Development and psychometric testing of a competency of nursing process questionnaire
2023-05-14ViryaKoyJintanaYunibhanAnrewRauthNiholasBirherManilaPrakRiharHenker
Virya Koy ,Jintana Yunibhan ,Anrew Rauth ,Niholas Birher ,Manila Prak ,Rihar Henker
a Faculty of Nursing,Chulalongkorn University,Bangkok,Thailand
b Department of Hospital Services,Ministry of Health,Phnom Penh,Cambodia
cSchool of Nursing,University of Pittsburgh,Pittsburgh,PA,USA
d Cambodian Association of Nurses,Phnom Penh,Cambodia
Keywords: Cambodia Competency Development Nursing process Psychometric testing
ABSTRACT Objectives: This study aimed to develop and evaluate a competency of nursing process questionnaire(CNPQ) for registered nurses in Cambodia.Methods:Guided by the nursing process,an initial questionnaire was generated through focus group discussion,literature review,and the expert consultation.Finally,the validity and reliability of the questionnaire were validated through a questionnaire survey online of 260 registered nurses selected from Complimentary Package Activities 1,2,3,and national hospitals from January to February 2022 in five geographic areas of Cambodia.Results:The content validity index was 1.00.The Cronbach’s α coefficient for the whole questionnaire was 0.963,and the range for the five dimensions was 0.963-0.964,which shows that the questions were consistent.The test-retest reliability was 0.769.The exploratory factor analysis led to a list of 24 items that were grouped into five dimensions: assessment,diagnosis,planning,implementation,and evaluation.The cumulative variance contribution rate was 70.08%.Conclusions:The CNPQ developed in this study showed good reliability and validity and can be used to assess the competency of registered nurses by themselves and help nursing managers to develop the relevant policies.
What is known?
·The five steps of the nursing process have been implemented globally.
·Competency of the nursing process improves outcomes in critical illness,patient well-being,nursing care quality,and patient safety.
What is new?
·This study developed the Competency of Nursing Process Questionnaire (CNPQ) and proved its reliability and validity.
·The CNPQ can help registered nurses evaluate their skills and provide baseline data that can be used to help spread best practices.
1.Introduction
Nursing competency comprises the core abilities required to fulfill the role of a nurse.Therefore,it is essential to define nursing competency to develop a principle for the nursing education curriculum.In addition,nursing competency is vital for improving care quality and patient safety[1].Moreover,the registered nurses’core competence has been attributed to the ability to apply knowledge,attitudes,and skills that enable them to exercise efficiently and effectively [2].Evaluating nursing competency is an essential step in clinical practice and may not overestimate as a proper clinical competency assessment negatively affects patients’ outcomes [3].In recent years,surgical procedures have encountered heavy changes because of increasingly advanced technologies,the complexity of diseases,and advanced medical equipment.Therefore,assessing nursing competency based on validated and reliable questionnaires is necessary for complex surgical situations [4].
The nursing process is fundamental to professionalism in modern nursing practice.This analytical method uses scientific reasoning,critical thinking,and problem-solving to guide nurses in providing effective patient care [5].It includes five steps: 1)assessment,2) diagnosis,3) planning,4) implementation,and 5)evaluation [6].Numerous studies have provided strong evidence that the nursing process (NP) competency improves outcomes in critical illness,patient well-being,nursing care quality,and patient safety [7,8].By using the nursing process,nurses play a significant role in identifying the patient's health problems,providing interventions,and evaluating the outcomes of nursing care[9-11].
Despite the centrality of the nursing process,not all cultures have the necessary instruments to assess it.The nursing process has gained acceptance globally,and while registered nurses (RNs)agree on its beneficial effects,it is not widely used in practice[12,13]due to a lack of competence among RNs[14].One reason the widespread use of the nursing process has not emerged is that nurses lack competence and,consequently,lack confidence in their ability to use it[15,16].Applying the nursing process is connected to critical thinking and goal-oriented tasks.The Kingdom of Cambodia is making a concerted effort to further modernize and enhance professionalism in nursing.The standards of nursing care developed in Cambodia were approved in 2015 [17],and it explains the application of the steps of the nursing process within the nursing practice [18].However,over a few decades in Cambodia,the RNs use of the nursing process has not progressed as hoped due to a high nurse-patient ratio,24-h working shifts,lack of knowledge of the nursing process,and the pandemic [19].
A reliable and valid instrument designed specifically for Cambodian nursing is needed to improve competency in the nursing process at the Department of Hospital Services,Ministry of Health,Cambodia.In this study,competency of the nursing process refers to the extent to which the RN perceives their ability to practice the five steps of the nursing process to meet the patient’s needs by using critical thinking and specific skills.Based on the need for a competency assessment with respect to the nursing process,there were at least three reasons that a new instrument had to be developed despite that there were existing instruments:1) existing instruments did not focus on competency,2) available instruments were not based on the entire nursing process,and 3)the existing instruments lacked construct validity.
Cambodia’s healthcare system was classified from the community level to the national level.The lowest level is Complimentary Package Activity 1 (CPA1).This level provides health services such as minor surgery without anesthesia and maternity services.The CPA2 level provides medium surgery with anesthesia,emergency,maternity,and laboratory services.The CPA 3 level adds specialty surgery to the CPA2 level.Finally,the national hospitals have multiple specialists in surgery that a CPA3 cannot help.
Over the past three decades,a few studies in the west have focused on measuring nursing process.One such study developed an instrument to measure the attitudes of RNs,focusing on the nursing diagnosis step of the nursing process.The Positions on Nursing Diagnosis scale comprises 20 pairs of adjectives(e.g.,easy/difficult,important/unimportant),one of which reflects an attitude favoring the nursing diagnosis concept [18].A seven-point Likert scale was used to respond to the items,assigning a value of one to the most negative position on each pair and seven to the most positive.In 2018,a study measured the implementation of the nursing process using a five-point Likert scale (i.e.,never,sometimes,do not know,usually,and continuously).The degree of implementation of the five parts of the competency of nursing process (CNP) ranged from 36% to 57% [20].These two examples illustrate that the measures of CNP mainly reflected western cultures and did not focus on RNs’ perceptions of CNP.Given gaps in instruments available to assess the nursing process,we developed an instrument to measure the perceptions of registered nurses’competency in the clinical application of the nursing process in Cambodia.Our study aimed to develop the Competency of Nursing Process Questionnaire(CNPQ)and assess the reliability and validity of this new instrument.
2.Methods
2.1.Theoretical framework
This study guided by Nursing Process [21],which was the relationship between patient and nurse.This theory stressed that what the RNs did was find out about and meet the patient’s immediate need for help.With these,the RNs’ tasks are to know how to deal with those adverse effects so the patient can continue to get better well-being.The nursing process helps nurses develop a good plan for caring for a patient that can be easily changed if something goes wrong.Competency in the nursing process means that an RN has the confidence to use the knowledge,skills,attitude,and clinical judgment needed to do nursing tasks within the scope of their practice at an acceptable skill level.Based on this theory,this study made the competency items for each concept,such as assessment,diagnosis,planning,implementation,and evaluation.
2.2.Development of the first item pool
The item pool was created in the following ways.First,creating items for the scale,three focus group discussions(FGD)resulted in 44 items.In the first FGD,there were ten nurses with a associate degree in nursing: four men (40.0%),and six women (60.0%).The age range was 35-59 years;the average working experience was 27.5 years.In the second FGD,there were ten RNs with a bachelor’s degree: five men (50.0%) and five women (50.0%).The age range was 30-45 years,and the working experience was 21 years.Finally,in the last FGD,there were ten nurses with an master’s degree:six men and four women.The age ranged from 30 to 38 years,and the working experience was 12 years.The FGD was kept separate from the different levels of education of the participants because each group could freely talk about CNP.The average work experience of the RNs ranged from more to fewer years because the master’sprepared nurses were younger than those with Associate Degree and Bachelor’s Degree.
During the FGD,the authors ensured the trustworthiness by observing participants,taking notes of their opinions,and reviewing the verbatim compared with national and international findings to ensure transferability.In addition,the saturation method was followed for data collection and analysis.Last,the results were returned to participants’ feedback to ensure the validation of the findings.Second,the literature review produced 20 items from the relevant literature on competency of nursing process,competency of nursing diagnosis,attitude of implementation in nursing process,and Deliberative Nursing Process theory were initial generated;therefore,the total items were 64.
2.3.Primary questionnaire development
Considering the different participants’ contexts,the eight experts were invited to join the consultative workshop,including two nurse managers (one female and one male RNs),three nurse clinicians with a Bachelor of Nursing Science degree(two female and one male RNs),and three nurse educators with a Master of Nursing Science degree (two female and one male RNs).The age ranged from 30 to 55 years,and the average working experience was 25 years.At this stage,the eight experts were different from the FGD participants because of the input from many other points of view would benefit to obtain the experts’ content validity.
The consultative workshop and research team deleted similar 32 items,including American experts who had experience in developing the standard of nursing practice.However,the last phase,systematic assessment,was based on the interpretation and textual material according to the operational definition.It was found that eight items did not reflect the competency of the nursing process;thus,these eight items were deleted.Consequently,24 items composed the preliminary scale.
The Khmer version of the item pool was used by eight of the experts.The eight experts judged the items on a scale of 1=not relevant to 4=very relevant.Microsoft Excel was used to calculate the content validity index (CVI) at both the item and scale levels.The acceptable values are >0.79 and >0.80,respectively[22].
2.4.Formal investigation
2.4.1.Participants
Participants were recruited from five geographic(Phnom Penh-Kandal,Kampong Cham,Kampot,Battambang,and Stung Treng)areas in Cambodia who worked in Complimentary Package Activity(CPA)1,2,and 3 hospitals,national hospitals,and private hospitals.The sample size criterion was 10 participants per item for Exploratory Factor Analysis (EFA) [23].The initial CNPQ consisted of 24 items;therefore,the total estimated sample size was 264 participants (240 +10%).
2.4.2.Ethical considerations
The National Ethic Committee for Health Research approved this study(no.021-2022 NECHR).All participants signed consent forms before data collection.They were informed of their right to withdraw from the study at any time.
2.4.3.Instruments
2.4.3.1.General data questionnaire.The demographic data age,gender,working experience,educational levels,nurse leadership status,healthcare settings,were included.
2.4.3.2.Competency of nursing process questionnaire.The CNPQ is used to evaluate the level of competency of nursing process among RNs across 5 dimensions: assessment (4 items),nursing diagnosis(5 items),planning(5 items),intervention(7 items),and evaluation(3 items).In this step,the level of CNPQ was created based on the CNPQ total score;the higher the score,the higher the perceived competency of the nursing process.
The CNPQ was written in the form of a questionnaire.We used a five-point Likert scale response format for the items,where 1=feel not confident at all,2=feel not confident,3=feel that I need more practice,4=feel confident,and 5=feel proficient at that skill.
2.5.Data collection
The Google form was created for data collection between January and February 2022.The questionnaire was shared through the Khmer and English Google questionnaire platform,and researchers shared the online link with the nursing division at each hospital.The Google questionnaire included the no.021-2022 NECHR,the consent form,the participant information sheet,the contact details of the research members,and an anonymous platform.Each questionnaire took about 30 min for a nurse fulfill in.Only the research team could access and check at the end of the survey with confidentiality and anonymity for the participants.
2.6.Data analysis
The IBM SPSS version 26 (SPSS,IBM,2016,Armonk,New York,USA)was used for data processing and statistical analysis.The main key statistical analysis methods included descriptive statistics(frequency,mean,and standard deviation)and inferential statistics(factor analysis and Pearson correlation analysis).Statistical significance was set atP<0.05.
An exploratory factor analysis (EFA) principal component analysis was computed on the inter-correlations among CNPQ items.The reliability was evaluated using Cronbach’s α coefficient for the CNPQ and its dimension.The items scoring ≥0.3 were kept,and Cronbach’s α coefficient greater than 0.70 was accepted as internal consistency[24].The larger the correlation coefficient,the more the item represented the content of the evaluation tool.
Expert validity was used to reflect content validity,represented by the content validity index(CVI).A factor analysis was used to test the structural validity of the questionnaire.The content validity index was calculated using Microsoft Excel,including the content validity index,S-CVI/Ave >0.80,and I-CVIs >0.78 [25].The itemtotal correlations were suggested to be higher than 0.30 by previous authors [22].Pearson correlation coefficient between the two measurements was calculated to verify reliability of the questionnaire: two weeks later,the test-retest reliability was checked by asking fifty RNs who had already filled out the self-administered questionnaire to do it again to verify the repeatability of the CNPQ.
3.Results
3.1.Participant demographic characteristics
A high response rate of 98.0%was achieved as 260 out of the 264 questionnaires were returned.More than half of the participants were men(58.0%),and the average age was 28.83 years(SD=5.87).The years of work experience as an RN were ranked from 1 year to 30 years.Most participants had an associate degree in nursing(50.0%),46.0% had a bachelor’s degree,and 4.0% had a master’s degree.Most were RNs (91.0%),and team leaders and nurse managers accounted for 4.5% each.The participants were drawn from national hospitals,CPA 3,CPA 2,and CPA 1 hospitals,and private hospitals (21.2%,21.2%,20.0%,16.8%,and 20.8%,respectively).
3.2.Content validity and item analysis
The Khmer version of the item pool was used by eight of the experts.The 24-item of CVI value resulted that the scale-level CVI average was ranged 1.0,and the scale-level CVI universal average was ranged 1.0,and item-level of CVI was ranged 1.0.Therefore,the CNPQ demonstrated excellent content validity because an item CVI greater than 0.80 is considered excellent.
3.3.Construct validity
The Kaiser-Meyer-Olkin(KMO) test result was 0.926,which indicates that the sample size was adequate for EFA,and Bartlett’s test result was significant (χ2=4477.17,P<0.001),which demonstrated that all items were significantly correlated.The varimax rotation method’s principal component analysis (PCA)extraction was not used for EFA because there were five steps in the nursing process.The findings of EFA for five dimensions(24 items)included eigenvalues that ranged from 1.04 to 11.62,and the total variance explained was 70.08% (Tables 1 and 2).The item-total correlations for the 24 items ranged from 0.42 to 0.78.The correlation coefficients among the five dimensions ranged from 0.58 to 0.66 (P<0.05).
3.4.Reliability test
The Cronbach’s α coefficient of CNPQ for the total scale was 0.963,with dimensions values were 0.964,0.964,0.964,0.963,and 0.963 for assessment,diagnosis,planning,intervention,and evaluation,respectively (Table 1).Fifty participants were invited randomly to complete the CNPQ again two weeks after the first time.The intraclass correlation coefficient of the total questionnaire was 0.769,and the five dimensions ranged from 0.695 to 0.801 (P<0.01).

Table 1 The description 24-item of CNPQ after EFA (n=260).
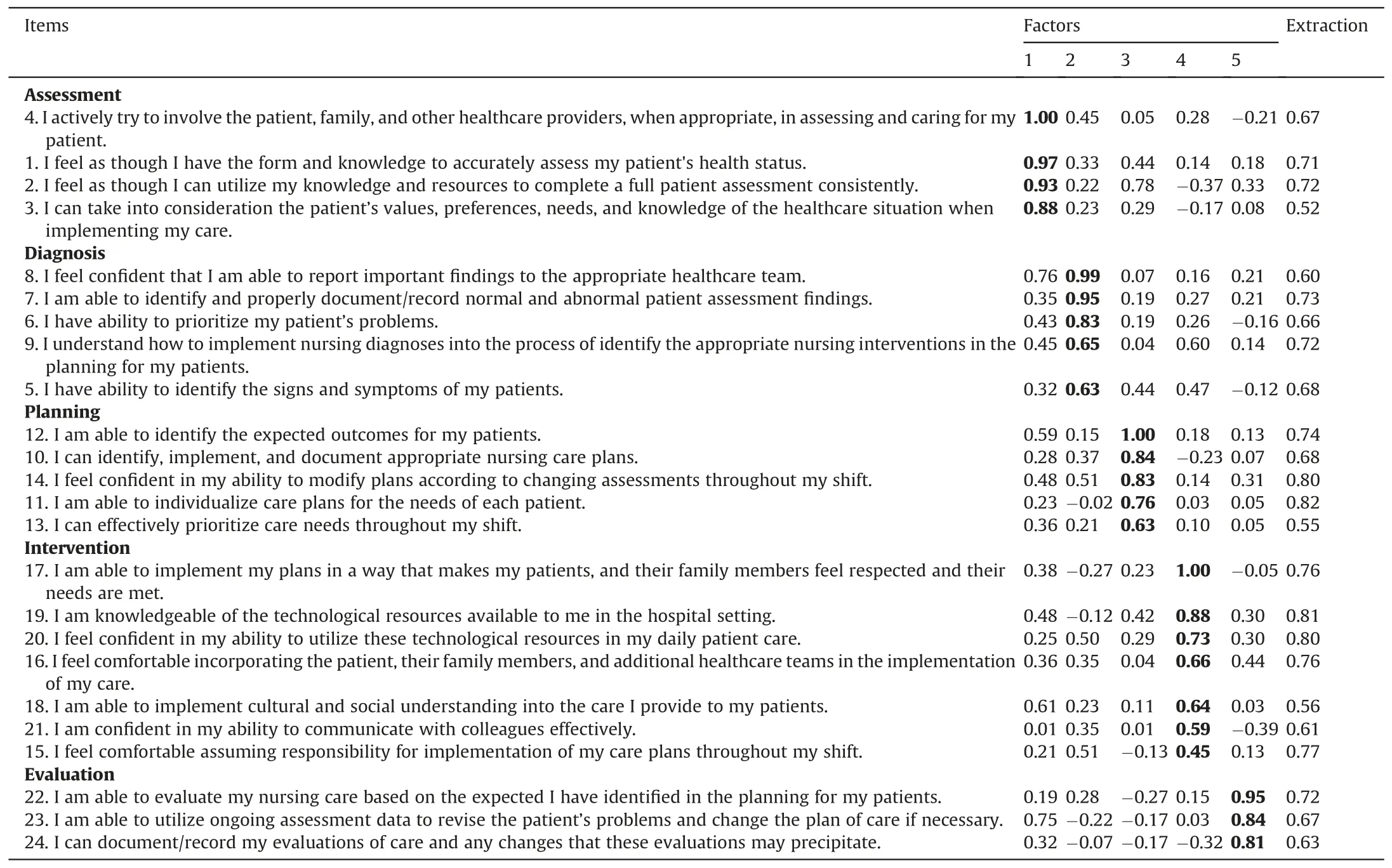
Table 2 Principal component analysis with varimax orthogonal rotation for CNPQ and 5-factor solution (n=260).
4.Discussion
4.1.The validity and reliability of the questionnaire
Content validity Index: the item CVI value was 1.0,the scalelevel CVI average was 1.0,and the scale-level CVI universal average was 1.0.Therefore,the CNPQ demonstrated excellent content validity because an item CVI greater than 0.80 is considered excellent[26].The reason was that the CNPQ was a good test of how nurses do their jobs in all settings,according to those who answered the questionnaire.
Internal consistency reliability was used to figure out how well all the questions on the CNPQ measure the same thing in the same way.Throughout the pilot study,the results were consistent(Cronbach’s α coefficient for the total scale and each subscale ranged from 0.93 to 0.94).A well-known and widely used tool needs a scale with Cronbach’s α coefficient of at least 0.80 [27].In addition,the correlations between items and totals ranged from 0.45 to 0.78.Because it is reliable,the CNPQ is a great way to measure CNP in all clinical nursing practices.
Our statistical analysis on construct validity,the CNPQ,indicated scientific validity.The EFA principal component analysis was used to investigate dimensionality.For good factor analysis,a KMO value greater than 0.600 is required [22].We adopted a maximum variance method and varimax with Kaiser normalization.EFA showed that KMO=0.926(>0.60),and the five factors explained more than 70% of the total variance of the CNPQ.It was required by previous scale development experts [21].
Pearson’s correlation coefficients were computed for the total scores.Correlations can be classified as very weak,weak,moderate,strong,and very strong associations (rrange: 0.000-0.190,0.200-0.390,0.400-0.590,0.600-0.790,and 0.800,respectively).The CNPQ receivedr=0.58-0.66,indicating moderate to strong correlation levels;as a result,the CNPQ is an excellent scientifically validated questionnaire for measuring the CNP in clinical settings[28].
Choosing the appropriate assessment questionnaire is critical for measuring CNP in various settings for RNs to maintain individual nurses’ competencies.In addition,this will also let the nursing staff figure out how well they understand the nursing process and where they need more education and training.
4.2.The practicality and scientificity of the questionnaire
In this study,we developed and evaluated the psychometric properties of an instrument to measure CNP,which has its roots in Cambodia’s culture and healthy environment.The development of the CNPQ has taken a different path than those taken by the several existing nursing process instruments in other countries.First,a literature review of current instruments was conducted,and the items related to the nursing process were pooled.Second,a review of the standards of nursing practice documentation was performed.Thus,the items included in this instrument were generated from the two sources.
It is also possible to relate this study to the nursing process approach because the items were relevant to each construct [13].The instrument was designed to measure perceived CNP and highlight the need for targeted competence improvement within Cambodian healthcare facilities.It is an essential first step in a developing country where advanced nursing techniques and nursing research are yet to make their mark[29].However,further psychometric testing of the CNPQ and possible refinement are needed.Instruments measuring CNP must be validated,reliable,and acceptable in the cultural context.
4.3.Limitation
The CNPQ was developed across practical nursing settings.Therefore,the scale items reflect the nature of the nursing process nurses implements.It is an excellent questionnaire to help with a precise understanding of the implementation of nursing processes in the clinical setting.
The first possible limitation with respect to generalizability was that 91%of the participants had an associate degree in nursing,and they may have different perceptions of the CNP compared with RNs with a bachelor’s or Master of Science in nursing degree.The second limitation is convenience sampling,which limits the findings from being generalized to the nursing population in Cambodia.The last,a lack of experts’ opinions on scale development may impact the appropriate number of clear and simple items.The CNPQ will need to be evaluated using a larger and more diverse sample of nurses to further support the measure’s validity and reliability.
5.Conclusion
The final version of the CNPQ comprises five dimensions.The internal consistency of the instrument was good.Satisfactory levels of construct validity imply that this scale can be used in clinical nursing practice to measure the nursing process.The next step is to use the instrument to compare the perceptions of RNs before and after the implementation of the nursing process in both public and private healthcare facilities in Cambodia.
The challenge for the health sector in any country,including Cambodia,is to ensure that nurses’ practice is of a high standard.Improving the standards of nursing practice requires reliable methods to assess baseline practice outcomes.The challenge continues for nurse administrators and RNs alike to demonstrate the effect of CNP on patient outcomes.
The results of this study provide nurse administrators and policymakers with empirical evidence of a measure that can be used to improve CNP in both public and private hospitals in Cambodia.When using instruments such as the CNPQ,nurse educators,mentors,and students can better understand nursing assessment,evaluation,and recording of relevant information related to the nursing process steps.This will increase novice nurses’ awareness of the nursing process in hospitals and help educators and mentors assess the competence of nursing students as well as their competence.Nursing institutions should consider reviewing or revising the curriculum to emphasize CNP,preparing the nursing process for new natural settings.
Funding
No external funding.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
CRediT authorship contribution statement
Virya Koy: Conceptualization,Methodology,Software.Andrew Rauth: Data curation,Writing-original draft.Manila Prak: Visualization,Investigation.Jintana Yunibhand:Supervision.Nicholas Bircher:Software,Validation.Richard Henker:Writing-reviewing and editing.
Declaration of competing interest
The authors have declared no conflict of interest.
Acknowledgments
The authors are grateful to Ministry of Health,the participants,research assistants,readers,translators involved the Cambodian National Ethics Committee for Health Research,and Internal Review Board of University of Pittsburgh.Appreciation is given to the Ratchadapisek Somphot Fund for a Postdoctoral Fellowship,Chulalongkorn University,Thailand.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2023.03.009.
杂志排行

International Journal of Nursing Sciences的其它文章
- A feasibility study on home-based kyphosis-specific exercises on reducing thoracic hyperkyphosis in older adults
- Development and validation of dynamic nomogram of frailty risk for older patients hospitalized with heart failure
- Validation of the Portuguese version of the social isolation scale with a sample of community-dwelling older adults
- Effects of pre-operative education tailored to information-seeking styles on pre-operative anxiety and depression among patients undergoing percutaneous coronary intervention: A randomized controlled trial
- Factors influencing the quality of sexual life in the older adults: A scoping review
- Comparison of the effects of three kinds of hand exercises on improving limb function in patients after transradial cardiac catheterization