Therapeutic potential of dental pulp stem cells and their derivatives:lnsights from basic research toward clinical applications
2022-08-01ShengMengYuanXueTingYangSiYuanZhangWeiDongTianBoYang
Sheng-Meng Yuan, Xue-Ting Yang, Si-Yuan Zhang, Wei-Dong Tian, Bo Yang
Sheng-Meng Yuan, Xue-Ting Yang, Si-Yuan Zhang, Wei-Dong Tian, Βo Yang, State Key Laboratory of Oral Diseases, National Clinical Research Center for Oral Diseases, Engineering Research Center of Oral Translational Medicine, National Engineering Laboratory for Oral Regenerative Medicine, West China Hospital of Stomatology, Sichuan University, Chengdu 610041, Sichuan Province, China
Sheng-Meng Yuan, Xue-Ting Yang, Wei-Dong Tian, Βo Yang, Department of Oral and Maxillofacial Surgery, West China Hospital of Stomatology, Sichuan University, Chengdu 610041, Sichuan Province, China
Abstract For more than 20 years, researchers have isolated and identified postnatal dental pulp stem cells (DPSCs) from different teeth, including natal teeth, exfoliated deciduous teeth, healthy teeth, and diseased teeth. Their mesenchymal stem cell(MSC)-like immunophenotypic characteristics, high proliferation rate, potential for multidirectional differentiation and biological features were demonstrated to be superior to those of bone marrow MSCs. In addition, several main application forms of DPSCs and their derivatives have been investigated, including stem cell injections, modified stem cells, stem cell sheets and stem cell spheroids. In vitro and in vivo administration of DPSCs and their derivatives exhibited beneficial effects in various disease models of different tissues and organs. Therefore, DPSCs and their derivatives are regarded as excellent candidates for stem cell-based tissue regeneration. In this review, we aim to provide an overview of the potential application of DPSCs and their derivatives in the field of regenerative medicine.We describe the similarities and differences of DPSCs isolated from donors of different ages and health conditions. The methodologies for therapeutic administration of DPSCs and their derivatives are introduced, including single injections and the transplantation of the cells with a support, as cell sheets, or as cell spheroids. We also summarize the underlying mechanisms of the regenerative potential of DPSCs.
Key Words: Dental pulp stem cells; Cell injections; Modified cells; Cell sheets; Cell spheroids; Regeneration
lNTRODUCTlON
Dental pulp stem cells (DPSCs) have received major attention since they were first isolated in 2000 due to their easily accessible properties, lack of ethical problems, high proliferation ability and multidirectional differentiation potential[1-3]. Since then, numerous studies have emerged on the extraction and identification of DPSCs. Scholars have obtained DPSCs from a variety of dental sources and confirmed that they are superior to bone marrow mesenchymal stem cells (MSCs) in various characteristics, such as easier access, higher proliferation, and better neural differentiation[4-8].
In view of their excellent stem cell characteristics, DPSCs, as an important source of postnatal MSCs,have been widely studied in the field of regenerative medicine in the past two decades, including but not limited to cerebral ischemia[9], bone and dental loss defects[10,11], the nervous system[12], the digestive system[13] and the endocrine system[14], and many studies have achieved meaningful therapeutic effects. Meanwhile, in the application of regenerative medicine, with the continuous progress of cell culture and modification technologies, the application forms of MSCs continue to expand, such as the transformation from primitive cells to modified cells and the leap from single-cell preparations to multicell units[15-17]. These enhanced stem cell applications play an important role in improving the therapeutic effect of stem cells, which promotes the development of tissue engineering and regenerative medicine.
However, the mechanism by which DPSCs promote regeneration has not been fully revealed. At present, two main aspects of MSCs, immunomodulatory and paracrine effects, have been widely discussed[18-20]. MSCs have been suggested to possibly be involved in the process of immune regulation in the host by regulating the physiological functions of immune cells such as T cells, B cells,dendritic cells (DCs), and natural killer (NK) cells[21] or transmitting intercellular signals through paracrine pathways such as secretomes, exosomes and extracellular vesicles (EVs)[22-24], thereby inhibiting inflammation and promoting disease improvement. In addition, transplanted stem cells may directly promote the repair or regeneration of tissue injury by residing at the transplant site and differentiating into corresponding cells[25-29]. As a promising member of the MSC family, DPSCs may also play a role through the above mechanism in the process of promoting injury repair and reconstruction or disease improvement[18,30,31].
In this review, we introduce DPSCs from different sources and their characteristics and discuss several main applications of DPSCs in regenerative medicine in recent years, including cell injections(cell suspensions), modified cells, cell sheets and cell spheroids. We introduce the background,biological characteristics, representative examples and preliminary therapeutic effects of these various derivatives in regenerative medicine and briefly summarize the possible mechanisms of DPSCs in promoting regeneration.
SOURCES OF DPSCS
Since their discovery, DPSCs have garnered extensive attention due to their easily accessible features and lack of ethical issues. In 2000, Gronthoset al[1] isolated clonogenic and highly proliferative cells from enzymatically disaggregated dental pulp tissue of normal human impacted third molars for the first time. The isolated cells were termed DPSCs[1]. Since then, many researchers have focused on DPSCs and successfully isolated these cells from dental pulp tissue of different ages and different states,as well as using cell sorting technologies to isolate subsets of cells with special phenotypes. These DPSCs have both the same characteristics and obvious differences.
DPSCs from teeth of different ages
To date, researchers have extracted DPSCs from teeth of different age groups, including children(deciduous teeth), adolescents, adults, aged (permanent teeth) and even infant donors (natal teeth)[1,32-34]. The most common are DPSCs from adult permanent teeth (generally less than 30 years old) and exfoliated deciduous teeth.
Adults (generally less than 30 years old):Adult human health dental pulp tissue derived dental pulp cells, as subsequently demonstrated by Gronthoset al[1], contained clonogenic cell populations within them that have the ability to form clones. Although colonies of dental pulp cells occurred at a similar frequency in comparison to bone marrow mesenchymal stem cells (BMSCs) from bone marrow aspirates flushed free of hematopoietic cells, DPSCs exhibited a higher proliferation rate than BMSCsin vitro, and they maintained their high rate of proliferation even after extensive subculturing[1]. In view of this phenomenon, the authors believe that DPSCs satisfy two of the criteria of a postnatal somatic stem cell:ex vivoexpansion and clonogenicity[35]. Also, transplanted DPSCs can generate a dentin-pulp-like complex representative of the microenvironments from which they were derivedin vivo, which underscores one of their stem cell natures again: Tissue reconstitution[1,35]. Later studies improved the immunophenotypic identification of DPSCs from adult healthy teeth and repeatedly confirmed their multidirectional differentiation ability, finding that DPSCs are positive for mesenchymal lineage markers (CD13, CD29, CD44, CD73, CD90 and CD105) and negative for monocytic (CD14) and hematopoietic lineage markers (CD34, and CD45). At the same time, DPSCs have the potential to differentiate into typical mesodermal cell lineages, such as osteogenic, chondrogenic, and adipogenic lineages[4-7]. In conclusion, DPSCs derived from adult healthy dental pulp have the phenotypic characteristics and multidirectional differentiation ability of MSCs and meet the criteria for postnatal somatic stem cells.
Children (deciduous teeth):In 2003, Miuraet al[32], for the first time, isolated stem cells from exfoliated human deciduous teeth, named stem cells from human exfoliated deciduous teeth (SHED), which were also identified as a population of highly proliferative, clonogenic cells capable of differentiating into a variety of cell types, including odontoblasts, endothelia, neural cells and adipocytes[32,36,37]. They could also express MSC markers such as CD29, CD73, CD90, CD105, CD146, and STRO-1[32,38,39].However, SHED showed higher expression of CD105 and CD146 than DPSCs, suggesting that SHED is a unique undifferentiated stem cell lineage and may have a higher capacity for differentiation[38].Subsequent studies confirmed the differences between SHED and adult DPSCs, including that the SHED exhibited more colony forming units, shorter doubling time, higher proliferation rate, higher endothelial differentiation potential, stronger osteogenic and adipogenic differentiation abilityin vitroand osteoinductive capacityin vivo[32,38,40,41]etc. Even under the adverse culture conditions of hypoxia, high glucose and low serum, the above characteristics of SHED were still better than the characteristics of DPSCs[42]. However, the neurogenic ability of SHED is lower than the neurogenic ability of DPSCs[43,44]. In short, from the current findings, SHED may be a better seed cell player than DPSCs in addition to neurogenic ability, which may be attributed to its younger physiological age.
Other ages:In addition to the above two common sources of DPSCs, another study reported that DPSCs obtained from natal teeth also have the immunophenotypic characteristics (expressed CD13, CD44,CD73, CD90, CD146, and CD166, but not CD3, CD8, CD10, CD11b, CD14, CD15, CD19, CD33, CD34,CD45, CD71, CD117, and HLA-DR) and multidirectional differentiation (adipogenic, osteogenic,chondrogenic, myogenic and neurogenic) potential of MSCs[45]. In addition, compared with the deciduous pulp, the expression of nestin and CD44 was stronger in the dental pulp of natal teeth.Positive immune expression of SOX2 (embryonic stem cell marker) was observed only in the dental pulp of natal teeth, which confirms the presence of a higher percentage of stem/progenitor cell population compared with the deciduous pulp[34]. In addition, Wuet al[33] specifically compared the growth and differentiation characteristics of DPSCs from patients of different ages, including children,adolescents, adults and aged donors. The results showed that although a large portion of cell surface markers was expressed in all DPSC lines, the expression of CD29 was downregulated in the DPSCs from aged teeth. At the same time, the doubling time of DPSCs from aged teeth was prolonged, and the number of apoptotic cells increased with propagation. Moreover, these DPSCs from aged teeth were completely or partially deprived of lineage differentiation capacity[33]. These results suggest that DPSCs from younger ages are more suitable as excellent candidates for regenerative medicine stem cell resource banks.
DPSCs from different pulp health statuses
Although the sources of healthy dental pulp are very extensive, the sources of unhealthy dental pulp are more abundant with the trend of frequent occurrence of caries, dental pulp diseases and periodontitis.Therefore, some researchers have turned their attention to the field of dental pulp in different healthy states to expand the potential source range of DPSCs.
Yuet al[46] reported that stem cells from inflamed pulp of deciduous teeth (SCIDs) were positive for cell surface markers, including CD105, CD90, and CD146, and had high proliferation ability and osteogenic, adipogenic, and chondrogenic differentiation potentials. Except for SCIDs that secreted more tumor necrosis factor-α (TNF-α) protein, there was no significant difference in proliferation and differentiation potentials between SCIDs and SHED[46]. Pereiraet al[47] also supported that the morphology, proliferation rate and differentiation potential of inflamed and normal DPSCs are similar[47].
However, Kimet al[48] and Alongiet al[49] reported different results: The abilities of colony forming and osteogenic differentiationin vitroandin vivoof stem cells from inflamed pulp tissue were decreased compared with normal DPSCs[48,49]. Another study also confirmed that DPSCs from carious teeth(DPSCs-CT) are not as efficient as normal DPSCs in differentiating into dopaminergic-like cells[50]. The colony forming capacity of stem cells isolated from pulp polyps (chronic hyperplastic pulpitis) and dental pulp with irreversible pulpitis was also lower than the colony forming capacity of healthy DPSCs, but both cell types (normal and pulpitis) have demonstrated the ability to form pulp/dentin complexes when transplanted into immunocompromised mice[51,52].
Interestingly, strong staining for CD146 was observed in inflamed pulps during the initial inflammatory response, and short-term TNF-α treatment has also been confirmed to enhance dental pulp cell function, including the ability to form cell colonies, migrate, and differentiate into odontogenic and adipogenic lineages[53]. Moreover, researchers have also identified and studied DPSCs isolated from teeth with different stages of aggressive periodontitis (representing different degrees of dental pulp inflammation) to explore the impact of periodontal infection during the progression of periodontitis on the pluripotency and regenerative potential of DPSCs within periodontally compromised dental pulp.The results showed that periodontal inflammation had a negative impact on the colony forming ability and proliferation of DPSCs, but the relationship between the effect on their pluripotency and the severity of the disease was uncertain. Although DPSCs from the inflamed dental pulp of teeth extracted due to aggressive periodontitis appear to have undergone some changes in terms of their stem cell properties, they still possess the capacity to differentiate into odontoblastic and osteoblastic phenotypesin vitroand form pulp- and dentin-like tissuesin vivo[54]. These data indicate that the stem cell characteristics of unhealthy dental pulp-derived stem cells are unstable, which may be related to the degree of inflammation in the diseased dental pulp. Further characterization is needed to determine whether they can serve as a source of therapeutic cells for future regenerative therapies.
Subpopulations of DPSCs
DPSCs showed heterogeneity in the earliest isolation and identification studies: In primary cultured DPSCs, many of the phenotypic markers were not uniformly expressed but were found in subsets of cells, which may represent different pulp cell lineages[1], indicating that there are different cell subpopulations in the primary DPSCs isolated and cultured directly, which may dominate the different cell fates of stem cells. The development and progress of cell sorting technologies make the separation of cell subsets possible.
Currently, DPSC subpopulations that have been isolated include but are not limited to side population cells with stem cell phenotypic characteristics[55], bromodeoxyuridine (BrdU)-labeled labelretaining cells for the localization of dental pulp stem/progenitor cells[56], ALDH1+ cell subpopulations reflecting DPSC niches[57], DPSCs mobilized by G-CSF (MDPCs) with high proliferation rates and stability[58], CD34-/CD34+ DPSCs with different neural differentiation potentials[59], thy-1-positive cells in the subodontoblastic layer with the ability to differentiate into hard tissue-forming cells[60], and CD271+ dental MSCs with high odontogenic potential[61]. These subsets reflect the origin or location of stem cells or have high potential in a particular direction of differentiation. For example, a group of unique multipotent stem cells were recently identified from mouse dental papilla called multipotent dental pulp regenerative stem cells, exhibiting enhanced osteogenic/odontogenic differentiation capabilitiesin vitroandin vivoand efficiently regenerating functional pulpo-dentinal complexlike tissuesin vivo[62]. CD146+ human DPSCs have also been reported to be able to regenerate an increased area of dentin/pulp-like structuresin vivocompared with their CD146- counterparts or mixtures of the two[63]. These results suggest that the use of DPSCs is flexible in tissue engineering, and taking advantage of a specific side group may be the pathway to achieve accurate and efficient tissue regeneration.
Regardless of the source of DPSCs, DPSCs are used in the later description of this article, and no special distinction is made when describing their applications in regenerative medicine.
DERlVATlVES OF DPSCS
Stem cell-based tissue engineering has been developed for many years, during which the application forms of stem cells have undergone major changes from primitive cells to genetically modified cells and from discrete stem cell suspensions to multicellular units, prompting regenerative medicine to take a big step forward. Here, we will discuss several main derivatives of DPSCs derived from long-term application, including cell injections, genetically modified cells, cell sheets and cell spheroids, and introduce their formation background, preparation techniques, biological characteristics and examples of their application in regenerative medicine.
DPSC injections
The transplantation of DPSCs has been investigated as a potential therapy for a variety of injuries and diseases, including but not limited to stroke[64], spinal cord injury[65], cerebellar ataxia[66], retinal degeneration[15], diabetic neuropathy[67], parotid gland injury[68], cystitis[69], Sjögren syndrome[70],etc. In the treatment of these diseases using DPSCs, injection is one of the more commonly used forms.Stem cell injections are the easiest cell therapy products to prepare, and the commonly used vehicles at present for resuspension of stem cells is phosphate-buffered saline[69-73], Hank's Balanced Salt Solution[15], normal saline[14,67,74-76], and modified medium[66,68,77-79]. These mediators have no therapeutic effect and only serve as transport vectors for stem cells, so it is possible to observe the monotherapy effect of transplanted stem cells and rule out the influence of carriers. In addition, DPSC injections are usually administered by local injection[15,66,69,80], intramuscular injection[67,76,81] and intravenous injection[67,68,72,82]. Different methods of administration lead to different systemic distributions and different efficacies.
A study by Kimet al[83] indicated that intravenously injected human DPSCsviathe tail vein in nude mice were distributed mostly to the lungs and rarely detected in other organs at all observed time points[83]. Another study confirmed that intravenously administered DPSCs did not show liver and kidney migration in Sprague-Dawley rats[72]. However, another study suggested that SHED transplantationviathe tail vein in nonobese diabetic mice was observed mainly in the liver and spleen[70]. The mode of administration by intravenous injection can be seen to possibly cause drug distribution in multiple organs. However, locally administered DPSCs rarely migrated to other organs over time,e.g., DPSCs were transplanted into the pulp chamber[83]. This result indicated a differential distribution pattern of transplanted DPSCs between the intravenous and local injections. Both intravenously and locally injected DPSCs have been shown to improve symptoms of various lesions[15,72,76,80]. DPSCs have also been shown to migrate and integrate into the site of injuries[15,69,73,74] and differentiate into corresponding cells[68,72,75,79,84].
Shahaniet al[71] traced the biodistribution of intramuscularly transplanted human DPSCs in immunocompetent healthy rats. The results showed that DPSCs started entering into the blood vessels adjacent to the muscle at hour 24 and gradually metastasized, but the signal intensity in the muscles at the injection site remained highest, serving as a repository for DPSCs in transplantation. Intramuscular injection also avoids the lung “first pass effect” compared with intravenous injection, prolonging the survival of transplanted stem cells in the body and thus providing a sustained delocalized benefit for systemic diseases[71]. Dattaet al[67] compared the effects of intramuscular and intravenous injection of DPSCs on diabetic neuropathy, and a more rapid improvement in neuropathic symptoms was observed for DPSC intravenous transplantation. However, DPSC intramuscular injection, especially after repeated administration, maintained the improved inflammatory state[67]. The study of Hataet al[14]also confirmed that the therapeutic effects of DPSC transplantation with a single intramuscular injection lasted for prolonged periods[14], further demonstrating the continued efficacy of DPSC intramuscular administration. Another study demonstrated that the efficacies of DPSC intramuscular transplantation were limited to the administration site, but it was difficult to play a role on the opposite side[81],possibly related to the number of DPSCs that migrated.
In summary, intravenously administered DPSCs are distributed mainly in the lungs and can also be transferred to the injured area; however, locally injected DPSCs are less likely to migrate to other parts of the body, whereas intramuscularly injected DPSCs may enter into the blood vessels and metastasize but are distributed mainly in the local muscles and less in the lungs and persist longerin vivo.Intravenous administration works more quickly than intramuscular administration, but the effects of intramuscular transplantation last longer, while the effect of local injection is mostly limited to the site of administration. In conclusion, regardless of the injection mode, DPSC injections have shown certain therapeutic effects in the treatment of various diseases.
Modified DPSCs
The combination of cell therapy and genetic engineering has resulted in genetically engineered cells,which are considered to have greater prospects of therapeutic potential and efficient treatment than nonengineered cell therapy approaches[85]. Although there are still many factors to consider before genetically modified stem cells can be directly used in regenerative medicine[86], gene therapy, as an increasingly mature discipline, has profoundly influenced the development of regenerative medicine.Genetically engineered cell therapy using primary cells that overexpress tissue-specific or therapeutic genes makes it possible to produce therapeutic proteins at sites of regeneration or to differentiate new cells into the desired cellular lineage and thus promote tissue regeneration[87]. Obtaining the carrier cells, genetically modifying and expanding the cellsin vitroand then using the cells for disease therapeutic strategiesin vivois a common method of applying genetically engineered cell therapy[88].Genetically engineered cell therapy often uses MSCs as gene delivery vectors due to their accessibility for genetic modificationin vitroand their ability to be cultured and expandedin vitro[85,87-89]. DPSCs,a type of MSC, are characterized by self-renewal, multipotent differentiation potential and amplificationin vitro, as well as easy access, low risk of immune rejection and fewer ethical issues; DPSCs are also considered ideal gene vehicles with wide application prospects[16].
Compared with unmodified DPSCs, genetically modified DPSCs have been shown to be more potent in treating various diseases. For instance, compared with DPSCs, DPSCs overexpressing hepatocyte growth factor have been shown to dramatically relieve the disease activity of dextran sulfate sodiuminduced ulcerative colitis[16], promote improvements in postischemia/reperfusion brain injury[90],promote the grafted DPSC-induced hepatic functional recovery from liver cirrhosis in a rat model[91],significantly improve periodontal bone regeneration in swine[92] and have a stronger capacity to significantly reduce ovariectomy-induced bone loss in the trabecular bone of the distal femur metaphysis[93]. Similarly, Rizket al[94] engineered sizable three-dimensional (3D) cartilage-like constructs using human DPSCs, and the results showed that constructs with transforming growth factor(TGF)-β3-DPSCs showed higher collagen type II and Sox9 mRNA expression than nontransduced DPSC constructsin vivo[94]. Gene therapy using Runx2-modified DPSCs has also been reported to be more effective in tibial distraction osteogenesis during bone deposition and new bone formation[95].
These studies indicated that genetically modified DPSCs can not only play the role of DPSCs themselves but also secrete specific therapeutic proteins to enhance their therapeutic effects, which is a major direction of innovative applications of DPSCs.
DPSC sheets
Recently, as a cell transplantation system that requires no scaffolds or carriers, cell sheet engineering has gradually become the research focus of regenerative medicine based on cell therapies and has been used for regenerative treatment of the esophagus, cornea, heart,etc[96-98]. In contrast to conventional tissue engineering approaches, cell sheet technology allows cell harvest as a continuous cell sheet with intact extracellular matrix (ECM) proteins and cell-cell junctions, which facilitates cell transplantation without any other artificial biomaterials[99]. Compared with the traditional tissue engineering of cell suspensions combined with bioscaffolds, cell-sheet transplantation can better fix the transplanted cells at the graft site without considering the negative effects of scaffold material degradation[100,101]. In this trend, DPSC sheets also emerged.
According to previous reports, the initial study used temperature-responsive cell culture dishes to prepare the DPSC sheet and used it to successfully reconstruct the corneal epithelium[102]. The dish responds to temperature changes, allowing the formed DPSC sheets to automatically shed. Subsequent studies also confirmed that DPSC sheets can be prepared within 3-4 d using temperature-responsive cell culture dishes[103,104]. Although this method is not time-consuming, it requires the use of special materials and complicated production procedures, which limit its expanded use. Therefore, some researchers have developed a method of using vitamin C (VC) to induce DPSCs to form cell sheets[105],and it has gradually become the mainstream preparation method.
VC is an essential micronutrient for humans, a potent antioxidant and a cofactor for a family of biosynthetic and gene regulatory enzymes, and VC plays an important role in supporting the function of the immune system[106]. VC also plays a key role in the biosynthesis of collagen and other ECM constituents[107,108] and promotes the proliferation of stem cells without affecting their differentiation potential[109]. Therefore, some researchers have predicted that VC alone may induce cell sheet formation, streamline production procedures or avoid using special materials, and confirmed this prediction with their studies, developing a simple and inexpensive VC-mediated procedure to obtain MSC sheets[105]. The authors also explored the mechanism of VC-induced cell sheet formation, and the optimal dose of VC showed that VC is capable of inducing telomerase activity in MSCs, leading to upregulated expression of ECM and stem cell markers. Meanwhile, VC induces MSCs to form cell sheets in a dose-dependent manner, and 20 μg/mL VC is the optimal concentration for complete cell sheets with a high level of success. However, in the existing reports, the concentration of VC alone to induce DPSCs to form sheets ranged from 10 μg/mL to 100 μg/mL[110-114], incubated continuously for 10-15 d or until the edge of the cell sheet became slightly rolled up or spontaneously detached from the bottom of the dish, all of which resulted in the formation of operable sheets consisting of 2-3 layers of cells. It has even been reported that the harvested whole DPSC sheet contained five or six layers of cells[17]. Although the use of VC has the above characteristics, the time-consuming disadvantage is also very prominent.
In addition, some other studies have seeded cells on the surface of the amniotic membrane (AM)[115,116] or even directly cultured them in basic medium[117] to obtain DPSC sheets. For example, after DPSCs were seeded on the amniotic membrane and cultured for 2 wk, the cells became confluent and formed 1-3 layers of cell sheets that adhered to the basement membrane AM[115]. DPSC sheets have also been reported to be composed of multilayer cells forming after 4 wk of culture in basal medium[117]. In addition to the above cell sheet preparation techniques, more recently, scholars have also used techniques such as near infrared triggering, light induction, and the combination of rough surfaces with thermoresponsive polymers to accelerate or improve the formation of cell sheets[118-120]. These techniques need to be further applied to the preparation of DPSC sheets.
To date, use of DPSC sheets has been reported for the regenerative treatment of a variety of injuries,including but not limited to dental pulp diseases[112], periodontal tissue diseases[121], bone defects[122], nerve injuries[123,124],etc., and all of these applications have achieved significant results. In one representative clinical study, autologous DPSC sheets from deciduous teeth were transplanted into injured young permanent teeth due to trauma. This transplantation was able to regenerate whole dental pulp, increase the length of the root and reduce the width of the apical foramen at 12 mo after treatment[125]. Furthermore, the evaluation of DPSC sheets in a rat facial nerve crush injury modelin vivoestablished that in comparison to untreated controls, nerves treated with dental pulp cell sheets had greater axon regeneration through the injury site and superior functional recovery as quantitatively assessed by compound muscle action potential measurements, possibly because the DPSC sheets can highly express neurotrophic factor (NTF) and continuously deliver the NTF to sites of peripheral nerve injury[123]. Moreover, bioengineered teeth using human DPSC aggregates combined with decellularized tooth matrix or avulsed teeth after traumatic dental injuries can regenerate 3D dental pulp and periodontium equipped with vasculature and innervation in both a preclinical pig model and a pilot clinical trial for treating tooth avulsion[126].
In summary, in cell-based regenerative medicine, the application of cells into the injured site using cell sheets shows a significant increase in the therapeutic effect compared to dissociated cell injections,which may be related to the form of cell sheets being able to provide a large number of seed cells and improve the survival rate of transplanted cells[127,128]. DPSC sheets have also been reported to be more effective in repairing periodontal bone defects and regenerating soft tissue than pulp stem cell injections[17]. Moreover, the applications of decellularized cell sheets suggest that in addition to the function of seed cells in the sheets, extracellular matrix may also play a certain role in regeneration[129]. For example, a decellularized matrix of DPSC sheets can promote the proliferation and osteogenic differentiation of inoculated human periodontal ligament stem cells[130].
DPSC spheroids
Most studies in cell biology are performed on a two-dimensional (2D) culture basis, although these studies facilitate microscopic analysis and medium changes and sustain cell proliferation for most cell types. However, this is generally not considered the natural microenvironment of the cells[131]. A cell spheroid is a 3D aggregation of cells, which is considered to be closer to the microenvironmentin vivobecause its formation mode simulates the natural processes of cells undergoing biological self-assembly to form complex tissues with 3D architecture and intensive cell-cell contacts from the perspective of embryonic development[132]. Cell spheroids have been proven to be able to mimic the architectural and functional characteristics of native tissue. For example, liver spheroids constructedin vitroby liver cells and endothelial cells have an ultrastructure of liver tissue, such as bile canaliculus-like and Disse’s space-like structures, and show stable albumin secretion and ammonia removal activity[133]. 3D lung spheroids of outgrowth cells from healthy lung tissue explants can be expanded to a large quantity and can form alveoli-like structures and acquire mature lung epithelial phenotypesin vitro[134]. The introduction of endothelial cells can form capillary networks in spheroids from different kinds of cells,which is conducive to anastomosing with the host vasculature after transplantation and prolonging the survival time of cell spheroids[135-137]. In view of the above characteristics, cell spheroids are widely believed to be able to be used as excellent candidates for basic units of 3D tissue engineering constructs,thus providing new strategies for tissue defect repair and reconstruction.
At present, techniques to form cell spheroids include mainly pellet culture, spinner culture, hanging drop (HD), liquid overlay, rotating wall vessel, external force, microfluidics, micromolded nonadhesive hydrogels[138], microwell culture, medium regulation, bioreactors[139] and bioactive materials such as cellulose hydrogel film[140,141]. There are also methods to generate cell spheroids by using cell sheets as prophase tissues[142] or culturing in specific charged culture dishes based on polyion complex nanoparticles[143]. Some of these methods are still in the research stage and are not ready to be adopted for large-scale manufacturing. The manufacturing methods of DPSC spheroids have also emerged in an endless series, including but not limited to serum-free medium culture[144,145], culturing on Matrigel[146], special 3D Petri dish culture[135,147], low or ultralow attachment culture plates[62,148], culturing on gelatin methacrylamine/poly(ethylene glycol) diacrylate (GelMA/PEGDA) composite hydrogels[149], coculturing with microparticles with a leaf-stacked structure based on polycaprolactone[150], HD or molded parafilm-based methods[151]. Most of these methods belong to the classification of the aforementioned technologies.
Regardless of the method, the prepared DPSC spheroids basically have spherical or spheroid-like shapes, ranging in diameter from microns to millimeters. Since the typical viable rim of cells in spheroids is approximately 100-300 μm, cells die in the center of large spheroids due to the lack of oxygen and/or nutrients, accumulation of waste products and low pH[146]. Therefore, a larger spheroid diameter is not better. Histological examination of cell spheroids at the micron level revealed that spheroids were compact throughout with small single cells evenly distributed after 24 h of culture[147], while a diversity of nuclei in the spheroids after 1 wk of culture suggested that cells in the spheroid were multitype[145]. Real-time reverse transcriptase-polymerase chain reaction analysis also demonstrated that the stemness/pluripotency markers Oct4, Sox2, NANOG, TP63, and CD44 were expressed in 3D cultured DPSCs, and the expression level was significantly increased when compared to 2D cultured DPSCs[145,147]. In addition, compared to 2D cultured DPSCs, the osteogenic,adipogenic, odontogenic differentiation potential and migration ability of DPSC spheroids are also enhanced[145,147,152-154]. These results indicate that the stemness of 3D cultured DPSCs is maintained while the multilineage differentiation potential could be enhanced, which may be related to the improvement of signal transmissions between cells.
DPSC spheroids have been proved to be able to differentiate into specific phenotypic cells, or simulate the structural and functional characteristics of the corresponding tissues, and play a therapeutic role. For example, evidence that DPSC spheroids can differentiate into neuron-like cells with potential functions under neurogenic inductionin vitrohas been reported[155]. The expression of neuronal markers such as microtubule-associated protein 2 in DPSC spheroids was increased after culture in neurogenic maturation medium or with the addition of central nervous system mitogens such as EGF and bFGF[156,157]. These DPSC spheroids are able to differentiate into functional neuronal cells and stimulate neurogenesis in the adult mouse hippocampus through neurotrophic supportin vitro[158]. Dissanayakaet al[135] also confirmed that DPSCs support the survival of the co-cultured endothelial cells, and they can self-assemble into microtissue spheroids within the microwells of an agarose mold. Combined with tooth-root slices, these prevascularized, scaffold-free, microtissue spheroids could successfully regenerate vascular dental pulp-like tissue in immunodeficient mice[135].In addition to spherical cell spheroids, there are some irregular cell aggregates constructed by 3D cell culture technology, which are still multicellular units of DPSCs in nature and have corresponding regenerative therapeutic effects. For instance, some scholars obtained rod-like 3D DPSC constructs by shaping sheet-like aggregates of DPSCs with a thermoresponsive hydrogel, which could form blood vessel-rich pulp-like tissues in nude mice[159].
If the cell sheet is still a cell aggregate in a two-dimensional concept, cell spheroids are advancing the concept of 3D tissue engineering. In 3D cell spheroids, cells are in close contact with each other and surrounded by extracellular matrix, enabling the simulation of cell-to-cell interactions and cellextracellular matrix interactionsin vitro. These processes are very important for signal transmission between cells and guiding cell behaviors such as movement, proliferation and differentiation[138].Current studies have confirmed that these characteristics can enhance the properties of DPSCs in 3D cell spheroids, more studies are needed to explore the therapeutic advantages of DPSC spheroids compared with other DPSC products.
The above derivatives based on DPSCs themselves can be used alone or in combination with bioscaffold materials for the treatment of diseases, which will not be discussed here. Figure 1 shows an overview of the main sources of DPSCs, their derivatives and examples of their applications in regenerative medicine.
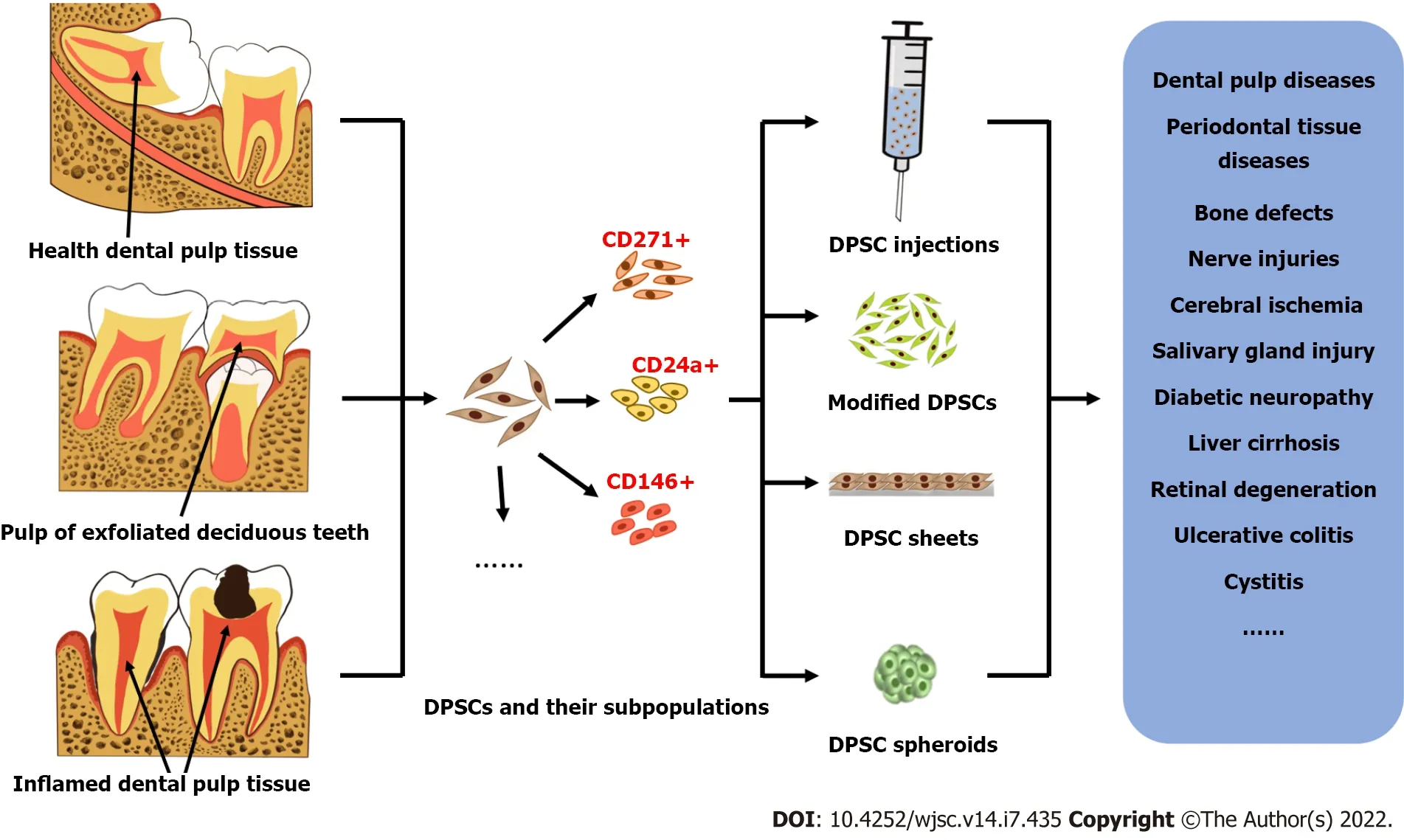
Figure 1 Overview of the main sources of dental pulp stem cells and their derivatives and examples of their applications in regenerative medicine. Dental pulp stem cells (DPSCs) can be isolated from dental pulp tissue of different ages and health statuses, such as the healthy dental pulp tissue of adult impacted teeth, the pulp of children′s exfoliated deciduous teeth, and the inflamed dental pulp tissue of patients with caries or periodontitis. Using cell sorting technologies, dental pulp stem cells can be isolated into multiple cell subsets with specific phenotypes, such as CD271+ DPSCs, CD24a+ DPSCs, and CD146+DPSCs. Several main derivatives of DPSCs derived from long-term applications, including cell injections, genetically modified cells, cell sheets and cell spheroids,which can be used in the treatment of various diseases such as dental pulp diseases, periodontal diseases, and bone defects. DPSC: Dental pulp stem cell.
MECHANlSM OF REGENERATlON PROMOTED ΒY DPSCS
Direct effects on the regeneration process
For years, scholars have failed to fully understand the fate of implanted injured stem cells and their role in regeneration. The results of some studies show that the implanted stem cells can stayin situand differentiate into corresponding cells, thus directly participating in the process of regeneration[25-29].Researchers have preliminarily revealed this process through stem cell labeling techniques, such as green fluorescent protein (GFP)/BrdU labeling[26], superparamagnetic iron oxide[160], and fluorescence-based tracing[161]. For example, BrdU-labeled MSCs migrated into the entire periodontal tissue, including the periodontal ligament, alveolar bone, cementum and blood vessels, and differentiated into periodontal ligament fibroblasts and osteoblasts 6 wk after implantation in periodontal defects, confirming that MSC transplantation has the potential to regenerate periodontal tissue and that transplanted MSCs are at least partially directly involved in the formation of new tissue[29]. The findings of Hasegawaet al[25] also supported this conclusion[25]. Another example is the combination of Dil (a fluorescent dye) or GFP-prelabeled hESC-MSCs with the simulated tendon complex to form tissue-engineered tendons, which were then ectopically transplanted into the back of nude mice or orthotopically transplanted into the impaired rat Achilles tendon. Four weeks after transplantation, the transplanted MSCs partially survived and differentiated into the tenocyte lineage, and functional tendons were regenerated successfully[27].
Similarly, transplanted DPSCs have been proven to be partially involved directly in the process of tissue regeneration. For instance, 5 wk after DPSCs stably transduced with GFP, GFP-DPSCs were seeded into tooth slices/scaffolds and transplanted into the subcutaneous space in the dorsum of immunodeficient mice. The DPSCs were observed to differentiate into endothelial cells and form neovascularization anastomosed with host vessels by immunohistochemistry and immunofluorescence staining. This process may be related to the activation of the Wnt/β-catenin signaling pathway by vascular endothelial growth factor (VEGF)[162]. Luzuriagaet al[163] also confirmed that human CD31+/CD146+ and Nestin + DPSC-derived cells can survive 1 mo after grafting into the brains of nude mice, expressing CD31 and VEGF, forming full blood vessels of human origin and integrating into the host brain vasculature[163]. In short, these results suggest that transplanted stem cells can partially survive and directly participate in the process of tissue repair and regeneration.
Immunomodulatory effects
In addition, stem cell transplantation has also shown promising results in the treatment of immunerelated diseases[164,165], which suggests that stem cell transplantation may be involved in the process of immune regulation in the host. Previous studies have confirmed that MSCs have the characteristics of immunosuppressionin vivoandin vitroand are capable of regulating immune cells, such as T cells, B cells, DCs, and NK cells[21]. MSCs can efficiently suppress the proliferation of T cells[166] and reduce the production and release of cytokines such as interferon (IFN)-γ and interleukin (IL)-17[167,168].MSCs also efficiently inhibit the maturation of DCs and markedly impair a variety of functions of NK cells[169]. Furthermore, MSCs are able to inhibit the proliferation of B cells and their capacity to produce antibodies[20]. MSC-mediated immunosuppression may occurviathe concerted action of chemokines and nitric oxide (NO). In the presence of IFN-γ, TNF-α, IL-1A, or IL-1β, MSCs can be stimulated to express several chemokines at high levels and inducible NO synthase. Chemokines drive T-cell migration into proximity with MSCs, where T-cell responsiveness is suppressed by NO, while blocking chemokine receptors could abolish immunosuppression[170]. However, there is a species variation in the mechanisms of MSC-mediated immunosuppression: Immunosuppression by cytokine-primed mouse MSCs is mediated by NO, whereas immunosuppression by cytokine-primed human MSCs is executed through indoleamine 2,3-dioxygenase (IDO). The similarity is that they both exert immunosuppressionviathe concerted action of chemokines and immune-inhibitory NO or IDO[19].
DPSCs have also been found to have immunomodulatory functions similar to those functions in MSCs. Therefore, DPSCs are considered promising candidates for cell therapy for a variety of immuneand inflammation-related diseases. Previous reports have demonstrated that DPSCs can suppress T cell proliferation and therefore might be suitable for preventing or treating T cell alloreactivity associated with hematopoietic or solid-organ allogeneic transplantation. The study also confirmed that DPSCs had a stronger inhibitory effect on the T cell response than BMSCs[171]. In addition, DPSCs can also inhibit acute allogeneic immune responses by their release of TGF-β as a result of allogeneic stimulation of T lymphocytes[172] and inhibit the proliferation of peripheral blood mononuclear cells (PBMCs)viathe expression of soluble factors partly induced by the secretion of IFN-γ by activated PBMCs[173]. In another study, Toll-like receptors, key molecules that bridge the innate and adaptive immune responses,were shown to trigger the immunosuppression of DPSCs by upregulating the expression of TGF-β and IL-6[174]. In addition, DPSCs could induce activated T cell apoptosisin vitroand ameliorate inflammation-related tissue injuries in mice with colitis, which was associated with the expression of the Fas ligand (FasL). Knockdown of FasL expression reduced the immunoregulatory properties of DPSCs in the context of inducing T cell apoptosis[21]. These studies indicate that DPSCs exert their immunoregulatory functions mainly by inhibiting immune cells, especially T cells, including inhibiting proliferation,reducing the release of cellular inflammatory factors, and inducing apoptosis.
Paracrine effects
However, the proposal of secretomes, exosomes or EVs provides a new direction for us to understand how stem cells promote regeneration: Paracrine cues and derives a cell-free tissue engineering strategy.Many studies have confirmed that conditioned media/secretomes/exosomes/EVs from BMSCs, DPSCs or other types of stem cells can perform functions similar to the functions of stem cells themselves,promote the regeneration of damaged tissue or improve the severity of the disease[18,31,175,176].Exosomes from different MSCs have been reported for the treatment of liver disease, kidney disease,cardiovascular disease, neurological disease, immune disease, and skin wounds[24,177]. Exosomes from MSCs may accomplish changes in the cellular microenvironment and the behavior of their neighboring cells by transferring factors that modulate different metabolic and signaling pathways, such as the maintenance of a dynamic and homeostatic environment and the ability to activate angiogenesis, proliferation, migration and differentiation of the main cell types involved in regeneration, thereby restoring tissue homeostasis and enabling cells within the tissue to recover, repair and regenerate[24,177]. In addition, some scholars believe that paracrine signaling is mainly responsible for the involvement of MSCs in the modulation of immune responses and the progression of diseases. Through the release of secretomes consisting of a diverse range of cytokines, chemokines, and EVs, MSCs convey regulatory messages to recipient immune cells in the microenvironment[178]. DPSC-derived exosomes have also been shown to alleviate cerebral ischemia-reperfusion injury by suppressing inflammatory responses,such as reducing the protein expression of IL-6, IL-1β, and TNF-α[18], suggesting that the immunomodulatory effect of stem cells may also be achieved through the paracrine pathway.
In conclusion, DPSCs may promote tissue repair and regeneration by directly differentiating into corresponding cells, exerting immunomodulatory effects, or by releasing paracrine substances such as exosomes to maintain microenvironment homeostasis and activate the functions of adjacent cells.
CONCLUSlON
According to published data, DPSCs have become one of the important seed cells of regenerative medicine. Younger DPSCs, such as DPSCs from natal teeth or SHED, are more suitable as excellent candidates for regenerative medicine stem cell resource banks. However, due to the lack of abundant sources of natal teeth, SHED may become the most powerful source of DPSCs in the future. The establishment of a stem cell bank for SHED is an urgent problem to be solved. In addition, taking advantage of a specific side group of DPSCs may be the pathway to achieve accurate and efficient tissue regeneration. However, this does not mean that the use of the total population of DPSCs is meaningless.The possible reason could be that the tissue is composed of a variety of cells with different functions,and a certain subpopulation currently reflects only one or a few of its dominant functions. The use of a subpopulation may not be sufficient to regenerate well-organized native-like tissue. Therefore, the combined use of several side groups may be more sensible DPSCs can be used in the treatment of diseases in the form of single injections, cell sheets and cell spheroids, and their therapeutic effect can be enhanced by gene modifications. DPSC injections may be a useful method for the treatment of systemic diseases, but for the treatment of localized damaged tissue, which requiresin situtissue regeneration,how to keep the implanted DPSCsin situis worth considering; therefore, cell sheets and cell spheroids with supports are more suitable in this case. Current data show that DPSCs may promote the improvement, repair and regeneration of diseased and injured tissues by means of immune regulation,paracrine signaling and direct differentiation into corresponding cells to occupy the injured site.However, the mechanism by which DPSCs promote regeneration is complex, and the above discussion does not address all of the mechanism. We should continue to pay attention to the new applications of DPSCs and improve the mechanism by which DPSCs promote diseased tissue recovery.
FOOTNOTES
Author contributions:Yuan SM wrote the paper and drew the figure; Yang XT revised the original manuscript;Zhang SY reviewed the manuscript and revised the language; Tian WD and Yang B proposed the ideas and approved the manuscript to be published.
Supported byNational Natural Science Foundation of China, No. U21A20369; Sichuan Science and Technology Program, No. 2021YJ0147; and Research and Develop Program, West China Hospital of Stomatology Sichuan University, No. RD-02-202113.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Sheng-Meng Yuan 0000-0003-0585-514X; Xue-Ting Yang 0000-0002-0013-2893; Si-Yuan Zhang 0000-0002-6214-3459; Wei-Dong Tian 0000-0003-0175-1132; Bo Yang 0000-0003-0127-9632.
S-Editor:Fan JR
L-Editor:A
P-Editor:Fan JR
杂志排行

World Journal of Stem Cells的其它文章
- Role of hypoxia preconditioning in therapeutic potential of mesenchymal stem-cell-derived extracellular vesicles
- Application of exosome-derived noncoding RNAs in bone regeneration: Opportunities and challenges
- Metabolic-epigenetic nexus in regulation of stem cell fate
- Stem cell therapy for insulin-dependent diabetes: Are we still on the road?
- Prodigious therapeutic effects of combining mesenchymal stem cells with magnetic nanoparticles
- Application of extracellular vesicles from mesenchymal stem cells promotes hair growth by regulating human dermal cells and follicles