Gastric intestinal metaplasia development in African American predominant United States population
2022-10-25AkramAhmadArielleLeeClaireCaplanColinWikholmIoannisPothoulakisZaynabAlmothaferNishthaRavalSamanthaMarshallAnkitMishraNicoleHodginsInGukKangRaymondChangZacharyDaileyArvinDaneshmandAnjaniKapadiaJaeHakOhBrittneyRodriguezAb
Akram I Ahmad,Arielle Lee,Claire Caplan,Colin Wikholm,Ioannis Pothoulakis,Zaynab Almothafer,Nishtha Raval,Samantha Marshall,Ankit Mishra,Nicole Hodgins,In Guk Kang,Raymond K Chang,Zachary Dailey,Arvin Daneshmand,Anjani Kapadia,Jae Hak Oh,Brittney Rodriguez,Abhinav Sehgal,Matthew Sweeney,Christopher B Swisher,Daniel F Childers,Corinne O'Connor,Lynette M Sequeira,Won Cho
Akram l Ahmad,loannis Pothoulakis,Department of Internal Medicine,MedStar Washington Hospital Center,Washington,DC 20010,United States
Arielle Lee,Claire Caplan,Colin Wikholm,Zaynab Almothafer,Nishtha Raval,Samantha Marshall,Ankit Mishra,Nicole Hodgins,ln Guk Kang,Raymond K Chang,Zachary Dailey,Arvin Daneshmand,Anjani Kapadia,Jae Hak Oh,Brittney Rodriguez,Abhinav Sehgal,Matthew Sweeney,Christopher B Swisher,Daniel F Childers,Corinne O'Connor,Lynette M Sequeira,Won Cho,Department of Internal Medicine,Georgetown University School of Medicine,Washington,DC 20007,United States
Won Cho,Department of Gastroenterology and Hepatology,INOVA Medical System,Leesburg,VA 20176,United States
Abstract BACKGROUND Gastric cancer significantly contributes to cancer mortality globally.Gastric intestinal metaplasia (GIM) is a stage in the Correa cascade and a premalignant lesion of gastric cancer.The natural history of GIM formation and progression over time is not fully understood.Currently,there are no clear guidelines on GIM surveillance or management in the United States.AIM To investigate factors associated with GIM development over time in African American-predominant study population.METHODS This is a retrospective longitudinal study in a single tertiary hospital in Washington DC.We retrieved upper esophagogastroduodenoscopies (EGDs) with gastric biopsies from the pathology department database from January 2015 to December 2020.Patients included in the study had undergone two or more EGDs with gastric biopsy.Patients with no GIM at baseline were followed up until they developed GIM or until the last available EGD.Exclusion criteria consisted of patients age < 18,pregnancy,previous diagnosis of gastric cancer,and missing data including pathology results or endoscopy reports.The study population was divided into two groups based on GIM status.Univariate and multivariate Cox regression was used to estimate the hazard induced by patient demographics,EGD findings,and Helicobacter pylori (H.pylori) status on the GIM status.RESULTS Of 2375 patients who had at least 1 EGD with gastric biopsy,579 patients were included in the study.138 patients developed GIM during the study follow-up period of 1087 d on average,compared to 857 d in patients without GIM (P=0.247).The average age of GIM group was 64 years compared to 56 years in the non-GIM group (P < 0.001).In the GIM group,adding one year to the age increases the risk for GIM formation by 4% (P < 0.001).Over time,African Americans,Hispanic,and other ethnicities/races had an increased risk of GIM compared to Caucasians with a hazard ratio (HR) of 2.12 (1.16,3.87),2.79 (1.09,7.13),and 3.19 (1.5,6.76) respectively.No gender difference was observed between the study populations.Gastritis was associated with an increased risk for GIM development with an HR of 1.62 (1.07,2.44).On the other hand,H.pylori infection did not increase the risk for GIM.CONCLUSION An increase in age and non-Caucasian race/ethnicity are associated with an increased risk of GIM formation.The effect of H.pylori on GIM is limited in low prevalence areas.
Key Words: Gastric intestinal metaplasia;Gastric cancer;Helicobacter pylori;Retrospective longitudinal study;Esophagogastroduodenoscopy;African American population
lNTRODUCTlON
Gastric cancer is the fifth most common cancer and the third leading cause of cancer mortality worldwide[1,2].Non-cardiac intestinal-type gastric adenocarcinoma represents the majority of cases in the United States[2].In 2018,over 26000 new cases of gastric cancer were reported with 10600 deaths in the United States[3];in 2020,more than 700000 deaths were reported globally[4].The high mortality rate of gastric cancer is mostly attributed to the late presentation of the disease.In areas with a high incidence of gastric cancer,the mortality-incidence ratio is decreased by screening programs[1],while in areas with low incidence,surveillance programs for gastric premalignant lesions in high-risk individuals are likely an optimal screening strategy based on risk stratification.
The Correa cascade proposed that intestinal-type gastric adenocarcinoma is formed from normal gastric mucosa that progresses through a series of transition stages: Chronic gastritis,atrophic gastritis,gastric intestinal metaplasia (GIM),and dysplasia,which can progress to gastric adenocarcinoma[5,6].The latter three histopathological findings are considered as gastric premalignant lesions.GIM is defined as the replacement of normal gastric epithelium with intestinal epithelium consisting of Paneth,goblet,and absorptive cells[7].The replacement happens under chronic stressors like inflammation.The prevalence of GIM in the general United States population is estimated to be 5%-8%[7] with an 0.13%-0.25%[6,7] estimated annual risk of progression into gastric cancer and a median time to progression of around 6 years[6].
Currently,GIM is more recognized as the best pre-malignant stage for surveillance because identifying and treating these lesions can potentially prevent further progression to gastric cancer[2,5].Multiple international guidelines recommend surveillance for gastric pre-malignant lesions including GIM[8,9];on the contrary,the American Gastroenterology Association (AGA) recommends against such screening guidelines for GIM with some exceptions[2].Multiple risk factors have been identified to help guide surveillance including smoking,alcohol use,ethnicity,family history of gastric cancer,and genetic factors[10].However,long-term effect of surveillance is not well understood in countries with a low incidence of gastric cancer due to the limitation of the available studies.Furthermore,the lack of clear guidelines for GIM medical management after diagnosis has added to the challenge[2].Thus,we designed this retrospective longitudinal study to investigate potential risk factors involved in GIM formation from normal mucosa in an African American predominant United States population.
MATERlALS AND METHODS
Study design
This is a retrospective longitudinal study conducted at Medstar Washington Hospital Center.The study was reviewed and approved by the Medstar Health Research Institute and Georgetown University Hospital Institutional Review Board.
Study population
Patients with GIM were identified from the Pathology Department’s database at Medstar Washington Hospital Center.Patients included in the study had undergone two or more esophagogastroduodenoscopies (EGDs) with gastric biopsy,with at least one EGD performed between January 2015 to December 2020.Exclusion criteria consisted of patients age < 18,pregnancy,previous diagnosis of gastric cancer,and missing data including pathology results or endoscopy reports.Patients with a baseline of no GIM were followed up longitudinally.The follow-up period ended at the event occurrence (GIM formation) or the last follow-up EGD.Based on the GIM status from the gastric biopsy at the end of the follow-up period,the study population was divided into two groups-GIM group and non-GIM group.Patients were excluded from the study if they were younger than 18 years old.
Data collection
Electronic medical records were reviewed to collect and analyze the following patient information: Demographics,medication use,EGDs findings,Helicobacter pylori(H.pylori) status,gastric biopsy reports,and laboratory findings.Patients’H.pyloristatuses were exclusively based on biopsy testing.
Data analysis
To present the data,we used frequency with percentage for categorical variables and median with first and third quartile (IQR) for non-normal continuous variables.The D'Agostino-Pearson test was used to test normality.Chi-square test with Yate’s correction or Kruskal-Wallis rank-sum test was performed to compare the difference between the groups.Kaplan-Meier estimators were calculated,and the curves were plotted to show the probability of GIM at a respective time interval after the baseline.To detect the differences in survival,we used Peto-Peto's weighted Log-rank test.Univariate and multivariate Cox proportional hazards regression model was performed to investigate how the predictors were associated with the risk of GIM over time.All unadjusted and adjusted hazard ratios with 95 percent confidence intervals were presented,along with the unadjustedPvalues.Statistical significance was set at aPvalue less than 0.05 and all statistical analyses were conducted with R software.The statistical methods of this study were reviewed by Jiling Chou from MedStar Health Research institute.
RESULTS
Overall data summary
Of 2375 patients who had at least 1 EGD with gastric biopsy during 2015 to 2020,579 patients met our inclusion criteria.A total of 138 (23.8%) patients developed GIM during the follow-up period of 1087 days on average,compared to 857 d in patients without GIM (P=0.247).The GIM group was older with an average age of 64 years compared to 56 years in the non-GIM group (P< 0.001).Female patients represented 60.7% (351 patients) of the total study population and there was not a significant difference between study groups (P=0.208).Ethnicity was significantly different between the study groups (P=0.032): African American,Caucasian,Hispanic and other ethnicities/races represented 72.9% (94 patients),9.3% (12 patients),5.4% (7 patients),and 12.4% (16 patients) of the GIM group respectively,compared to 71% (287 patients),18.1% (73 patients),2.7% (11 patients),and 8.2% (33 patients) in the non-GIM group respectively (Table 1).
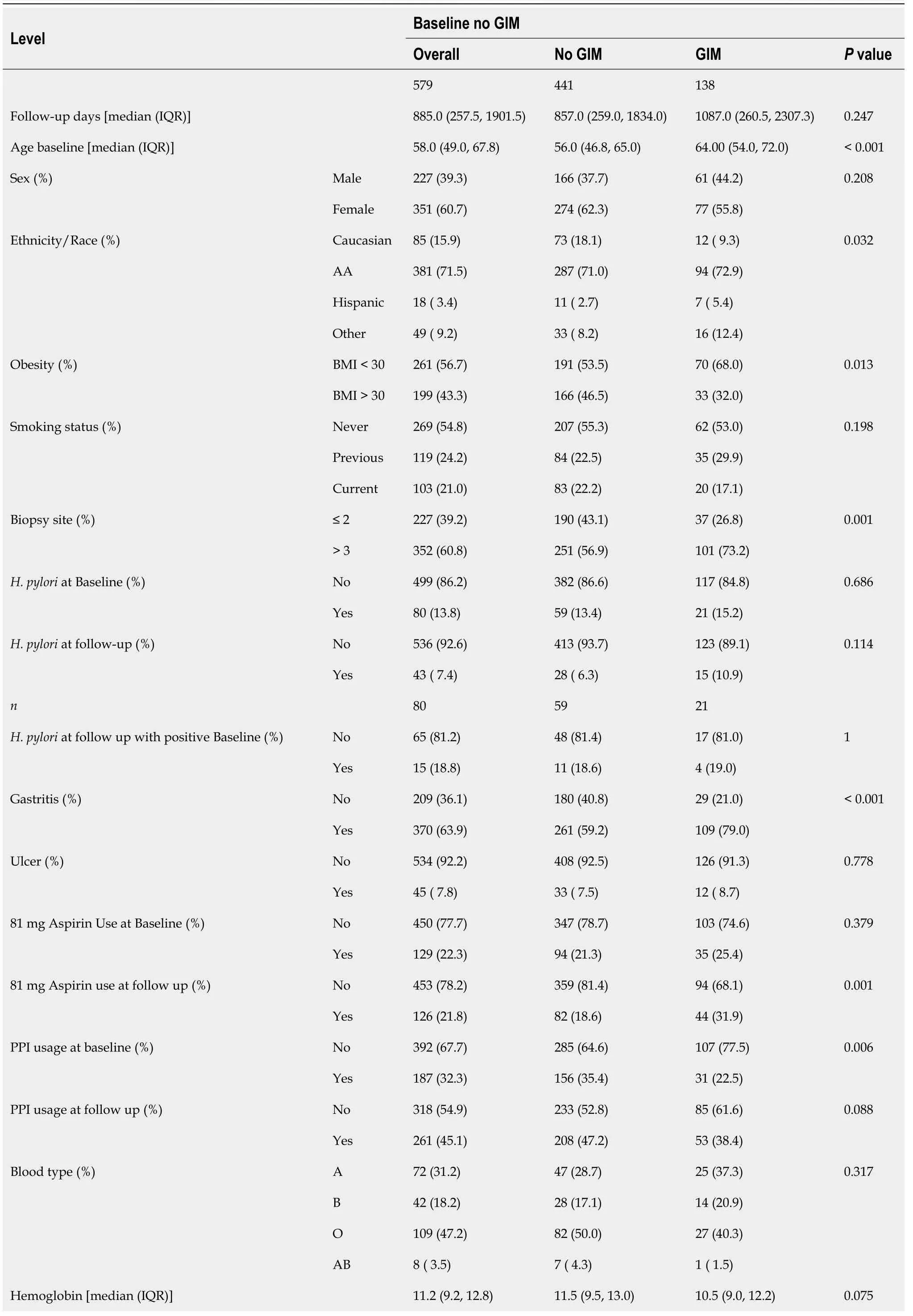
Table 1 Data summary and comparison between patients with and without gastric intestinal metaplasia

GIM: Gastric intestinal metaplasia;IQR: Interquartile range;AA: African Americans;BMI: Body mass index;PPI: Proton pump inhibitors.
Regarding medication use,a higher percentage of the GIM group [44 patients (31.9%)] was using 81 mg of aspirin on follow-up,compared to 82 patients (18.6%) in the non-GIM group (P=0.001).A lower percentage of the GIM group [31 patients (22.5 %)] was using proton pump inhibitors (PPI) at baseline compared to 156 patients (35.4%) in the non-GIM group (P=0.006).However,aspirin use at baseline and PPI use on follow up was not significantly different between study groups.
On follow-up EGDs,gastritis was observed more in the GIM group [109 patients (79.0 %)] compared to 261 patients (59.2%) with gastritis in the non-GIM group (P< 0.001) (Table 1).
H.pyloriwas positive in the baseline biopsies of 80 patients (13.2%),compared to those of 43 patients (7.4 %) on follow-up.Of thisH.pyloripositive group,15 patients had positiveH.pyloriat both the baseline and follow-up,but this persistentH.pyloriinfection was not different between the two study groups.A detailed summary of the data is presented in Table 1.
Risk of GIM over time
In a group of patients with no GIM at baseline,adding one year in age increases the risk of GIM by 4% over time with aPvalue < 0.001.In comparison to the age group of 45 years or younger,patients have a hazard ratio (HR) of 2.13 (P=0.028),2.09 (P=0.029),and 4.03 (P< 0.001) for age groups 46-55,56-64,and ≥ 65 years respectively.Over time,African Americans,Hispanics,and other ethnicities/races had an increased risk of GIM compared to Caucasians with an HR of 2.12 (1.16,3.87),2.79 (1.09,7.13),and 3.19 (1.5,6.76) respectively.Gastritis on follow-up biopsy was associated with a higher risk of GIM with an HR of 1.62 (1.07,2.44) (P=0.022),while 81 mg aspirin use increased the risk of GIM by 49% (P=0.031).Obesity at baseline had a 42% less risk of GIM (P=0.010).Using theH.pylori-negative group at baseline and follow-up as a reference group,H.pyloriinfection at baseline or follow-up,as well as the persistence ofH.pyloriinfection did not have significant effects on GIM risk over time.Subgroup analysis of patients withH.pyloripresent at baseline shows no major difference from the main study analysis (Table 2).
On multivariate Cox regression analysis,the age ≥ 65 group was continuously associated with a higher risk of GIM with an HR of 3.01 (P=0.014).African Americans and other ethnicities have a higher risk of GIM with an HR of 3.4 (P=0.026) and 7.46 (P=0.001) when compared to Caucasians respectively.Hispanic,other age groups,gastritis,H.pyloristatus,and smoking status did not reach the level of statistical significance on multivariate analysis (Table 3).
We calculated the Kaplan-Meier survival estimate for GIM development over 12 years.The population at risk is limited by the available follow-up EGD and censored observations.At the 12 years follow-up,26 patients were at GIM risk (Figure 1A).Close to 50% of the population at risk developed GIM during 12 years of follow-up.A 12 years survival Curve was done to present the survival probability of developing GIM based on ethnicity,age group,and gastritis status (Figure 1B-D).We observed a significant difference in the GIM development over 12 years based on gastritis status (P=0.023),age group (P< 0.0001),and ethnicity (P=0.023).
DlSCUSSlON
GIM is a recognized gastric pre-malignant lesion with an increased risk for developing gastric cancer.The risk factors for GIM formation and evolution are significant clinical interest and thus currently under active investigation since these factors will likely help design optimal surveillance programs and management of GIM after diagnosis.Our study showed that the GIM group was older compared to the non-GIM group (Table 1).In multiple studies including ours,more advanced age was associated with an increased risk of GIM formation,progression,and gastric cancer development,which could be attributable to prolonged exposure of gastric mucosa to mutagenic factors and inflammation[1,4,11].The average age at GIM diagnosis in low gastric cancer incident countries was 60 to 67 years,comparable to the average age of 64 in our GIM group (Table 1)[1,11,12].A one-year increase in age was associated with a 4% increase in GIM risk in our population.Age groups of 45-54,55-64,and > 65 were associated with an increased risk for GIM development compared to the < 45 age group (Table 2).The age group > 65 had the highest HR,and it was the only age group associated with an increased risk of GIM formation on multivariate analysis (Table 3).However,a study in China found that age > 45 is associated with GIM progression[13].After five years of follow-up,around 50% of patients in group > 65 develop GIM,compared to 10% in < 45 age group (Figure 1C).These results suggest that an age close to 65 may be a good threshold for screening for GIM.
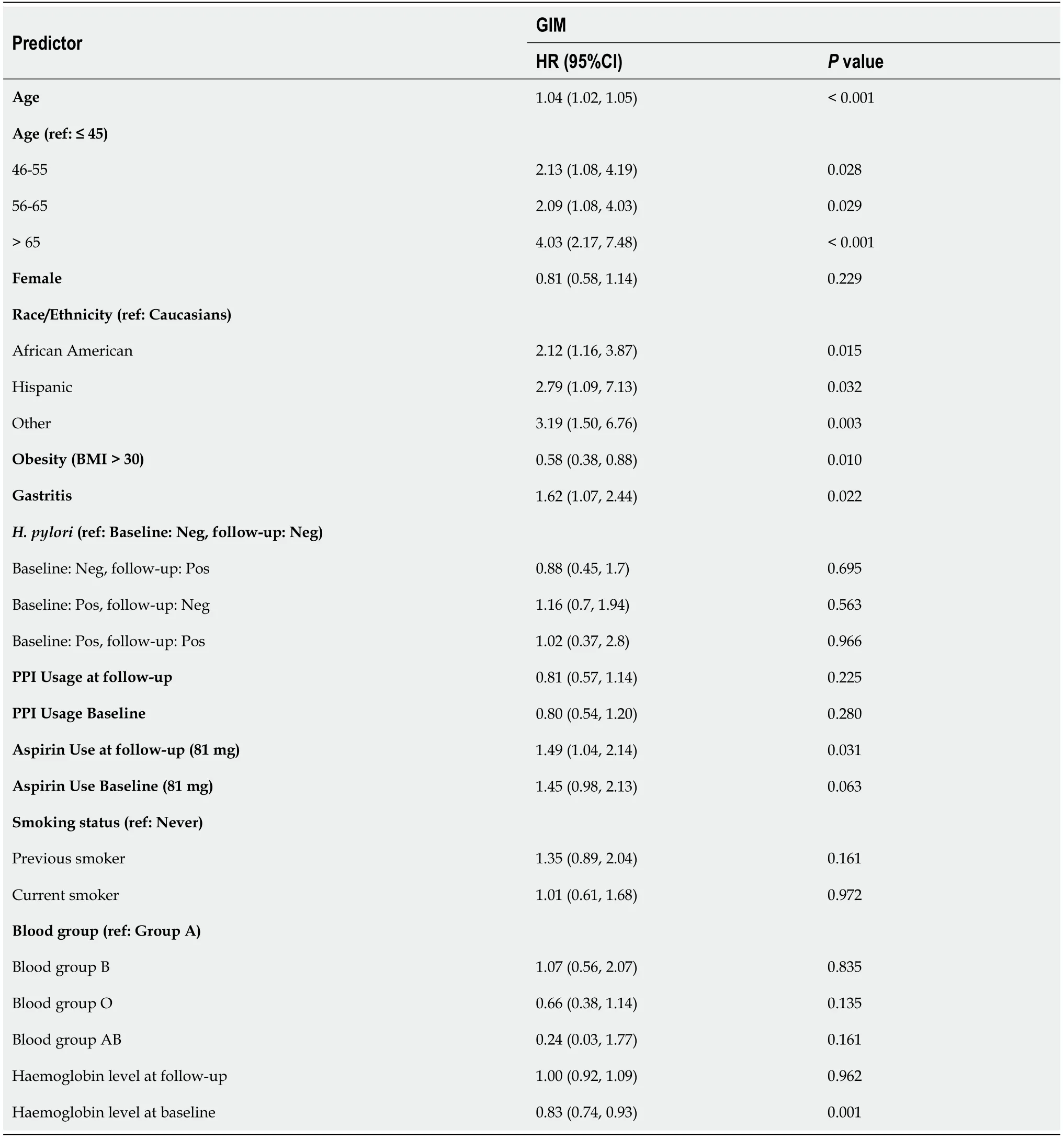
Table 2 Univariate Cox proportional hazards regression model results for gastric intestinal metaplasia formation over time
Although gastric cancer is known to be more common in males[14],GIM has equally affected both genders in our study and others[1,4].In contrast,a cohort study in Puerto Rico showed a greater percentage of females affected by GIM compared to males[12],and in a Thai population,the male sex was a risk factor for GIM development[11].The influence of gender on GIM development might be significant,but our study might have failed to detect it due to the small sample size.Alternatively,gender might have an isolated effect on GIM progression to gastric cancer rather than GIM development.
Non-cardia gastric cancer has a higher incidence rate in certain United States race/ethnicity minorities including,African Americans,Hispanics,and Asians[15].Previous studies on the United States population have shown that ethnicity is a risk factor for GIM formation,independent of age orH.pyloristatus[16-18].Non-Hispanic whites have the lowest risk of GIM in comparison to other races/ ethnicities.Hispanics,followed by African Americans,carry the highest risk for GIM compared to non-Hispanic whites,which is consistent with other studies[16-18].Our study also showed African Americans,Hispanics,and other ethnicities/races had an increased risk of GIM compared to Caucasians (Table 2).However,the Hispanic population did not reach the statistical significance level on multivariant analysis,likely due to the small size of Hispanic population in our study (Table 3).The Asian population is also thought to have a higher risk of GIM,but this population is generally less investigated in United States literature due to the small number of Asians in the United States.Asian and different groups of ethnic and racial minorities were combined as the other ethnic/racial group in our study,this group carried the highest HR when compared to Caucasians.After 5 years of follow-up,close to 25% and 50% of Caucasians and other ethnic/racial groups developed GIM (Figure 1B).Our study is notable that African Americans represent the majority of our study population and carry a higher risk for GIM.
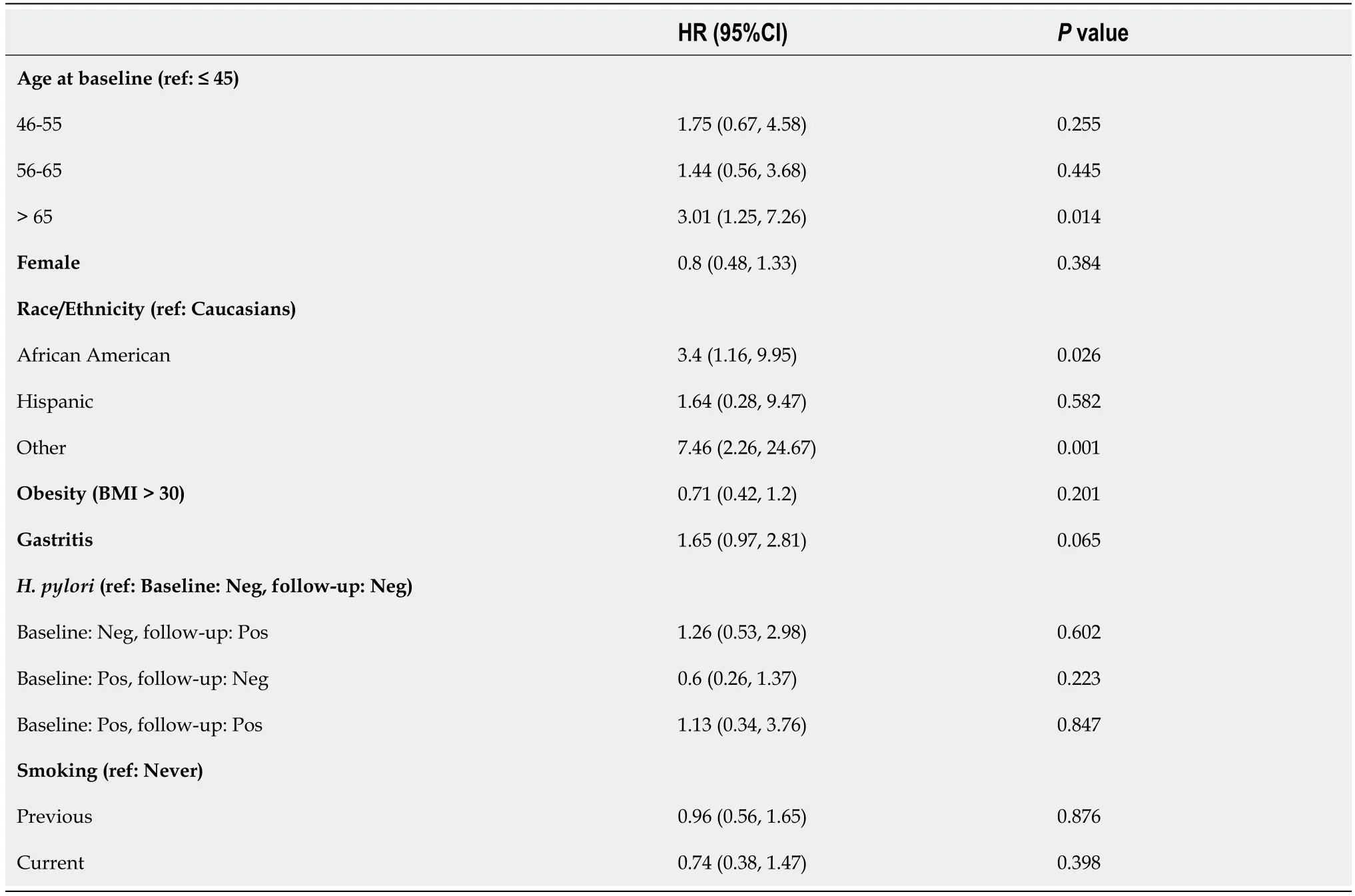
Table 3 Multivariate Cox proportional hazards regression model results for gastric intestinal metaplasia formation over time
Currently,the AGA recommends surveillance for ethnic/racial minorities only on a conditional basis[2].Place of birth,rather than ethnicity,was shown to be a risk factor for GIM in one study,where only Hispanics born outside the United States carry a higher risk for GIM compared to Hispanics born in the United States regardless ofH.pyloristatus[19].The effect of place of birth and race on GIM needs further investigation,as it might be a potential factor that affects surveillance.
The impact ofH.pyloriinfection on GIM formation and progression was extensively investigated,but the results in the literature were often conflicting thus suggesting the complex role ofH.pyloriin GIM and gastric cancer.H.pyloriinfection is thought to affect the development and progression of GIM[20],but few studies have shown either formation or progression but not both[17].Ethnicity,genetic makeup,andH.pylorivirulence factors are additional factors that can further influence the effect ofH.pylorion GIM[10,18,21].However,in the present study,no clear effect ofH.pylorion GIM development was found as shown in other studies[4,19,22].In our study population,only 13.8% of patients hadH.pyloriinfection,which is lower than the reported averageH.pyloriinfection in the United States and patients with positiveH.pyloriinfection at baseline biopsy,follow-up biopsy,or both seem to have the same risk of developing GIM,not different from those who tested negative forH.pylori.However,given the known strong association betweenH.pyloriand gastric cancer,we agree with the AGA recommendation for testing and treatingH.pyloriand confirming its eradication,especially if positive in GIM,even though our results did not show a direct effect ofH.pylorion GIM formation.
Chronic gastritis is part of the Correa cascade,and it precedes GIM development.The long-term effect ofH.pylori-negative chronic gastritis and its role in the development of GIM have been poorly studied.A prospective study in Thailand investigated 400 patients with chronic gastritis and showed that chronic gastritis is associated with an increased risk for progression regardless ofH.pyloristatus[4].Our study showed that gastritis is associated with GIM formation over time.The gastric inflammation,rather than the H.pylori infection itself,might be driving GIM formation.On the 12 years survival curve,a significant difference in GIM formation is shown between the group with and without gastritis,noticeable as early as 1 year (Figure 1D).Thus,early recognition and treatment of gastritis can impact GIM formation and possibly prevent GIM thus reducing gastric cancer risk.
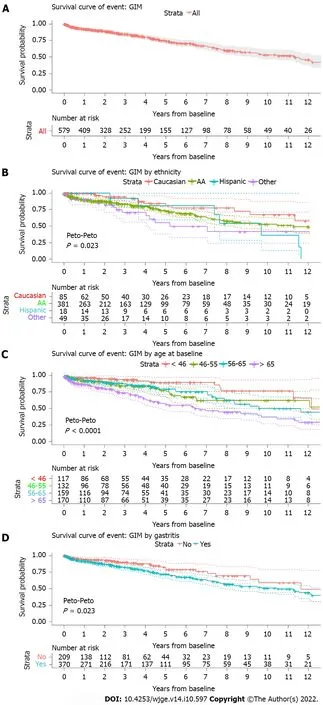
Figure 1 Survival estimate curve along with population at risk table.
The study is limited by its retrospective nature.All the patients in the study are from a single tertiary center in Washington,DC.The standard evaluation of GIM in our pathology lab does not involve further grading or classification,which added to the study's limitation.In spite of the retrospective nature of the study,the strength of our study is its unique study design and distinct study population to assess the longitudinal data over time between upper endoscopies in a single academic center with a predominantly African American population,which has not been adequately investigated in other studies.It is also notable that this study population has a low prevalence ofH.pylori,thus allowing us to examine other risk factors involved in the development of GIM aside fromH.pyloriinfection.Our limitations also include the low number of Asians in our study population who were included as the other ethnic/racial category in our study,thus limiting comparisons with other published studies from Asia.
CONCLUSlON
In conclusion,our study demonstrates that race is an important risk factor for GIM and ethnic/racial minorities in the United States carry a higher risk of GIM compared to Caucasians.Older age,especially age group > 65,was associated with higher GIM risk.Gastritis rather thanH.pyloriinfection is also associated with GIM formation in our lowH.pyloriprevalent patient population.These risk factors identified in our study will serve as important components in developing risk stratification models for optimal surveillance programs for GIM and gastric cancer.
ARTlCLE HlGHLlGHTS
Research background
Gastric intestinal metaplasia (GIM) is a form of gastric pre-malignant lesions.It falls on the spectrum of the Correa cascade.The cascade includes chronic gastritis,atrophic gastritis,GIM,and dysplasia.
Research motivation
We designed this study to investigate factors leading to GIM formation.There is a lack of literature about this topic in the United States,especially among ethnic minorities,which are considered high-risk populations.
Research objectives
We aimed to identify factors that increase GIM formation in high-risk populations.These factors would help guide the future surveillance of selected patients and possibly suggest treatment modalities.
Research methods
This is a retrospective longitudinal study in a tertiary hospital in Washington,DC.The study includes patients with at least two upper endoscopies with gastric biopsies to assess the evolution of GIM over time.A Cox regression model was built to investigate the significant factors over the study time.
Research results
Our study confirms that Ethnicity-Race minorities have a higher rate of GIM formation.We found that gastritis increases GIM formation over time.Helicobacter pylori in low-prevalence areas might not be a strong risk factor.Our results emphasize on future surveillance of minorities and management of gastritis as a way to reduce the burden of gastric cancer.
Research conclusions
In conclusion,our study suggests that older age,having gastritis,or being from ethnic-race minorities is associated with an increased risk of GIM.
Research perspectives
Further studies are needed to clarify factors associated with GIM progression and regression.This would help form a complete picture of the development and progression of gastric pre-malignant lesions.
FOOTNOTES
Author contributions:Ahmad AI and Cho W contributed to the study designing and wrote the manuscript;Ahmad AI,Cho W,Lee A and Pothoulakis I contributed to the manuscript edit;Lee A,Caplan C,Wikholm C performed the project coordinator;Lee A,Caplan C,Almothafer Z,Raval N,Marshall S,Hodgins N,Kang IG,Chang RK,Dailey Z,Daneshmand A,Kapadia A,Oh JH,Rodriguez B,Sehgal A,Sweeney M,Swisher CB,Childers DF,Mishra A,O'Connor C and Sequeira LM contributed to the data collection.
lnstitutional review board statement:The study was reviewed and approved by the Medstar Health Research Institute and Georgetown University Hospital Institutional Review Board.
lnformed consent statement:The study was exempt from informed consent based on the MedStar Health Research Institute IRB committee.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:Technical appendix,statistical code,and dataset available from the corresponding author at Akram.i.ahmad@medstar.net.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:United States
ORClD number:Akram I Ahmad 0000-0001-5168-8050;Arielle Lee 0000-0003-3421-953X;Claire Caplan 0000-0002-5259-4117;Ioannis Pothoulakis 0000-0002-3084-8577;Zaynab Almothafer 0000-0002-8286-7921;Nishtha Raval 0000-0002-8613-4872;Samantha Marshall 0000-0002-1663-6949;Ankit Mishra 0000-0002-7277-4027;Nicole Hodgins 0000-0002-4606-7724;Raymond K Chang 0000-0002-1250-6725;Zachary Dailey 0000-0001-8243-1848;Arvin Daneshmand 0000-0003-3926-7311;Anjani Kapadia 0000-0003-4072-2019;Jae Hak Oh 0000-0003-3401-6345;Brittney Rodriguez 0000-0002-3512-4973;Abhinav Sehgal 0000-0001-7410-8768;Christopher B Swisher 0000-0002-6570-0564;Daniel F Childers 0000-0003-3878-0965;Corinne O'Connor 0000-0001-7496-6340;Lynette M Sequeira 0000-0002-5246-2317.
S-Editor:Fan JR
L-Editor:A
P-Editor:Fan JR
杂志排行

World Journal of Gastrointestinal Endoscopy的其它文章
- Endoscopic palliation of malignant biliary obstruction
- Water-jet vs traditional triangular tip knife in peroral endoscopic myotomy for esophageal dysmotility:A systemic review and metaanalysis
- Laparoscopic Janeway gastrostomy as preferred enteral access in specific patient populations:A systematic review and case series
- Tracheoesophageal fistulas in coronavirus disease 2019 pandemic:A case report
- Hemostasis of massive bleeding from esophageal tumor:A case report
- Cronkhite-Canada syndrome:First case report from Egypt and North Africa