults by considering primarily the quantitative nature of social networks [7].The original version was developed by Lubben(1988)with 12 items.Later,the abbreviated version(LSNS-6) was evaluated by Lubben et al.[35] as having higher levels of internal consistency(0.83),stable factor structures(two subscales:family,3 items,and friends,3 items),and higher correlations with criterion variables.The score varies from 0 to 30,with a higher score indicating greater social engagement.This scale was validated for Portugal by Ribeiro and colleagues[36]and consists of the same two factors (family and friends).Internal consistency was 0.798(total scale),0.756 (family),and 0.732 (friends).
The Satisfaction with Life Scale (SWLS) assesses a person’s degree of satisfaction with their living conditions,their choices,and what they have achieved.It was developed by Diener and colleagues[37]and validated for the Portuguese population by Sim~oes[38].This author adjusted some aspects in the translation,thereby making the content easier for individuals with lower levels of education to understand,and reduced the number of response options from seven in the original to five.This instrument is widely used with older adults and includes five items rated on a 5-point Likert scale (1=strongly disagree to 5=strongly agree).The life satisfaction score ranges from 5 to 25,with a higher score indicating a higher degree of life satisfaction.The Portuguese version[38] shows good internal consistency (Cronbach’s α coefficient of 0.77)and good convergent validity.
The Geriatric Depression Scale (GDS-4) assesses the presence of depressive symptoms in older adults;it is an abbreviated version of the GDS-30 [39].Different versions of GDS,with 10,5,or 4 items,have since been published [40].In this study,we used the GDS-4,which was validated for Portugal by Santos and colleagues [41]with a sample of 1023 people(mean age:71 years)through CFA.The Portuguese GDS-4 version showed a model with adequate fit values(χ2/df=4.210,CFI=0.991 and RMSEA=0.055)and a Cronbach’s α of 0.71[41].This scale includes four questions about how participants felt in the last week,which are answered with either“yes”(0 points)or“no”(1 point).The total score varies from 0 to 4.
2.5.Data collection
Data collection took place between October 2021 and March 2022 and was carried out by five trained researchers.The researchers’preference was to collect the data through an interview(171,65.3%),but some participants preferred to complete the survey on their own (91,34.7%).Participants were recruited through the researchers’social networks and from nearby geographic areas;in addition,community institutions (e.g.,senior universities,municipalities,and recreational associations) were contacted to disseminate the study and support the recruitment of participants.The time taken to complete the questionnaire was 19 ± 6.7 min(ranging from 10 to 40 min).The SIS takes 3.6±0.7 min to complete(ranging from 3 to 5 min).After identifying potential participants,the project and the collaboration required were explained in detail to them.Those who agreed to collaborate signed an informed consent form.With some participants,the interview was carried out immediately (usually at their home or at a community institution office),while with others,the interview was scheduled for a day,place,and time of the participant’s convenience (commonly,their home).The administration of the questionnaire started with the application of the Mini-Cog [42],translated into several languages (https://mini-cog.com/mini-cog-in-other-languages/).At this point,12 participants with cognitive impairment were excluded(total score ≤2).The survey was then administered to the participants without cognitive impairment.Once this was complete,the interviewer thanked the participants for their collaboration.The sample comprised 250 participants.
2.6.Data analysis
In the descriptive statistics for the categorical variables,frequency and percentage were used;for the continuous variables,mean and median were used.The measurement properties were as follows.
Regarding construct validity,maximum likelihood estimation is a method that determines values for the parameters of model estimation.To assess the model fit,goodness of fit indices and the criteria suggested by Mar^oco [33] were used,including χ2,comparative fit index (CFI ≥0.9),normed fit index (NFI ≥0.9);Tucker-Lewis index (TLI ≥0.9);goodness of fit index (GFI ≥0.9);root mean square error of approximation (RMSEA <0.08);standardized root mean square residual (SRMR);Akaike information criterion (AIC);and Bayesian information index (BIC).
Convergent validity was measured through correlations between the SIS and GDS-4,the loneliness self-assessment question,LSNS-6,and SWLS.The correlation was measured by Spearman’s rank correlation coefficient(1-0.39,a weak correlation;0.40-0.69,a moderate correlation;0.70-0.89,a strong correlation;≥0.90,a very strong correlation) [43].
Internal consistency reliability was evaluated using composite reliability (CR) coefficients,with values between 0.60 and 0.70 considered acceptable and values between 0.70 and 0.90 considered satisfactory [44].
For test-retest reliability,the intraclass correlation coefficient(ICC)was used to test the adequacy of the instrument.The SIS was applied at two moments,with an interval of two weeks,to the same participants and under the same circumstances.The ICC cut-off values are as follows:<0.5 is poor;between 0.5 and 0.75 is moderate;between 0.75 and 0.9 is good;>0.9 is excellent [45].
Inter-rater reliability (IRR) was assessed by two raters (3rd and 4th authors).In the IRR data collection,on the same days,the 3rd author assessed the questionnaire and approximately 10 min later,the 4th author (second rater) assessed SIS.Cohen’s kappa coefficient (κ),the kappa statistic,and total agreement between investigators were calculated.This measure has values between -1 and 1,where 1 means perfect agreement and -1 means perfect disagreement.The value of 0 is verified when the observed and expected agreement are exactly the same due to chance.The values ofκcan be interpreted in several ways.In this study,these values were poor(κ<0),weak(0<κ<0.20),considerable(0.21<κ<0.40),moderate(0.41<κ<0.60),substantial(0.61<κ<0.80),and almost perfect (0.81<κ<1) [46].
Statistical data analysis was performed using IBM SPSS AMOS and Statistics version 28 software.A significance level ofP<0.05 was used for all comparisons.
3.Results
3.1.Participants
This study had 250 participants (Table 1).The mean age was 73.9(SD=6.4)years,ranging between 65 and 93 years;68.0%of participants were female;65.6%were married or cohabiting;61.6%lived in a rural area,usually in a house (88.0%).Regarding family finances,46% responded “just enough to make ends meet,” and 49.2% answered “some money left over.”
3.2.Validity
3.2.1.Construct validity
First,the model using the original SIS was tested,and the results showed a model with acceptable adjustment,with the exception of the χ2/df.A second model was respecified,after inspection of the modifiable index,with the correlated error covariance between e2 and e3(r=0.24)(Appendix B).The modified indices for this model were as follows:χ2(7)=12.49,P=0.086;CFI=0.96;NF=0.92;TLI=0.92;GFI=0.98;RMSEA=0.06 (95%CI: 0.00-0.106),P=0.364;SRMS=0.06;AIC=40.49;and BIC=89.79 (Fig.1 and Appendix B).Overall,a better fit for the indices was found in the second model.The CFA resulted in two factors for which the correlation was fair,r=0.23.Factor 1 (connectedness) comprised items 1 to 3,with factor loadings of 0.60-0.74.Factor 2 (belongingness)comprised items 4 to 6,with factor loadings of 0.67-0.70.
3.2.2.Convergent validity
There were negative and weak correlations between the SIS score and total GDS-4 score (rs=-0.16),and between the belongingness subscale and GDS-4 (rs=-0.16),with statistical significance.Scores of the total SIS scale and subscales were correlated with the loneliness self-assessment question with significant significance.There was a moderate correlation between LSNS-6 and the SIS total (rs=0.47),and between LSNS-6 and the connectedness subscale (rs=0.57),with statistical significance.There were weak correlations between SWLS and the SIS scores(total scale and subscales) with statistical significance (Table 2).
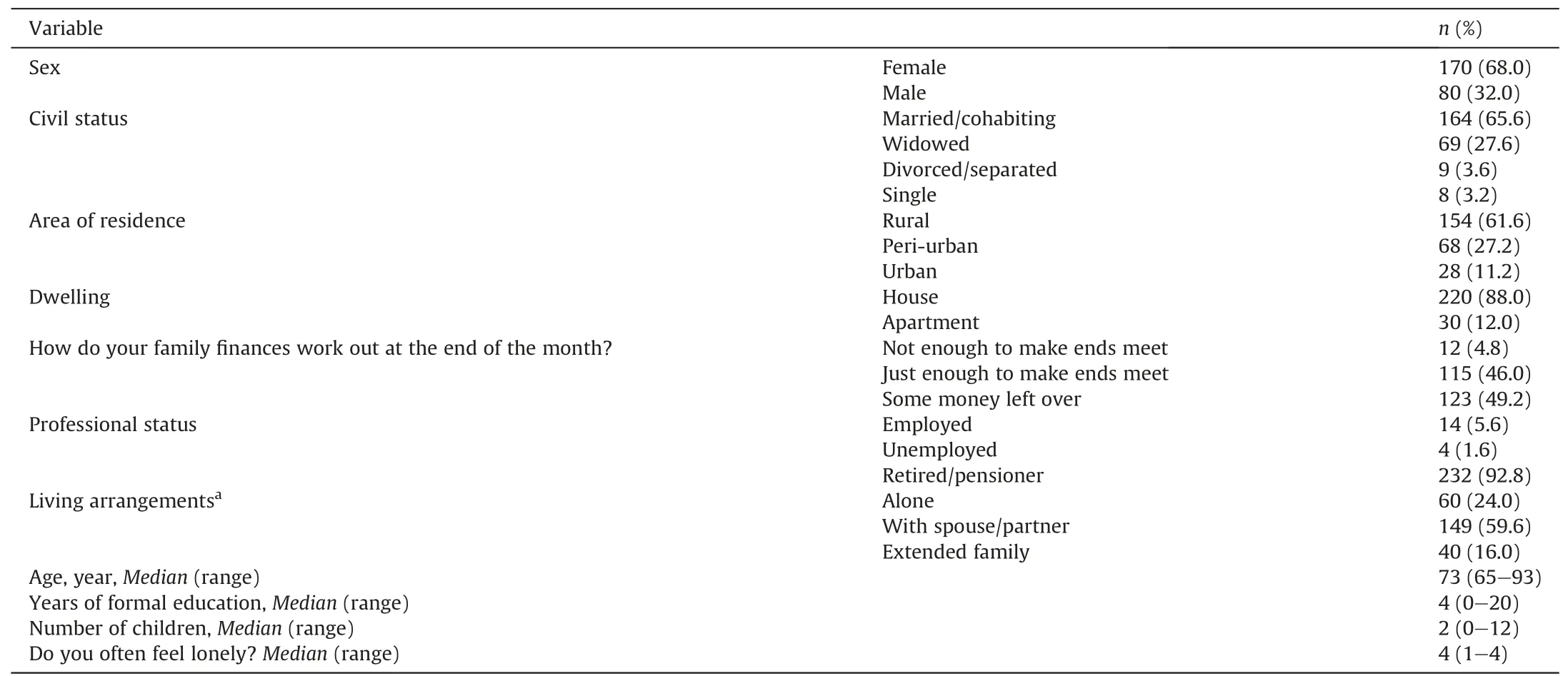
Table 1 Sociodemographic characteristics (n=250).
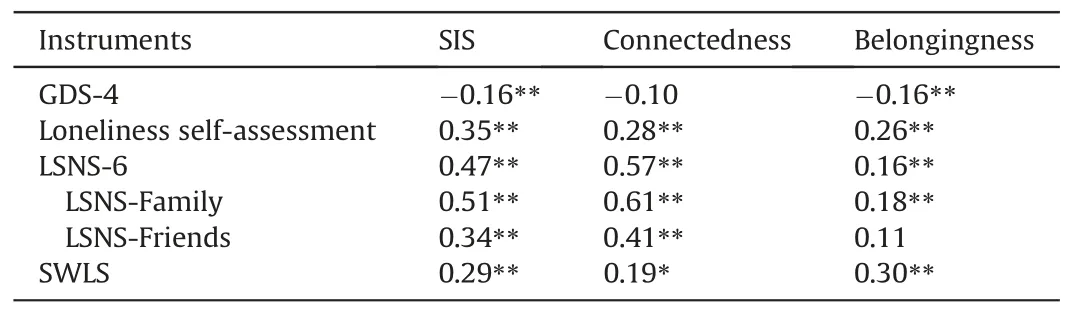
Table 2 Correlation of the SIS with other measures (n=250).
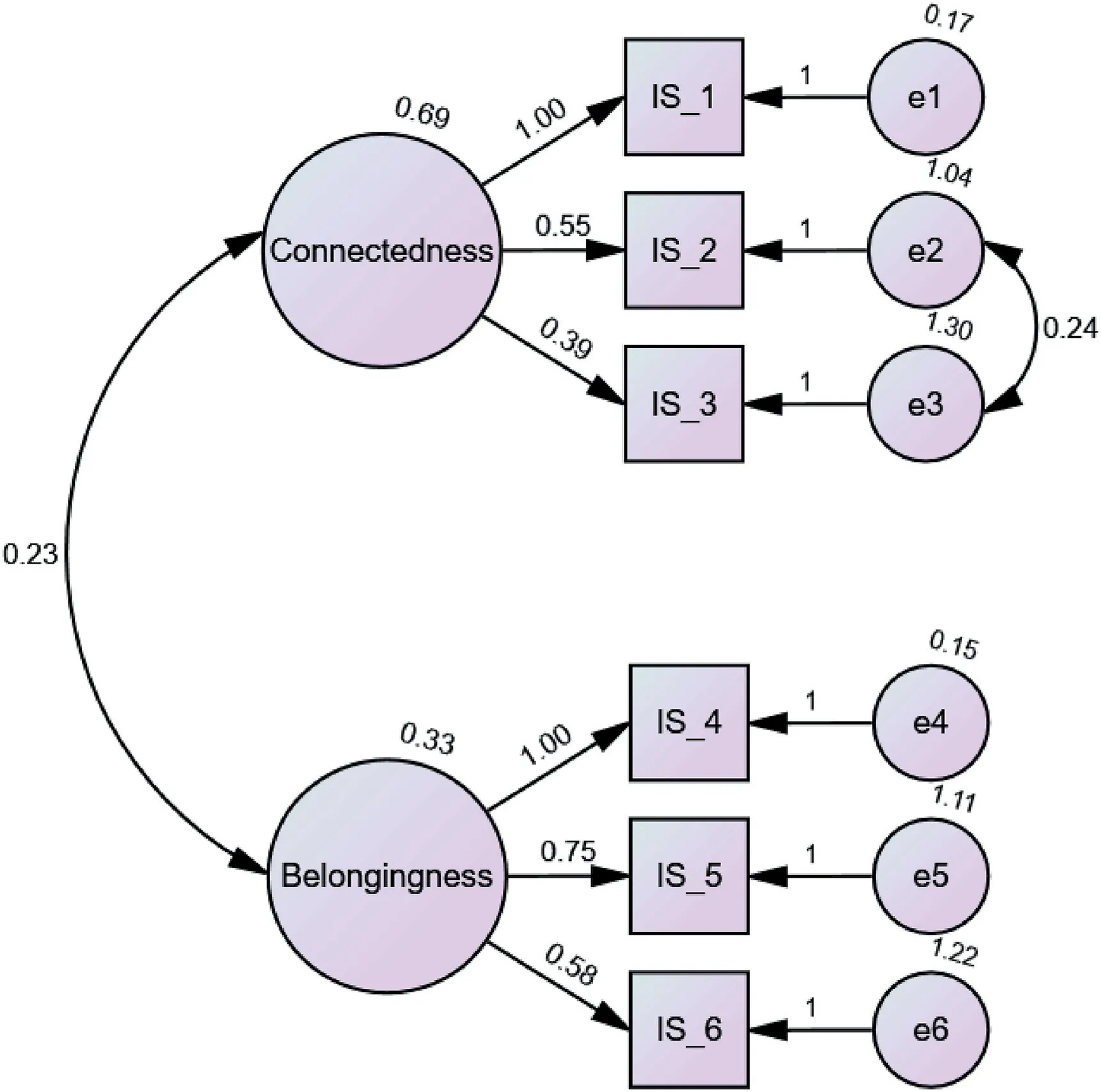
Fig.1.Standardized model parameters for the Portuguese version of SIS.
3.3.Reliability
3.3.1.Internal consistency
CR for the total scale was 0.708;for the connectedness subscale,it was 0.60;and for belongingness,it was 0.54.
3.3.2.Test-retest reliability
The test-retest was performed with a sample of 31 participants.The ICC for the six items ranged from 0.844 to 0.978.The ICC ofitems 1 to 4 was greater than 0.9 between the assessments performed in the test and retest.Items 5 and 6 had ICC <0.9 (item 5:ICC=0.846,95%CI 0.695-0.922,P<0.01;item 6:ICC=0.844,95%CI 0.692-0.921,P<0.01).
3.3.3.Inter-rater reliability
Inter-rater reliability was evaluated with a sample of 41 participants.The inter-rater evaluation was: κ=1,P< 0.01,concordance=100% for items 1,2,4,and 5.Items 3 and 6 showedκ=0.936,P< 0.01,concordance=95.2% and 97.5%,respectively.
4.Discussion
4.1.Psychometric properties of the Portuguese version of the SIS
The aim of this study was to examine the psychometric properties of the Portuguese version of the SIS in a sample of community-dwelling Portuguese older adults.Different approaches were adopted to assess the scale’s reliability and validity(CFA,convergent validity with correlation analysis),in line with Boateng and colleagues[31],who suggested at least two validation approaches as best practices for validating scales.Overall,results suggest that the Portuguese version of the SIS has adequate psychometric properties in terms of validity and reliability.To our knowledge,this is the first instrument validated for the Portuguese older adult population that assesses SI by considering both objective and subjective components.
The CFA,used for construct validity,showed an adequate fit for the structure of the two factors,consistent with the original version[7].This result reinforces the underlying theory that the construct of SI is composed of both an objective connectedness and a subjective belongingness [3,8].In the CFA,a second model was tested to improve the model adjustment.According to Mar^oco [33],it is possible,with a reduced number of changes,to specify the model to significantly improve the fit.The correlation between errors is one possible strategy,provided it is based on a theoretically defensible explanation.In this case,it appears that the number of people with whom the participants communicate(item 2)may include the same persons with whom they feel close at a personal level(item 3).This aspect may explain the correlation between errors (e2 and e3).According to the reference values proposed by Mar^oco [33],a model with a good quality of adjustment was obtained (absolute,relative indices,population discrepancy,and based on information theory).
The convergent validity showed that SIS correlated with other concepts related to SI.The highest scores for correlations were found with LSNS-6-namely,between LSNS-6 total,family,and friends-and SIS-total and SIS-connectedness (correlations were not significant with SIS-belongingness).This result could be expected because LSNS-6 was designed to assess objective social engagement.Correlations were significant between the loneliness self-assessment question and SIS-total,SIS-connectedness,and SISbelongingness.Loneliness and SI are related but different concepts[47].In fact,loneliness is a subjective variable of the emotional status of a person [23].Some authors have distinguished between emotional loneliness and social loneliness.The former results from the lack of close and intimate attachment to other persons,while the latter is associated with the lack of a social network with which to share interests and activities[48].Regarding GDS-4,correlations with SIS were negative for SIS-total and SIS-belongingness with statistical significance (not significant for SIS-connectedness),meaning that older adults with fewer depressive symptoms have a lower risk of SIS-total and belongingness,which is consistent with previous studies [49].Resultssuggest that depressive symptoms are influenced more strongly by the subjective component of SIS,as previous literature has shown[50].Correlations between SWLS and SIS were all positive and statistically significant,meaning that better satisfaction with life is associated with less objective and subjective SI,as verified in other studies[51,52].In addition,when people express satisfaction with life,they tend to show better health and longevity indicators [52].The SWLS had a correlation(rs=0.30) with belongingness,probably because life satisfaction involves a subjective assessment that individuals make of their lives,and SIS-belongingness is the subjective dimension of SI [7].
Regarding reliability,CR was used because it is based on the factor loading obtained in the CFA and is recommended for evaluating internal consistency in this type of analysis.CR has been presented as a more robust precision indicator compared to Cronbach’s α coefficient because,in the CR calculation,the loads or factorial weightings of items are subject to variation,while in the alpha coefficient,the item loadings are fixed [53,54].Thus,we chose to use CR,unlike the original version of the SIS,which used Cronbach’s α coefficient [7].CR for the total SIS scale was 0.708,which is acceptable [55] and in line with the original internal consistency (assessed using Cronbach’s α=0.77) [7].In the Portuguese version,the connectedness subscale showed a CR of 0.60,on the threshold of being acceptable [55],which was lower than that of the original scale(α=0.81)[7].The belongingness subscale showed lower values in the Portuguese version(CR=0.54)than in the original version (α=0.63) [7].In both versions,the values are low,which may be due,as suggested by Nicholson and colleagues[7],to the inverted item (item 5,written negatively).Reliability measures are sensitive to the number of items in a scale,and as a rule,when the number of items is reduced,internal consistency tends to be underestimated[44],while in short scales(<10 items),it is common to find a low internal consistency value.Cultural factors may have influenced these differences between the original(USA) and Portuguese versions;further validations for other countries will allow for better understanding these values.
The reliability results (inter-rater and test-retest) showed consistent scores/responses from participants over time and with different raters,which meets the recommendations of the COSMIN guidelines[32].There is no real consensus on the necessary sample size for investigating rater reliability,but a minimum of 30 participants are required for the results to be stable[45].In our study,the sample size in the test-rest (31 participants) and IRR (41 participants) is considered sufficient [45].Test-retest reliability concerns the reproducibility of the observed value when the measurement is repeated in a stable population.The ICC of all items in this study was equal to or greater than 0.844,demonstrating good temporal stability.IRR makes it possible to perceive whether there is consistency between raters by determining the level of agreement between one or more observers [1].The overall IRR results were excellent(κ≥0.936,P<0.01,concordance ≥95.2%)[46],indicating that the two raters obtained the same results in the SIS for the same older adults.
4.2.Strengths and limitations
In this study,the validation process followed a rigorous methodology using different approaches for validation and reliability according to the COSMIN guidelines.Moreover,the sample size was 46 participants per scale item,and with more than 200 observations,this is considered appropriate for factor analysis,which provides robust evidence supporting the validity and reliability of SIS in community-dwelling Portuguese older adults.Future research with samples of subpopulations of older adults(e.g.,those with comorbidities,residents of long-term care facilities)and with individuals who are socially isolated (recruiting them through the mediation of community projects aimed at minimizing SI) will be relevant to advance the psychometric testing of the SIS.A population-based study to measure the SI in a representative sample of the Portuguese population will be crucial to determining the prevalence of SI,comparing results with other countries or data sources,and implementing strategies.
Our study had some limitations.We selected a convenience sample with the majority of participants living in a rural area.Therefore,further studies should include participants from more urban areas of the country.This study’s participants were active and autonomous,had an adequate family income,and participated in various activities.These characteristics may be protective factors against SI.Socially isolated individuals were likely underrepresented because they were more difficult to reach or because they did not agree to participate.This could indicate sampling bias.Another limitation concerns internal consistency,where CR was slightly below the recommended level for the belongingness and connectedness subscales.This was probably due to the low number of items (three).Thus,a more in-depth evaluation may be necessary for future testing of this instrument.Lastly,the data collection process took place during the pandemic (which is ongoing),although during a phase of less restrictive measures,it may have affected the recruitment and participation of more isolated people.
5.Conclusion
In this study,the SIS was validated for community-dwelling Portuguese older adults.The psychometric properties show that the instrument is valid and reliable.As SI has been identified as a global social health problem,it is important to have validated measures for its assessment,as this will make better prevention and intervention possible.Thus,health and social professionals working in community settings now have a validated and reliable tool to assess SI by considering both its objective and subjective components.Nurses,especially those working in community settings,are in a unique position to detect isolated older adults and promote interventions that can prevent this condition or intervene when an older adult has been identified as at risk of being socially isolated.
Funding
This work was supported by national funds through FCT -Fundaç~ao para a Ci^encia e a Tecnologia,I.P.,within CINTESIS R&D Unit(UIDB/4255/2020 and UIDP/4255/2020)and within the scope of the project RISE (LA/P/0053/2020).
CRediT authorship contribution statement
João Tavares:Conceptualization,Methodology,Formal analysis,Writing-original draft preparation,Writing-review&editing.Ana Faria:Formal analysis,Investigation,Writing -original draft.Delphine Gonçalves:Formal analysis,Investigation,Writing-original draft.Diana Mendes:Formal analysis,Investigation,Writing -original draft.Sofia Silva:Methodology,Supervision,Writingreviewing and editing.Liliana Sousa:Conceptualization,Methodology,Supervision,Writing-reviewing and editing.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of competing interest
All authors do not have to declare any conflict of interest.
Appendices.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2023.03.002.
杂志排行

International Journal of Nursing Sciences的其它文章
- A feasibility study on home-based kyphosis-specific exercises on reducing thoracic hyperkyphosis in older adults
- Development and validation of dynamic nomogram of frailty risk for older patients hospitalized with heart failure
- Effects of pre-operative education tailored to information-seeking styles on pre-operative anxiety and depression among patients undergoing percutaneous coronary intervention: A randomized controlled trial
- Factors influencing the quality of sexual life in the older adults: A scoping review
- Comparison of the effects of three kinds of hand exercises on improving limb function in patients after transradial cardiac catheterization
- The trajectories of physical growth in 4 months postnatal corrected age among preterm infants discharged from neonatal intensive care units and associated factors: A prospective study