A feasibility study on home-based kyphosis-specific exercises on reducing thoracic hyperkyphosis in older adults
2023-05-14WiYingLiJinlingLuYongDaiAgnsTiwariPuiHingChau
Wi Ying Li ,Jinling Lu ,Yong Dai ,Agns Tiwari ,Pui Hing Chau
aSchool of Nursing,Nanjing Medical University,Nanjing,China
bSchool of Nursing,Li Ka Shing Faculty of Medicine,The University of Hong Kong,Hong Kong,China
cDepartment of Gastric Surgery,The First Affiliated Hospital of Nanjing Medical University,Nanjing,China
dInfection Control Office,The Liyuan Hospital of Tongji Medical College of Huazhong University of Science &Technology,Wuhan,China
eSchool of Nursing,Hong Kong Sanatorium &Hospital Limited,Hong Kong,China
Keywords: Aged Exercise Physical functional performance Posture Thoracic vertebrae
ABSTRACT Objectives: This study aimed to assess the feasibility of the home-based kyphosis-specific exercises among Chinese older adults with different exercise habits and explore its potential effects on reducing the kyphosis angle and improving physical performance.Methods:A single-group,pre-and post-test design was conducted according to CONSORT 2010 statement: extension for pilot and feasibility trials.A total of 20 participants aged ≥60 with thoracic hyperkyphosis and rehabilitation potential were recruited from four local communities in Wuhan,China.Participants underwent a six-week home-based kyphosis-specific exercises intervention that included warm-up,muscle strengthens,spinal alignment,spinal mobility and flexibility,and cool down five sections (22 exercises).The intervention involved seven 1-h group classes and 35 times daily home practice with identical content.At pre-and post-intervention,the participants' kyphosis angle in two standing postures,static balance,dynamic balance,cardiopulmonary function,dynamic gait assessment,pain,and self-image were assessed and compared.Feasibility was assessed by group class attendance,home practice adherence,and participant evaluations.Results:All participants completed group classes and >75% home practice.Post-intervention,the participant’s kyphosis angle in relaxed and best-standing postures was changed by -12.0° (-15.5°,-4.0°)(Z=-3.98,P <0.001)and -10.0° (-14.0°,-5.3°) (Z=-3.79,P <0.001),respectively.In addition,participants had significantly less pain (P <0.001),better self-image (P <0.001),and improved performance in five physical assessments (P <0.01).Different pre-intervention hyperkyphosis angle and daily physical activity did not affect intervention effects.Most participants considered the interventional exercise as moderate intensity and satisfactory.Conclusions:Home-based kyphosis-specific exercises showed the possibility of being a feasible intervention.And it was advantageous to reducing the kyphosis angle and improving physical performance.
What is known?
·Thoracic hyperkyphosis is a serious problem,and exercise positively impacts improving hyperkyphosis.
·However,the feasibility and effects of home-based exercise intervention need further exploration.
What is new?
·This study presented a six-week home-based exercise program suitable for Chinese older adults’ lifestyles that reduced their hyperkyphosis and enhanced their physical performance.
·The home-based kyphosis-specific exercise showed similar results of being feasible and effective among older adults having different baseline exercise habits or hyperkyphosis angles.
1.Introduction
Thoracic hyperkyphosis is an exaggerated anterior curvature of the thoracic spine [1].The angle that reflects the thoracic spine curvature is called the kyphosis angle[2].The most commonly used diagnosis criterion of thoracic hyperkyphosis in older adults is kyphosis angle >40°[1].Globally,it affects 20%-40% of community-dwelling older adult[3].A study conducted in Wuhan,China,found that 75.2% of community-dwelling older adults had thoracic hyperkyphosis associated with impaired physical performance [4].These findings underscore the importance of interventions to reduce the kyphosis angle among older adults.
Thoracic hyperkyphosis adversely affects older adults’ physical and psychological health [1,3,5,6].Studies found comparing with individuals having alignment posture,older adults with thoracic hyperkyphosis have significantly reduced muscle strength,impaired gait performance,decreased respiratory function,increased risk of falls,and all-cause mortality [1,3,5-9].Moreover,impaired physical function and dissatisfaction with appearance have been found to affect self-image in older adults negatively[10,11].Given that thoracic hyperkyphosis affects the appearance and physical function,it may also adversely affect self-image.Therefore,interventions to reduce the hyperkyphosis angle should also aim to improve physical function [12].
Current treatment options for thoracic hyperkyphosis include surgery [1],osteopeptide injection [13],menopausal hormone therapy [14],orthosis [15,16],traditional Chinese medicine therapies [17],and exercise [12,18-25].However,surgeries such as vertebroplasty and kyphoplasty are only recommended for patients with severe spinal deformities,vertebral fractures,or neurologic compromise [1,3,5,6].Other treatment methods may require specialized medical equipment or have limited evidence of their effectiveness.Therefore,exercise may be a more practical and costeffective option for community-dwelling older adults with less severe cases of thoracic hyperkyphosis.A previous review found that long-term and short-term exercise programs were effective in reducing hyperkyphosis [26].The kyphosis-specific exercise program designed by Katzman and colleagues,with an intervention period ranging from six months (72 group classes) to eight weeks(24 group classes),achieved the greatest reduction in kyphosis angle,with four studies reporting a decline ranging from 2.2°to 6°[12,20-22].The greater effectiveness of Katzman’s intervention compared to other exercise interventions may be attributed to its component of a comprehensive exercise plan which included exercises activating and strengthening the core and upper/lower extremity muscles,increasing spinal alignment by increasing alignment posture awareness,and increasing correct posture maintaining ability,and improving muscle flexibility and joints mobility [20,27].
However,Katzman’s intervention,which required numerous center-based practices,may not directly apply to Chinese older adults.Chinese has a unique cultural phenomenon in that older adults are commonly occupied with housework and grandchildren caring [28].Hence,the long transportation time required for frequent center-based group classes might hinder them from participating in a long-duration intervention program.Furthermore,a home-based program can address intervention needs in special times such as epidemics,and it is an economical way to increase physical well-being [29].Therefore,it obligated the need to provide home-based interventions to Chinese older adults with thoracic hyperkyphosis.
Nevertheless,the advantages and disadvantages of home-based and center-based interventions were still controversial.Some studies found that center-based intervention had a significant and slightly larger effect on low limb strength and gait speed among sarcopenia patients [30].In contrast,a review found that centerbased intervention showed similar effects but lower long-term adherence among Chronic Obstructive Pulmonary Disease patients[31].Hence,research studies were needed to investigate the potential effects of a home-based program.
Previous intervention studies on hyperkyphosis correction excluded participants who performed regular exercises or did not ask about participants’exercise routines[12,20-22].In addition,a previous cross-sectional study found the insignificant relationship between thoracic hyperkyphosis and exercise habits among Chinese older adults [4].As more than 90% of Chinese older adults report engaging in an exercise in their daily life[4],it is important to investigate the effectiveness of kyphosis-specific exercises as an intervention for reducing thoracic hyperkyphosis in older adults who exercise regularly.
We modified the kyphosis-specific exercise intervention protocols [20,27] to be more home-based by reducing the number of group classes,adding home practice content,and providing a tutorial video for guiding home practice.The main objectives of this feasibility study were: 1) to assess the logistics and adherence of home-based kyphosis-specific exercise intervention among Chinese community-dwelling older adults with hyperkyphosis;2) to investigate potential intervention effects on reducing the kyphosis angle and improving physical performance regardless of older adults’ exercising habits.
2.Methods
2.1.Study design and participants
Guided by the CONSORT 2010 statement:extension for pilot and feasibility trials [32],this study adopted a single group pre-and post-test design.The study was registered on ClinicalTrials.gov(registration ID NCT04143464).
Using experience-based sample size determination is reasonable in the feasibility study design since the main purpose is to determine the potential for progression to a subsequent main trial rather than establishing a precise intervention effect[33].A sample size of 20 was planned to allow the testing of the subject recruitment and intervention implementation.Twenty participants were recruited by convenient sampling from four communities in Wuhan,China.Participants of the previous cross-sectional study were given preference [4].Recruitment e-posters were sent to the resident online chat groups in the communities.
Inclusion criteria included 1) being Chinese;2) aged ≥60-yearold;3) having a kyphosis angle >40°(measured in a relaxed standing posture by a manual inclinometer);4)having the ability to decrease the kyphosis angle ≥5°while standing in best posture,indicating rehabilitation potential.Exclusion criteria included 1)having a cognitive impairment or communication difficulty;2)having central or peripheral neuropathy,untreated severe cardiopulmonary disease,or spinal fracture history;3) taking drugs affecting the nervous system or balance and strength,such as chlorpromazine and diazepam;4) the angle of scoliosis ≥10°;5)having undergone spinal surgeries,or had undertaken any specific therapeutic exercises for posture in the past year or were expected to do so it in the coming six months were also excluded.
2.2.Ethical consideration
The study was conducted according to the guidelines of the Declaration of Helsinki.Ethics approval was obtained from the Institutional Review Board of Liyuan Hospital,Tongji Medical College,Huazhong University of Science and Technology (ID: [2019]IEC (A001);09-08-2019).All participants received an information sheet explaining the study aim,data collecting method,benefit and potential risks,confidential data management,and the right to quit.The written consent form was signed before the baseline assessment.
2.3.Intervention
The home-based kyphosis-specific exercises were developed by a team led by a registered nurse with a fitness coaching license based on modifying two protocols published by Katzman et al.,in 2007 and 2016 [20,27].The main framework of the intervention followed Katzman’s team design of center-based exercise classes combined with daily home exercises,with adjustments to the exercise content and intervention schedule.
2.3.1.Intervention content
We adopted the original 1-h exercise plan with five modifications.First,diaphragmatic breathing was strengthened throughout the 1-h exercise,with two additional sessions added to the warmup and cool-down to enhance the skill.Second,three active warmup exercises,such as stepping and shoulder/waist rotation,were added to increase body flexibility and decrease injury risk [34].Third,the overhead arm wall slide exercise was included,as it has been found to effectively improve scapular alignment associated with spine alignment[35,36].Fourth,practices on unstable surfaces(on rollers) were replaced with those on firm ground to minimize injury risk.Fifth,for home practice safety considerations,an hourlong tutorial video with each exercise demonstration and key point explanation was sent to participants to ensure accuracy in home practice.In summary,our 1-h exercise plan has 22 exercises in total that were divided into five sessions,namely warm-up,back muscle strengthening,spine alignment practice,spine mobility,flexibility practice,and cool down.A complete list of 22 exercises and their purposes are presented in Table 1.
2.3.2.Intervention schedule
The intervention schedule underwent two changes.First,the frequency of center-based group classes was reduced to once a week from the original two or three times a week to accommodate the lifestyle of Chinese older adults better.Second,the home practice adopted the identical content as the center-based group classes,which differed from the original home practice of practicing neutral spinal alignment ≥3 times/day guided by a manual of pictures.Details arrangement was:
(1) Group class: Two 1-h group classes for learning and practicing the exercises were conducted in the first week,and weekly group class was conducted with reinforcement of learning and remedial teaching for five consecutive weeks.A registered nurse taught classes with fitness coaching liscese and a trained assistant nurse.The nurse-to-participant ratio remained above 1:5.
(2) Home-practice: Participants received a tutorial video and a log book after the first group class.They were asked to perform 1-h daily home practice following the video for six weeks except on the days having group classes.They were expected to finish 35 days (5 days in the first week plus six days per week in the subsequent five weeks) of home practice.In the log book,participants were instructed to record the frequency and duration of their home practice and any questions or concerns related to the intervention (Table 1).
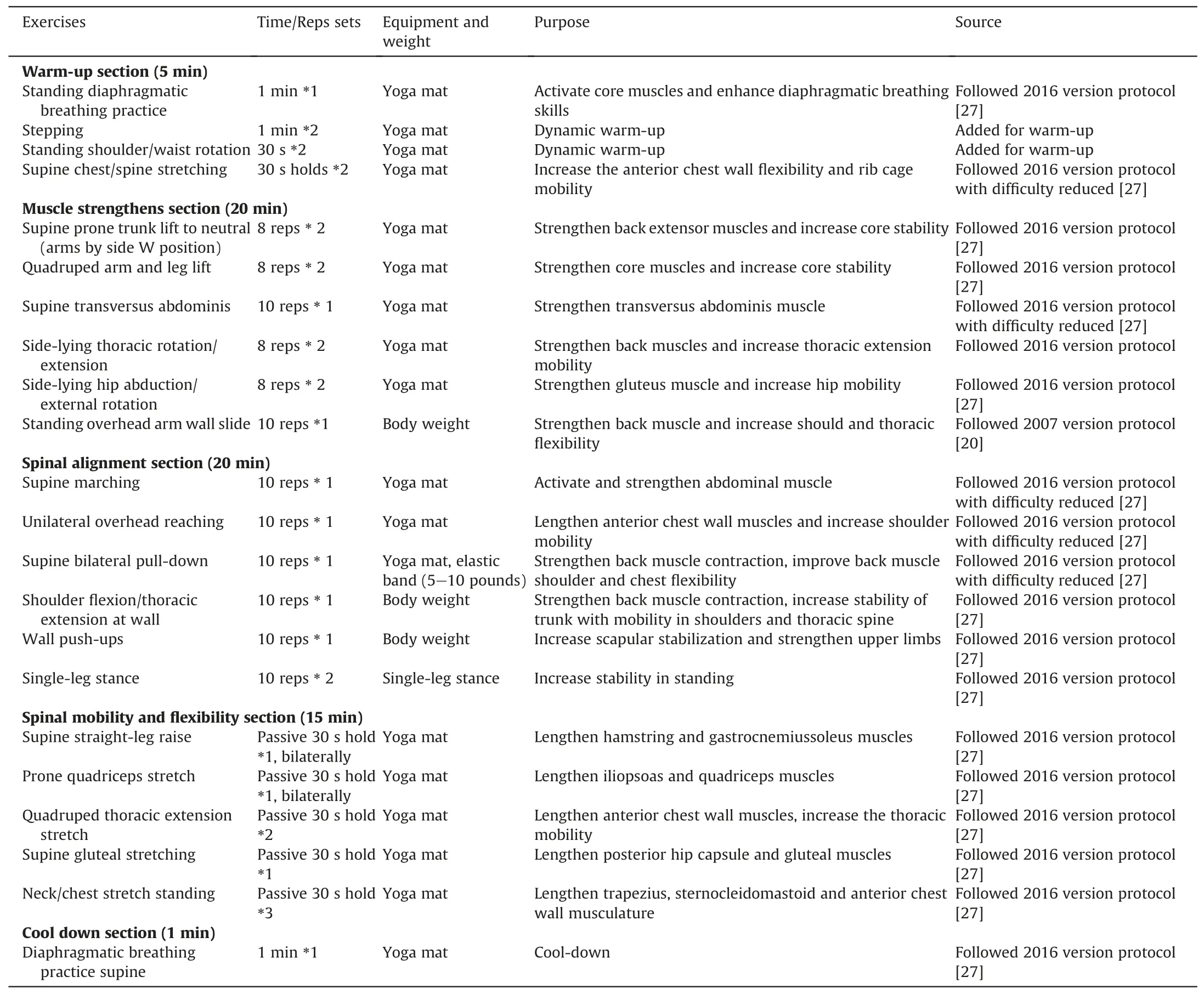
Table 1 Home-based kyphosis-specific exercise list.
2.4.Data collection
From August to September 2019,after obtaining written consent from eligible participants,data collection was conducted by nurses in pre-(week 1,T0)and post-intervention(week 6,T1)in the form of on-site paper-pencil questionnaire,kyphosis angle measurement,and physical assessments.Additionally,participants received follow-up phone interviews in T1 and the 1st,3rd,and 15th months after intervention completion.All tests and assessment tools were free from authorization requirements.
2.4.1.Feasibility,kyphosis angle change
The feasibility of the intervention and kyphosis angle change from T0 to T1 and follow-up phases were evaluated.Three trained nurses not involved in coaching took responsibility for kyphosis angle measurement,while the coach nurse took responsibility for the other assessments.
(1) Class attendance,log-book records,and T1 interviews were used to assess short-term adherence and subjective evaluations of the intervention.T1 phone interviews were conducted in a semi-structured format,with participants providing feedback on their experience,including their evaluation of the intensity of the home-based kyphosisspecific exercises (low/moderate/high),the level of satisfaction with the intervention (low/moderate/high),and whether they would recommend the study to other people(yes/no).
(2) The follow-up phone interview assessed long-term home practice adherence.Participants were asked whether they continued the exercises after the completion of the intervention.For those who continued,the frequency and duration of exercise were collected.For those who did not continue,the reasons for discontinuation were recorded.
(3) The changes in the kyphosis angle from T0 to T1 in relaxed and best standing postures reflected the potential effect of posture correction.A trained nurse identified and marked the spinous processes of C7,T1,T12,and L1 using erasable pens on participants’ bare bodies and used a manual inclinometer measuring kyphosis angle in the relaxed and best standing postures.The angle measurements were performed three times,and the mean angle was calculated for further analysis.The measuring tool,a manual inclinometer,has previously demonstrated excellent inter-rater and intra-rater reliability (ICC >0.90) [37,38] and satisfactory concurrent validity (r=0.86) [37].
2.4.2.Physical performance,pain,self-image
We also assessed changes in physical performance,pain,and self-image from T0 to T1.All selected tools and questionnaires had satisfying validity and reliability [39-44].Three trained nurses(non-coach nurses) took responsibility for this part.
(1) One-leg Standing Test(OLST)was conducted to assess static balance,where participants were asked to raise one leg and maintain the position for as long as possible until it was set back down on the floor [39].Longer OLST time indicates better static balance.This test was repeated three times,and the meantime was recorded for analysis.
(2) Timed Up &Go Test (TUG) was used to assess dynamic balance.Participants were instructed to raise from a chair,walked 3 m,turned around,walked back to the chair,and sit down,while the nurse timing the whole process [40].A shorter TUG time indicates better dynamic balance.This test was repeated three times,and the meantime was recorded for analysis.
(3) Thoracic Expansion Test (TE) was used to evaluate participants’ cardiopulmonary function.The participant’s bust difference in the fourth intercostal level between deep inhale and deep exhale recorded [41].Longer TE length indicates better cardiopulmonary function.This test was repeated three times,mean length was recorded for analysis.
(4) Six Minutes Walking Test(6MWT)also reflected participants’cardiopulmonary function.The test was performed in a 30-m-long,flat square in the community,and participants were instructed to walk as far as possible within 6 min[42].Longer distance covered during the test indicates better cardiopulmonary function.The test was conducted once,and the distance was recorded by three nurses,with the mean distance being used for analysis.
(5) Functional Gait Assessment (FGA) is a 6-m 10-task dynamic gait assessment.Every task scores from 0 to 3 according to the participant’s performance.The total maximum score is 30 [43].A higher FGA score indicates better gait performance.This test was conducted once with three nurses scoring,and the mean score was recorded for analysis.
(6) The changes in self-image and pain were assessed via the Chinese version of Scoliosis Patient Questionnaire-version 22(SRS-22) pain domain (five questions,Cronbach’s α=0.87;ICC=0.76) and self-image domain (five questions,Cronbach’s α=0.78;ICC=0.79).SRS-22 was originally developed to assess the health-related quality of life for patients with scoliosis but later expanded to all patients with spine deformity [44].It has five domains and 22 questions,each rated on a scale of 1-5 according to the subjective evaluation of description fitness;for the adopted two domains,higher scores indicate better self-image and less pain [44].
2.4.3.Socio-demographic and general health information
Participants also filled up questionnaires requesting sociodemographic and health-related information,including age,gender,marital status,education level,chronic disease,and daily physical activity intensity (via the International Physical Activity Questionnaire-Short Form) [45].Scoring <600 equivalent metabolic minutes (MET-min)/week indicated low physical activity intensity,≥3,000 MET-min/week indicated high intensity,and in between indicated moderate intensity.
2.5.Data analysis
Descriptive statistics summarized the participant characteristics.Continuous variables were presented as median and interquartile range,and category variables were frequency and percentage.The attendance rate of group classes and home practice adherence was calculated.The home practice adherence was calculated based on the total number of days participants finished home practice and the total practicing time.Proportions of participants who continued the exercise at the 1st,3rd,and 15th months after T1 were estimated.Qualitative feedback on exercise intensity,level of satisfaction,and recommendation preference in T1,and the reasons for not continuing in follow-ups were tabulated.Paired sample Wilcoxon Signed Rank Test was used to compare the within-group difference.The effects sizerwas estimated based onZusing the formula rA cut-offrvalue of large,medium,and small effects is 0.5,0.3,and 0.1,respectively[46].Mann WhitneyUTest was conducted for subgroup comparison.No missing data needed imputation.The SPSS version 27.0 was used;the significance level was 0.05.
3.Results
3.1.Socio-demographic characteristics
In 10 days,we approached 32 older adults;eight did not show rehabilitation potential,two had scoliosis of ≥10°,and two refused to participate.Thus,20 participants were included,with 15 participating in the previous cross-sectional study.The median(P25,P75) age of the participants was 65.0 (62.0,70.0) year-old;17 were female,18 were married,13 had received at least high school education,and 14 had no medical professional background.All participants reported having chronic diseases,12 had moderate or high daily physical activity intensity,and 10 had a BMI of ≥23,the Asian population’s BMI cut-off for overweight [47].
3.2.Feasibility and effect on posture correction
The group class attendance rate was 100%.Participants’median time at home was 33.0 (31.8,34.0) days,with a median total practice time of 1,610.0 (1,352.5,1,661.3) min.The adherence rate calculated using the total number of practicing days was 94.3%(90.7%,97.1%).However,the home practice adherence rate calculated using the total practice time was 76.7% (64.4%,79.1%).The participants practiced at home for most days.They did not complete the entire 1-h home practice.
Eighteen participants subjectively evaluated the home-based kyphosis-specific exercise intensity as moderate,whereas two evaluated it as high.All participants had a high level of satisfaction with the intervention.Seventeen participants reported that they would recommend the intervention to friends,whereas three were uncertain.All participants reported the onset of muscle soreness in the early phase;however,the soreness disappeared after two weeks of practice.Participants mentioned it was difficult to spend one continuous hour performing in-home practice.They were generally occupied by housework and caring for grandchildren so that they could perform the home practice only in fragments.Participants suggested splitting home practice into short sessions.No adverse events were observed.
For the long-term home practice adherence,19 (95%) participants reported continual practice in the 1st month after T1,while the numbers(proportions)decreased to 11(55%)and 6(30%)in the 3rd month and 15th month after T1,respectively.The reported practice frequencies and durations ranged from 2 to 3 times per week,and practicing time ranged from 20 to 30 min in all three follow-up interviews.The main reasons for not practicing included losing interest due to unchanged exercise content(n=8),worrying about practice accuracy due to no regular center-based class or losing video access (n=4),having satisfied the posture already(n=2).
Participants had reduced kyphosis angles,improved self-image,less pain,and better physical performance in T1 than preintervention (Table 2).The kyphosis angle changed by -12.0°(-15.5°,-4.0°) (Z=-3.93,P<0.001) in the relaxed posture and -10.0°(-14.0°,-5.3°) (Z=-3.79,P<0.001) in the best standing posture,with the effect sizerestimated as 0.89 and 0.85,respectively.In addition,participants showed enhanced static and dynamic balance as the OLS time increased by 23.7 (5.4,37.1) s;(Z=-3.52,P<0.001),TUG time changed by -2.3 (-3.0,-1.2) s(Z=-3.92,P<0.001),and enhanced cardiopulmonary function as TE length and 6MWT distance increased by 0.5 (0.1,0.9) cm(Z=-3.63,P<0.001)and 23.5(3.3,23.5)m(Z=-3.01,P=0.003),respectively.(Table 2).
3.3.Other potential effects
For subgroup analysis,the participants were divided into two groups: T0 kyphosis angle in a relaxed standing posture <50°(n=12) and ≥50°(n=8) (Table 3).Overall,the intervention showed positive effects in both groups,except for 6MWT distance for those with kyphosis angle <50°(Z=-1.87,P=0.062)and SRS-22 (self-image) score for those with kyphosis angle ≥50°(Z=-1.55,P=0.121).Compared with those with a T0 kyphosis angle ≥50°,older adults with a T0 kyphosis angle <50°had a significantly greater improvement in SRS-22(self-image)and SRS-22 (pain) scores.
Participants were also divided into two groups,low physical activity intensity level in T0(n=8)and moderate or high-intensity level in T0 (n=12) (Table 4).The intervention positively affected both groups,except for the 6MWT distance for those in the moderate or high-intensity group(Z=-1.83,P=0.068).There was an insignificant difference in outcome changes between the two groups,except in TUG time.Compared with those reported highintensity levels,older adults reported low or moderate physical activity intensity in T0 significantly improved TUG time(U=18.00,P=0.020).

Table 2 Pre-and post-intervention outcomes of the kyphosis angle (two postures) and five physical tests(n=20).
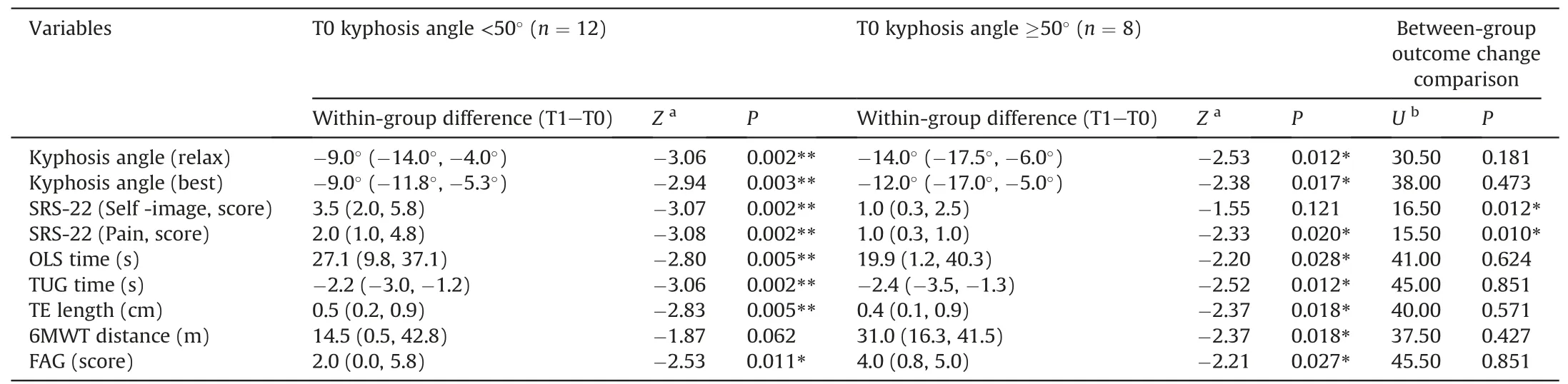
Table 3 Comparison of pre-and post-intervention outcomes between participants with different pre-intervention kyphosis angles.
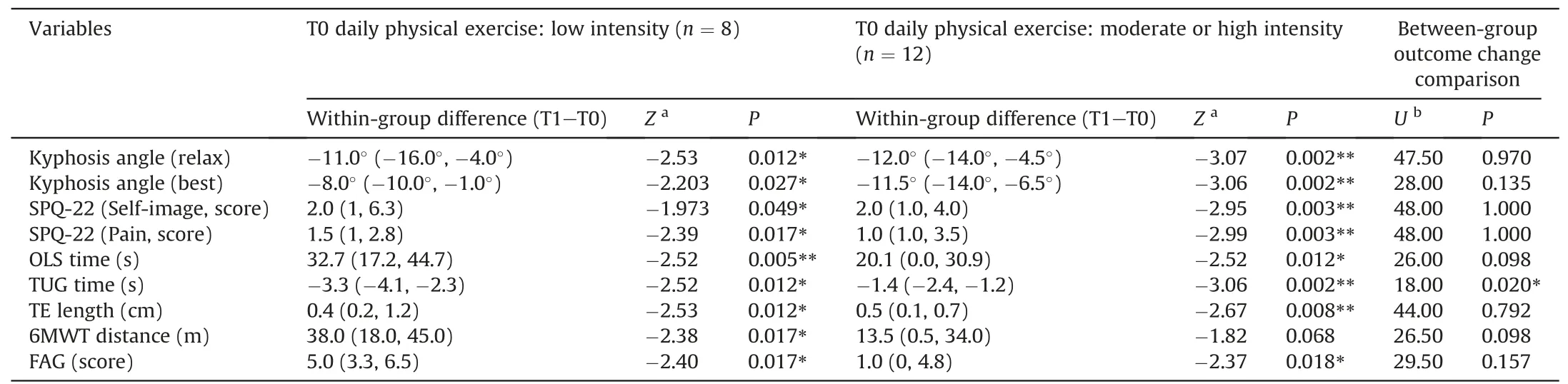
Table 4 Comparison of pre-and post-intervention outcomes between participants with different pre-intervention exercise levels.
4.Discussion
We modified the kyphosis-specific exercises from Katzman et al.[20,27]for home-based use,compressing the intervention period to six weeks,increasing the content of home practice,and providing a tutorial video for guidance.Following the intervention,all 20 participants exhibited a significant reduction in kyphosis angle in two standing postures,less pain,improved self-image,and enhanced balance,cardiopulmonary,and gait performance.The short-term home practice adherence rate was >90% by the number of days and >76% by practice time.
4.1.Potential of home-based kyphosis-specific exercise as an effective intervention for older adults
Our study found large effect sizes(0.89 and 0.85)for the changein kyphosis angles in both relaxed and the best standing postures.Previous studies using Katzman and team intervention reported smaller effect sizes(Cohen’s d=0.60 and 0.68)[12,21].However,a full-size RCT was needed to confirm the effects of our modified intervention program.Additionally,the kyphosis angles in both standing postures,40.0°(34.5°,43.5°)and 30.0°(22.5°,34.0°),were in the normal range at T1 [1],indicating the clinically meaningful potential for participants to return to normal kyphosis angles.The adherence rates of our study were 100% in center-based exercise classes and 94.3% (evaluated by days) to 76.7% (evaluated by practicing time)in home practice.Class adherence was higher than 84%and 75%,and home practice adherence was comparable to 78%and 72%,as reported in Katzman’s 3-month and 6-month intervention programs[12,21].The previous studies reported 5-6%drop-out rates[12,21],while our study had no drop-outs.95%,55%,and 30%of the participants continued practicing the exercise in the 1st,3rd,and 15th months after the intervention,showing longterm feasibility.
Our study included older adults with or without regular exercises,unlike previous kyphosis-specific exercise trials,which excluded such individuals [12,20-22].The results demonstrated significant improvements in kyphosis angle,self-image,pain,and physical performance,regardless of exercise habits.In China,older adults mainly perform aerobic exercises,such as square dance,Taichi,and brisk walking,but may lack systematic stretching,fullbody mobility,and flexibility training.Therefore,home-based kyphosis-specific exercises may be particularly beneficial for Chinese older adults as it comprehensively trained muscle strength,spine alignment,and full body mobility and flexibility.In addition,this result alerted the nurses that when conducting the health assessment or making a health promotion plan for older adults,we should consider the intensity/duration of physical exercise and the diversity of practice.Nevertheless,compared with the low daily physical activity intensity participants,those with moderate or high intensity showed significantly less improvement in the TUG test.This could be because the participants with moderate or high intensity already performed significantly better (P=0.025) at preintervention than those with low intensity.
In addition,the intervention positively affected all outcomes in subgroups with different pre-intervention hyperkyphosis angles,except for those with pre-intervention kyphosis angles ≥50°who did not show a significant change in self-image.The two subgroups did not show a significant difference in terms of the improvement in outcomes,except for self-image and pain.Participants with ≥50°kyphosis angle reported having less pain at pre-intervention,which was contradictory to the previous finding that people with more severe thoracic hyperkyphosis have more pain [4].This was probably because older adults with severe thoracic hyperkyphosis and bad pain were less likely to join the exercise intervention.Thus,participants with kyphosis angle ≥50°in our study had mild or no pain.Severe thoracic hyperkyphosis is strongly associated with body-image(r=0.951,P=0.008)that affects self-image[48,49].As the psychological intervention effectively improves body image[50],along with home-based kyphosis-specific exercises,we suggest people with severe thoracic hyperkyphosis may also need psychological intervention.Overall,our study indicates that the home-based kyphosis-specific exercise intervention can benefit older adults with or without regular exercise habits and with varying degrees of hyperkyphosis.
This intervention reduced the transportation time required for frequent center-based group classes and ensured safety and suitability for home practice.Limited participants per group class ensured higher study quality and safety.The exercises predominantly involved stable postures,such as supine,prone,quadruped,two-legs standing,and using bodyweight or easily accessible equipment,like an elastic band and yoga mat.Home-based kyphosis-specific exercises had additional benefits of meeting the WHO’s recommendation of weekly 300 min of moderate-intensity aerobic physical activity and ≥2 days of muscle-strengthening activities for older adults [51].Our intervention attained moderate intensity,as measured by Mayo Clinic’s physical activity intensity subjective measuring standard [52],and included both aerobic and muscle-strengthening exercises.
4.2.Possible mechanism of the intervention
Katzman et al.conducted two RCTs where x-ray measured kyphosis angle changes were significant six months postintervention.In contrast,body surface measured kyphosis angle changes were significant at six and three months post-intervention[12,21],implying that posture alignment may initially be contributed by muscle strength,flexibility,and spine mobility improvement before progressing to spine structure change.As our study intervention period was six weeks and the kyphosis angle was measured by body surface,the posture alignment might be contributed by muscle strength,flexibility,and spine mobility improvement[12,21].Although the 22 exercises in our intervention were grouped into five sections according to their main contribution,each exercise may contribute to one or more of the three dimensions: enhancing muscle strength,increasing alignment awareness and posture stability,and increasing spine mobility and muscle flexibility.Among all 22 exercises,those strength exercises using body weight or external resistance targeting core muscles,including abdominal wall muscles,back muscles,and diaphragm muscles)and limb muscles were contributing to enhanced muscle strength (dimension 1) [53,54].
Furthermore,practicing core muscles can enhance muscle awareness and improve core stability [55,56],further benefit posture alignment awareness and posture stability (dimension 2)[57,58],increase physical performance [59],and reduce back pain[60].Exercises targeting lower extremity muscles can also benefit posture stability and physical performance [54,61].For dimension 3,the training targets increasing upper extremity muscles and shoulder mobility to contribute to scapular alignment,which is associated with spinal alignment [35,36].The exercises increase spine mobility,and muscle flexibility can reduce the obstacles of spine extension and thoracic extension [62],which will further benefit obtaining alignment posture and enhance cardiopulmonary function [63].Further study may need to reveal the mechanism of posture alignment progress.
4.3.Scope for intervention improvement
Participants’ feedback revealed that there is potential to increase compliance with the daily home practice in our intervention.Participants had difficulty completing the 1-h practice in one continuous session due to unavoidable household duties,resulting in fragmented practice sessions of less than an hour [28].Participants suggested splitting the video into shorter clips to facilitate home practice.As participants in our study practiced 76.7%of home practice time,practiced in fragmented time,and showed significant improvements,it suggested home practice might still be advantageous after being split into multiple shorter sessions.In a future study,we can divide the home practice into several sessions according to the exercise aim.Since some participants did not continue the practice for the main reasons of unchanged exercise content and worrying about practice accuracy,we may consider increasing exercise diversity and developing an online platform in a future project to boost long-term adherence.For example,we may conduct evidence-based research to create a thoracic hyperkyphosis correction exercises library,provide practice videos to online platforms such as WeChat applets,and set up an online enquiry service to reduce doubts when practicing at home.
4.4.Strength and limitations
This study demonstrated nurses’experience modifying previous exercise interventions according to targeted participants' needs.The design of the current intervention adopted a home-based approach to suit older Chinese adults.Meanwhile,the benefits of this home-based kyphosis-specific intervention were objectively measured,and qualitative feedback was also collected to inform further modification of the intervention.After performing a fullscale randomized controlled trial,it may also be promoted to older adults in other countries having difficulties visiting healthcare facilities frequently.
This study had several limitations.First,the gold standard radiation imaging test was not used to measure the kyphosis angle.However,the manual inclinometer was acceptable,providing satisfactory validity and reliability [37,38].We also avoided unnecessary radiation exposure in our participants.Second,this study had a small sample size and no control group.The effectiveness of the study could not be established unless a randomized controlled trial with an adequate sample size was conducted.Third,this study lacked long-term follow-up and kinematic analysis,which may be considered in future randomized controlled trials.
5.Conclusions
This study proposed 6-week home-based kyphosis-specific exercises and showed its possibility of being a feasible and advantageous intervention.Regardless of participants’ daily physical exercise habits,the participants showed a potential reduction in hyperkyphosis angle and improvement of physical performance after receiving the intervention.A randomized controlled trial with an adequate sample size should be considered in the future.
CRediT authorship contribution statement
Wei Ying Li: Conceptualization,Methodology,Investigation,Writing-original draft,Writing-review &editing,Resources.Jinling Lu: Conceptualization,Methodology,Investigation,Writingoriginal draft,Writing-review &editing,Resources.Yong Dai:Conceptualization,Methodology,Investigation,Writing-original draft,Writing-review &editing.Agnes Tiwari: Conceptualization,Methodology,Investigation,Writing-original draft,Writing-review&editing,Project administration,Supervision.Pui Hing Chau:Conceptualization,Methodology,Investigation,Writing-original draft,Writing-review &editing,Resources,Project administration,Supervision.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author (Wei Ying Li) upon reasonable request.
Declaration of competing interest
The authors declare no conflict of interest.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2023.03.007.
杂志排行

International Journal of Nursing Sciences的其它文章
- Development and validation of dynamic nomogram of frailty risk for older patients hospitalized with heart failure
- Validation of the Portuguese version of the social isolation scale with a sample of community-dwelling older adults
- Effects of pre-operative education tailored to information-seeking styles on pre-operative anxiety and depression among patients undergoing percutaneous coronary intervention: A randomized controlled trial
- Factors influencing the quality of sexual life in the older adults: A scoping review
- Comparison of the effects of three kinds of hand exercises on improving limb function in patients after transradial cardiac catheterization
- The trajectories of physical growth in 4 months postnatal corrected age among preterm infants discharged from neonatal intensive care units and associated factors: A prospective study