Predictive factors based on the health belief model on cancerscreening behaviour in first degree relatives of patients with Lynch syndrome-associated colorectal cancer
2023-05-14JiojioGuShuminJiHuxingChoTinglnChenXiodnWu
Jiojio Gu ,Shumin Ji ,Huxing Cho ,Tingln Chen ,Xiodn Wu ,*
a The Third Affiliated Hospital,Sun Yat-Sen University,Guangzhou,China
b Li Ka Shing Faculty of Medicine,The University of Hong Kong,Hong Kong,China
c State Key Laboratory of Oncology in South China,Collaborative Innovation Center for Cancer Medicine,Sun Yat-sen University Cancer Center,Guangzhou,China
Keywords: Behaviour Family Health belief Hereditary nonpolyposis colorectal neoplasms Knowledge
ABSTRACT Objectives: This study aimed to investigate colorectal cancer-related knowledge,health beliefs,and screening behaviour in first-degree relatives (FDRs) of patients with Lynch syndrome-associated colorectal cancer (CRC) and explore the predictive factors of screening behaviour based on a health belief model.Methods:This cross-sectional study was conducted in the colorectal department of a Class A tertiary hospital in Guangzhou from December 2017 to December 2019.A total of 265 FDRs of 96 patients with Lynch syndrome-related CRC were selected.The study was conducted in the colorectal department of a tertiary cancer centre in Guangzhou.The demographic questionnaire,the simplified CRC knowledge questionnaire,and the Champion’s Health Belief Model Scale were used for evaluation.Data were analyzed using statistical description,between-group comparisons,and binary logistic regression.Results:A total of 160(60.4%),61(23.0%),and 44(16.6%)of the participants had high,medium,and low levels of knowledge about CRC,respectively;the average overall score of health belief was 121.36±13.02.Sixty-one participants (23.0%) underwent Lynch syndrome-associated cancer screening.The predictive factors of screening behaviour included sex (male),age (older),married status (married),multiple primary cancers of the index patients,and high levels of knowledge and health beliefs (P <0.05).Conclusions:The knowledge and health beliefs of cancer and cancer screening in FDRs of patients with Lynch syndrome-associated CRC should be improved.Both knowledge and beliefs are critical in promoting their cancer screening behaviour.Interventions should focus on health education and enhance health beliefs of the FDRs for better screening behaviour.
What is known?
·The first-degree relatives (FDRs) of patients with Lynch syndrome-associated colorectal cancer (CRC) have a 50% probability of carrying the same pathogenic genes and a high risk of developing Lynch syndrome-associated cancer.
·Screening is a recommended,simple and effective method for early diagnosis and to improve cancer prognosis.As a personal health behaviour,patients’ cancer screening can be influenced by health beliefs and health knowledge.
What is new?
·Approximately 40%of the participants had a moderate/low level of CRC knowledge,the mean score of health belief was at a medium level,and less than a quarter had a screening for Lynch syndrome-associated cancer,which is relatively low.
·Knowledge,health beliefs,age,sex,diagnosis of index patients,and marital status were predictive factors of screening behaviour in FDRs of Lynch syndrome-associated CRC patients.Interventions targeting the above intervenable factors to improve FDRs’ screening behaviour are recommended.
1.Introduction
Colorectal cancer (CRC) is the third most commonly diagnosed cancer,accounting for 9.8% of cancer cases.It is also the second most common cause of death in cancer patients,accounting for 9.2% of cancer deaths [1-3].The pathogenesis of nearly 10% of patients with CRC is related to genetic factors,i.e.,hereditary colorectal cancer,and Lynch syndrome-associated CRC is the most common form [4,5].Lynch syndrome accounts for approximately 3% of all CRC cases [6],affecting 1 in 279 people in the general population[7].The first-degree relatives(FDRs,a person’s parents,children,and siblings from the same father or mother) of patients with Lynch syndrome-associated CRC have a 50% probability of carrying the same pathogenic genes.Therefore,they comprise a high-risk group for Lynch syndrome-associated cancer,which primarily includes CRC,endometrial cancer,and other neoplasms of the urinary tract and stomach [8].Screening is a recommended,simple and effective method to diagnose cancer early and improve its prognosis[9],particularly for people with hereditary cancer risk[9-11].Promoting cancer screening in FDRs of patients with Lynch syndrome-associated CRC is a highly targeted,efficient,and simple method for preventing and controlling Lynch syndrome-associated cancers.Cancer screening reduces the incidence of CRC by 62% and the mortality rate by 65% in people with hereditary cancer syndromes[12].
Early screening and diagnosis substantially improve the prognosis.However,most patients with CRC delay visiting a doctor even after developing symptoms.Therefore,their first diagnosis often occurs in the middle or late stages,adversely affecting the prognosis[13].A similar situation occurs in people with a strong family history of cancer[13-15].Studies on the screening behaviour of the relatives of CRC patients outside China found better screening compliance in people with a family history of CRC than in common residents.Nevertheless,the degree was far from expectations[16,17].A total of 22%-49% of the blood relatives of CRC patients were screened for CRC in Australia,Victoria,and Singapore[17,18].Because of the genetic characteristics of Lynch syndromeassociated CRC,FDRs face a significantly increased risk of cancer and earlier onset.Relevant guidelines suggest more frequent and earlier cancer screening in FDRs of patients with Lynch syndromeassociated CRC and multiorgan tumour screening[10,13].However,to our knowledge,few studies have investigated the FDRs of patients with Lynch syndrome-associated CRC in China.Even largescale systematic studies on the blood relatives of Lynch syndrome-associated CRC patients are rare worldwide.Therefore,investigating cancer screening behaviour and its predictive factors in the FDRs of patients with Lynch syndrome-associated CRC may help prevent Lynch syndrome-associated cancers.
Similar to healthy behaviour,screening behaviour is related to various factors,such as age,sex,financial burden,healthcare system-and provider-related factors,knowledge of the disease,and health beliefs.The present study was guided by the Health Belief Model(HBM),proposed by Hochbaurm in 1958[19].HBM has been widely used in explaining cancer screening behaviour,and a systematic review concluded that HBM showed satisfying predictive effects [20].As a cognitive model,the HBM emphasizes how individuals rationalize their behaviours in nonspecific social contexts.It contributed substantially to predictions of whether individuals adopt healthy behaviours,such as prevention,screening,and disease control [21].According to this theory,behaviour is related to perceived susceptibility,severity,barriers,benefits,self-efficacy,cues to action,and sociodemographic factors.Health belief,the core concept in HBM,is summarized in two aspects: how an individual perceives a threat to health and how an individual perceives whether a certain health behaviour will effectively mitigate the threat [22].Individuals with high health beliefs tend to adopt healthy behaviours [23].For the FDRs of patients with Lynch syndrome-associated CRC,health beliefs reflect their knowledge and perception of the disease,screening methods,and confidence to achieve change via these actions.Therefore,an individual’s health beliefs and knowledge markedly influence cancer screening as a personal health behaviour [16].A broader sociocultural environment is critical for building beliefs and promoting favorable actions to prevent cancer[24,25].Nurses play an important role in the prevention of cancer.In the context of China,where social cancer screening services and cancer awareness events are insufficient,it is imperative to understand more about FDRs’ screening behaviour,related knowledge,and health beliefs so that it can help doctors and nurses provide personalized health education and reduce the burden of cancer.Therefore,the present study explored the effects of knowledge,health beliefs,screening behaviour,and its predictive factors in FDRs of Lynch syndrome-associated CRC to promote cancer prevention.
2.Methods
2.1.Study design and participants
A cross-sectional study was conducted at the colorectal department of a Class A tertiary care hospital in Guangzhou,Guangdong Province,China.The following inclusion criteria were used for the participants: 1) FDRs (parents,children,and siblings from the same father or mother) of patients who were diagnosed with Lynch syndrome-associated CRC;2) age ≥18 years;3) ability to communicate,read and comprehend;and 4)will to participate in the research.People with a history of malignant tumours or mental illness were excluded from the present study.The sample size was calculated by the sample size calculation formula for multiple linear regression embedded in PASS 14 software (power analysis and sample size):n=(4*[(Zα/2+Zβ)/ln((1+ρ)/(1-ρ))]2+3)/(1-).In this formula,ρ stands for the correlation between health belief and screening behaviour,and referring to the results of a previous study,ρ=0.283,=0.432 [26],α=0.05,β=0.1,so by calculation,we obtainn=157.Considering a 10%invalid sample,the minimum sample-size was determined to be 175 cases,and a sample of 265 participants was collected for our study.
2.2.Instruments
2.2.1.General information questionnaire
Researchers designed the general information questionnaire based on a literature review [15,18].It included information about the FDRs: age,chronic disease,education level,marital status,patient’s diagnosis index,and relationship with the index patients.
2.2.2.Screening behaviour
The FDRs of Lynch syndrome-associated CRC patients are at high risk of Lynch syndrome-associated cancer.The “screening behaviour”mentioned in this study refers to CRC screening and includes endometrial,urinary,and gastric cancer[8].Therefore,participants were asked whether they underwent screening for any of these cancers in the questionnaire.They were also requested orally about their past cancer screening examination to ensure the fidelity of the data.
2.2.3.Questionnaire on knowledge of CRC and screening
This questionnaire was revised based on the Chinese University of Hong Kong’s Colorectal Cancer Knowledge Questionnaire[27,28]with some contents simplified,mainly about the factors of Lynch syndrome-associated CRC,to suit the families of patients with Lynch syndrome-associated CRC.It assessed the participants’knowledge of CRC and screening.The knowledge portion of the questionnaire included four aspects: disease symptoms,diseaserelated factors,diagnostic methods,and the best strategy for early diagnosis [27].The options included 9 symptoms,12 factors related to CRC,and 6 main examination methods.When the participants knew at least one of the options for each aspect (i.e.,symptom,related factor,or examination method),they scored 1.Knowledge was divided into 3 levels:1)high-level:knowledge of 4 aspects;2) medium level: knowledge of 3 aspects;and 3) lowlevel: other scores.The questionnaire had good reliability and validity with a Cronbach’s α coefficient of 0.801 and a test-retest reliability of 0.758 [29].We collected 80 questionnaires for a preexperiment,and the results of the pre-experiment showed that Cronbach’s α coefficient calculated was 0.88,and the Cronbach’s α coefficient in our study was 0.789.
2.2.4.Champion’s Health Belief Model Scale (CHBMS)
The original versions of the CHBMS were developed by Jacobs based on the HBM to measure the participants’ health beliefs[30,33].The 36-item scale comprised the following 6 dimensions:perceived susceptibility to Lynch syndrome-associated cancer (5 items);perceived severity of Lynch syndrome-associated cancer(7 items);perceived benefits of screening(6 items);perceived barriers to screening (6 items);health motivation (7 items);and selfefficacy of screening (5 items).All items were rated using a 5-point Likert scale that ranged from 1 (completely disagree) to 5(completely agree),except for the dimension of perceived barrier,which was reversely scored from 5 (completely disagree) to 1(completely agree).Scores of relevant items were summed to calculate the total score of each dimension and the whole scale.Higher scores indicate higher patients’ beliefs in health behaviour[18,31,32].In this study,the Chinese version of the CHBMS showed good reliability,with Cronbach’s α coefficients of 0.881 for the total scale and 0.801 to 0.944 for the 6 dimensions.
2.3.Data collection
The investigator distributed questionnaires to participants at the hospital site from December 2017 to December 2019.Before the survey,we explained the study’s purpose,significance,and confidentiality and guided participants with unified language.The participants signed informed consent forms and completed the questionnaires within 15 min.The questionnaires were collected on the spot,and the researcher checked the quality of the questionnaires and promptly confirmed with the study participants for any missing entries and instructed them to fill them in.Participants could withdraw at any time.
2.4.Data a nalysis
Statistical analyses were performed using SPSS version 20.0(SPSS Inc.,USA).Continuous variables were described by mean and standard deviation,and categorical variables were described by frequency and percentage.Data were analyzed using the chi-square test,two independent samplet-test,and binary logistic regression.Chi-square tests,Ztests,and independent samplettests were used to explore the associations among knowledge,health beliefs,demographic data,disease-related data,and cancer screening behaviour.Additionally,we used logistic regression analysis to explore the main predictors of screening behaviour in FDRs of patients with CRC associated with Lynch syndrome.Whether participants underwent screening for Lynch syndrome-associated cancers was considered the dependent variable,and variables with statistical significance (P<0.05) in single-factor analysis were considered independent variables in binary logistic regression analysis.
2.5.Ethical considerations
Ethical approval was granted by the clinical research ethics committee of Sun Yat-sen University Cancer Center(no.GYX-2019-017).All the participants were reassured that their care would not be affected by a rejective decision or withdrawal at any time.All the completed forms were placed in sealed envelopes and stored in a secure place accessible only to the researcher.The data were used for the present study only and will be disregarded once the results are published.
3.Results
3.1.Demographic characteristics of participants
The average age of 96 index patients was 49.95 ± 11.63 years(14-73 years).The average age of 265 FDRs of the patients with Lynch syndrome-associated CRC was 35.89 ± 12.99 years (18-75 years).Among the participants’ families,2 to 8 relatives had been diagnosed with CRC.The youngest patient diagnosed with CRC in each family ranged from 14 to 59 years,and the average age was 44.01 ±10.83 years.
3.2.Knowledge,health beliefs,and screening behaviour of the FDRs of patients with Lynch syndrome-associated CRC
A total of 160(60.4%)participants had high CRC knowledge.The average score for health beliefs was at the medium level(121.36 ± 13.02).Sixty-one (23.0%) participants had undergone Lynch syndrome-associated cancer screening.All of these participants were screened for CRC,and some of them were screened for endometrial cancer (n=25),urinary system cancer (n=27),or gastric cancer (n=36).The details are shown below(Table 1).
3.3.Screening behaviour of participants with different characteristics
Health beliefs,self-efficacy (P<0.001),perceived susceptibility(P=0.008),perceived benefits (P<0.001),and health motivation(P=0.024) were significantly different between participants who underwent cancer screening and participants who did not.Age,education level,marital status,chronic disease status,and index patient’s diagnosis were significantly associated with screening behaviour (Table 2).
3.4.Influencing factors of screening behaviour among participants
Logistic regression analysis found that diagnosis of the index patient,knowledge level,health beliefs,age,sex,and marital status predicted screening behaviour (Table 3).
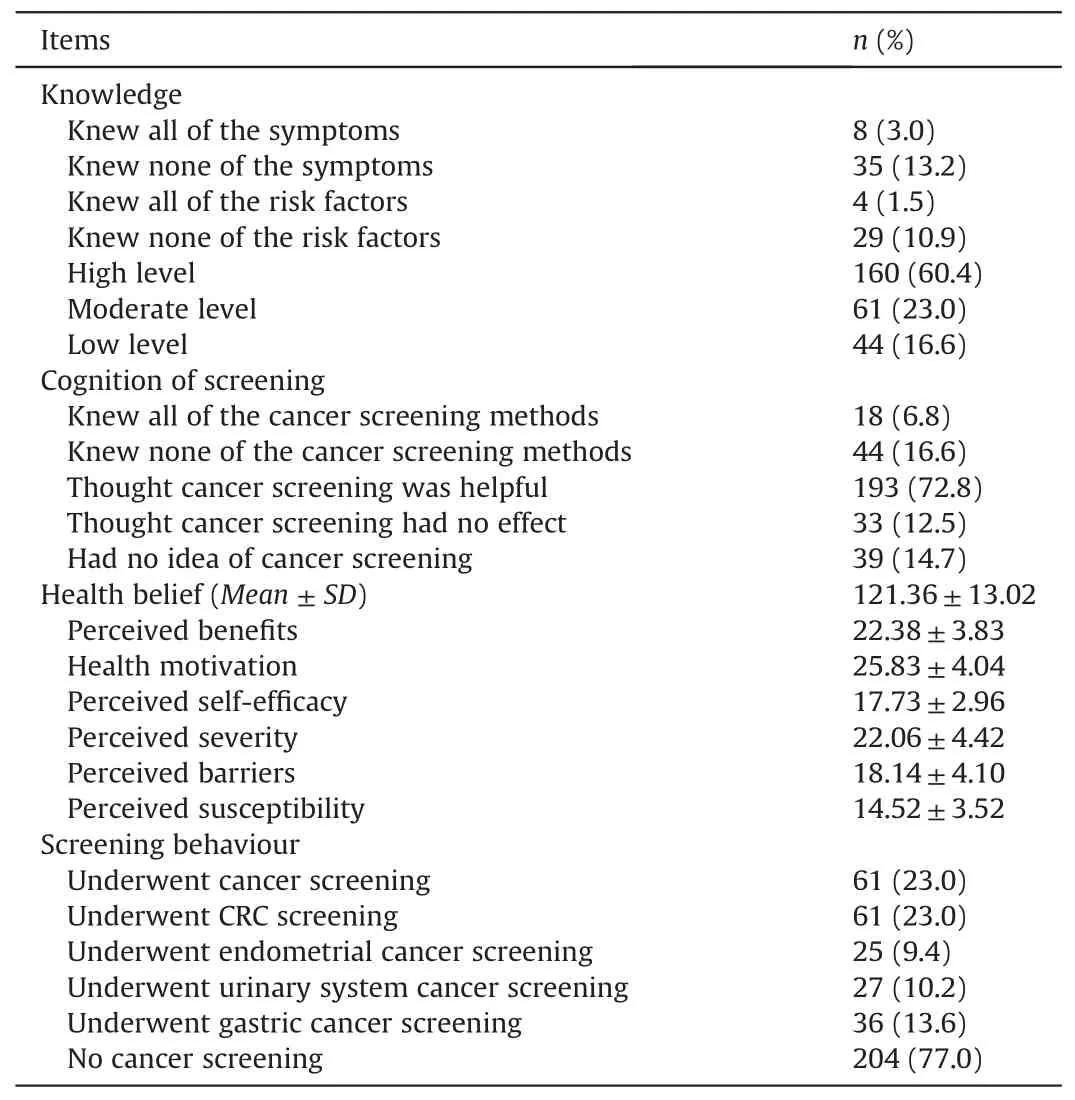
Table 1 Knowledge,health beliefs,and screening behaviour of the participants (n=265).
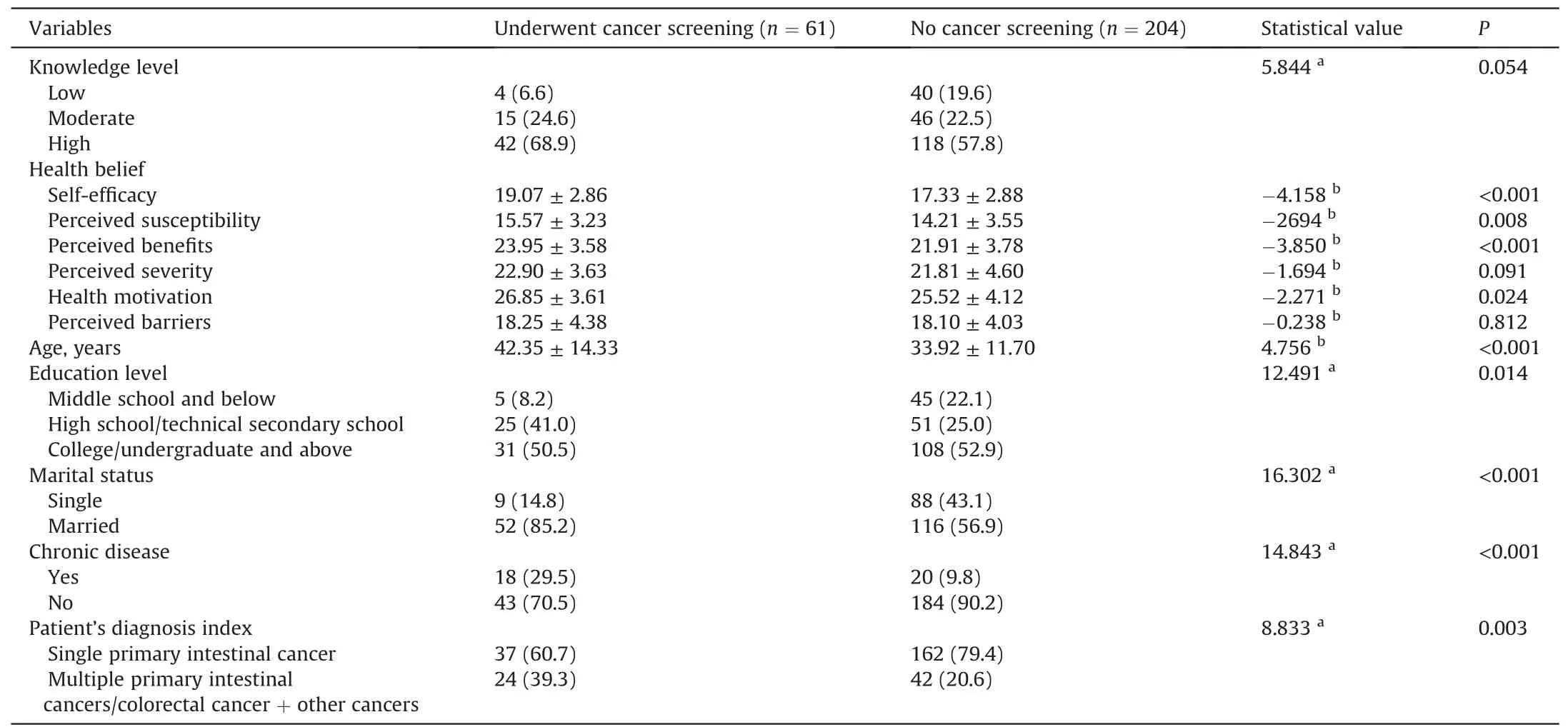
Table 2 Screening behaviour of participants with different characteristics (n=265).
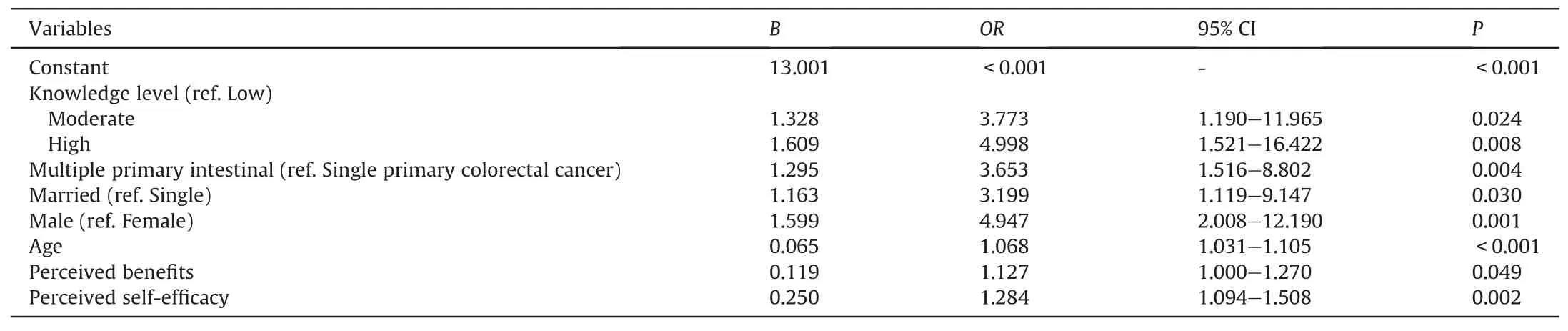
Table 3 Logistic regression analysis of participant screening behaviour.
4.Discussion
This study revealed that the FDRs of patients with Lynch syndrome-associated CRC had a relatively low level of knowledge.With a deeper understanding of the relationship between knowledge and behaviour and increased attention to CRC screening inrecent years,CRC knowledge investigations have gradually increased [28].However,targeted research on CRC knowledge is lacking in FDRs of patients with Lynch syndrome-associated CRC in China.Domestic scholars have shown that the knowledge level of CRC in common residents is generally low [14].A total of 16.6% of participants in this study had a low level of knowledge,which indicates that knowledge of the FDRs of patients with Lynch syndrome-associated CRC was not sufficient [34-36].A heavy clinical workload makes medical staff ineffective in communication,education,and resource sharing for patients and their families.However,patients,their families,and medical personnel may lack professional knowledge and an understanding of the characteristics of Lynch syndrome and focus little on CRC knowledge.Therefore,knowledge about CRC should be popularized.It also suggests that,in the future,the state should increase resources in healthcare and reduce the burden on clinical nurses to provide effective support for them to improve the knowledge of patients and families.
The mean total score of health belief in this study sample was at a medium level,between the second and third quartile of the total score range,suggesting that the participants’ health beliefs were temporarily ambiguous and had not formed clear attitudes or beliefs.The data from the study indicated slightly higher levels of health beliefs in our study than the FDRs of CRC patients in Turkey[18].The reasons for this difference may be that the participants in the present study were relatives of patients with hereditary CRC,with more diagnosed cancer patients in their family and more information about CRC cancer,and younger participants could easily gain more information about CRC and screening via diversified media [24,37].People with more information about CRC and screening reported higher health beliefs [18,32].However,the health belief levels of the participants in the present study were lower than those over 50,as Kharameh [38] and Tastan [33] reported.This difference may be due to the lack of awareness of CRC in the Chinese context and the incomplete distribution of social cancer screening services.A broader sociocultural environment is critical for building beliefs and promoting favorable actions to prevent and detect LS-associated cancer at an early stage [24,25].Therefore,more efforts are needed to improve the health beliefs of cancer screening.
The results showed that 61 participants(23.0%)received cancer screening.This overall screening rate is similar to a previous study on common residents in China[34].Although the participants faced a higher risk of cancer than the general population,their screening behaviour was suboptimal.A low screening rate may be related toparticipants being younger than the routine recommended cancer screening age.Participants in this study were at high risk of CRC and other associated cancers.Only CRC was chosen for testing for the screened participants,and some of these participants neglected other cancers.One potential reason for this is incomplete or invalid education by healthcare professionals.Some participants may falsely believe that they were only susceptible to CRC.Therefore,the characteristics of Lynch syndrome-associated CRC must be popularized,and cancer screening in young FDRs must receive increased attention.
The identified predictive factors of screening behaviour included knowledge,health beliefs,age,sex,diagnosis of index patients,and marital status in the present study.People with high levels of knowledge,perception of screening benefits,and selfefficacy,male,older or married,and related to index patients diagnosed with multiple primary CRCs or extraintestinal cancer were more likely to accept cancer screening.
Consistent with our findings,previous studies concluded that high knowledge and health belief levels contributed to understanding the disease risk,self-efficacy of cancer screening,and observation towards healthy behaviour,which promote cancer screening behaviour [35,38,39].Knowing more and correct information is the premise of forming clear and strong health beliefs in cancer screening.In addition to objective factors,such as knowledge,behaviours are substantially influenced by subjective factors.Health beliefs emphasize personal perception,exhibit individual psychological characteristics,and explain and predict healthrelated behaviours to a large extent [22,37].Health behaviours are more likely to occur when individuals perceive the disease severity,believe in the likelihood of adverse outcomes,and believe in the benefits of adopting healthy behaviours and that the costs are small.Health motivation,also known as cues to action,becomes the last promoter of behaviour in the process.In theory,each component of the HBM contributes substantially to health behaviour.However,this relationship is only sometimes completely corroborated in practice.Only two domains of health belief predicted screening behaviour in the present study: perceived benefits and self-efficacy.In a systematic review summarizing the predictive effects of health beliefs on CRC screening in the general population,some of the included studies tested each component of health beliefs.The most commonly demonstrated beliefs were perceived benefits and susceptibility [20].Although the other domains of health belief were not entered in the final regression model,most domains were significantly different between participants who received cancer screening and those who did not.Therefore,the HBM is valuable in guiding interventions to promote cancer screening.Notably,health education should target perceived benefits and self-efficacy in FDRs of patients with Lynch syndromeassociated CRC.
Male participants were more likely to screen for cancer than female participants.This finding was consistent with a populationbased study performed in FDRs of CRC patients [33].This consistency is likely because of public awareness that men have a higher risk of relevant cancers(colorectal cancer and gastric cancer)than women and women’s greater fear of possible discomfort and complications from screening methods [34,36,39].Patients with multiple and metastatic CRCs and their families generally receive more screening recommendations from their doctors.Studies in China and abroad found that obtaining screening advice from doctors correlated with the positive acceptance of screening[34,39].Compared to unmarried individuals,married participants tended to be encouraged by their spouses and other family members to undergo cancer screening.The risk of cancer increases with age.The mean age of participants screened for cancer was 43 years,ten years older than participants who did not receive screening.Guidelines suggest that people older than 45 should be a priority group for CRC screening[35,37].The refusal of younger relatives to undergo screening may be related to a lack of awareness of the high risk of hereditary CRC[38].However,because of the early onset of hereditary intestinal cancer,more attention should be given to younger FDRs.
This study described the knowledge,beliefs,and screening behaviour in FDRs of patients with Lynch syndrome-associated CRC in China,which has rarely been studied before.The present study confirmed the predictive effects of knowledge and health beliefs on cancer-screening behaviour and provided targeted direction for future intervention.For example,in the area of nursing,clinical staff could strengthen information sharing on Lynch syndromeassociated CRC,call for centralized education in FDRs,and communicate via social media platforms,such as WeChat,focusing on women,younger people,unmarried relatives,and index patients with single CRC.
5.Limitations
There were some limitations in this study.First,this study was an exploratory cross-sectional design with no way to determine causality,and future prospective dynamic follow-up studies should be conducted.Second,participants were sampled from only one hospital,limiting the generalizability of the results.Multicentre follow-up studies with large sample sizes should be considered in the future.Third,we did not consider the effect of clustering from the same family.A screening support system was not included in the predicting factors,which may have a certain predictive effect on screening behaviour.However,free screening is currently available in some areas.Therefore,the role of family and environmental factors must be considered in the future.
6.Conclusion
Diagnosis of the index patient,knowledge level,health beliefs,age,sex,and marital status were predictive factors of screening behaviour in FDRs of Lynch syndrome-associated CRC patients.The knowledge and health beliefs of cancer and cancer screening in FDRs of patients with Lynch syndrome-associated CRC must be improved.Both knowledge and beliefs are critical in promoting cancer screening behaviour.Interventions should focus on health education and enhance health beliefs for better screening behaviour.
Funding
Medical Research Fund of Guangdong Province(A2019004).The funding organization has not attended the survey’s design,implementation,and analysis.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
CRediT authorship contribution statement
Jiaojiao Gu:Conceptualization,Methodology,Writing-original draft.Shumin Jia: Resources,Formal analysis.Huaxiang Chao:Data curation,Investigation.Tinglan Chen:Data curation,Writingoriginal draft.Xiaodan Wu: Conceptualization,Supervision,Writing -review &editing.
Declaration of competing interest
The authors have declared no conflict of interest.
Acknowledgments
Our gratitude goes out to the nurses in the hospitals for their assistance in data collection,and to all the colorectal cancer survivors and their relatives who took part in the study.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2023.03.013.
杂志排行

International Journal of Nursing Sciences的其它文章
- A feasibility study on home-based kyphosis-specific exercises on reducing thoracic hyperkyphosis in older adults
- Development and validation of dynamic nomogram of frailty risk for older patients hospitalized with heart failure
- Validation of the Portuguese version of the social isolation scale with a sample of community-dwelling older adults
- Effects of pre-operative education tailored to information-seeking styles on pre-operative anxiety and depression among patients undergoing percutaneous coronary intervention: A randomized controlled trial
- Factors influencing the quality of sexual life in the older adults: A scoping review
- Comparison of the effects of three kinds of hand exercises on improving limb function in patients after transradial cardiac catheterization