Endoscopic ultrasound-guided gallbladder drainage in pancreatic cancer and cholangitis: A case report
2021-01-11GermanadeNucciNicolaImperatoreDesireePicasciaEnzoDomenicoMandelliCristinaBezzioIlariaArenaBarbaraOmazziAlbertoLarghiGianpieroManes
Germana de Nucci, Nicola Imperatore, Desiree Picascia, Enzo Domenico Mandelli, Cristina Bezzio, Ilaria Arena, Barbara Omazzi, Alberto Larghi, Gianpiero Manes
Abstract BACKGROUND Head pancreatic cancers often present with clinical challenges requiring biliary drainage for chemotherapy or palliative scope. If usual endoscopic modalities fail or if percutaneous approach is not feasible, endoscopic ultrasound (EUS) guided biliary drainage can be considered. Here we describe and discuss an interesting clinical case in which EUS-guided gallbladder drainage (EUS-GBD) was chosen to treat acute severe cholangitis in a patient with advanced pancreatic cancer.CASE SUMMARY An 84-year-old female with a previous EUS-biopsy proven diagnosis of head pancreatic cancer presented with clinical signs of acute cholangitis. In September 2018 she had positioned a biliary and duodenal stent to relieve jaundice and an initial duodenal substenosis. In the emergency ward, an abdominal computed tomography scan showed proximal biliary stent occlusion due to neoplastic progression, but endoscopic retrograde cholangiopancreatography was impossible because of worsening duodenal stenosis and the absence of a chance to reach the Vater’s papilla area. EUS-guided choledocoduodenostomy was not technically feasible but because the cystic duct was free of neoplastic infiltration,an EUS-GBD using an Axios™ stent was successfully performed. The patient started to feed after 48 h and was discharged 1 wk later. No other hospitalizations due to cholangitis or symptoms of Axios™ stent occlusion/dysfunction were observed up until her death 6 mo later due to underlying disease.CONCLUSION This case demonstrated how different EUS therapeutic approaches could have a key role to treat critical and seemingly unsolvable situations and that they could play a more fundamental role in the next future.
Key Words: Gallbladder drainage; Endoscopy ultrasound; Pancreatic cancer; Cholangitis;Case report; Axios stent
INTRODUCTION
Malignant neoplasms of the pancreatic head often present with clinical challenges requiring biliary drainage before upfront chemotherapy or palliative treatment[1].When endoscopic retrograde cholangiopancreatography (ERCP) fails due to anatomical or technical difficulties, the use of endoscopic ultrasound (EUS)-guided biliary drainage could be more appropriate than the percutaneous approach[2].Moreover, some authors have proposed EUS-guided gallbladder drainage (EUS-GBD)as another alternative to drain the biliary tree if the cystic duct is not entrapped by neoplastic tissue[3,4]. Gallbladder drainage has been simplified by the development of dedicated enhanced lumen-apposing self-expandable metallic stents that create a stable fistula between the gallbladder and the lumen of the stomach or the duodenum.This approach has been recently reported to be more effective than percutaneous drainage to treat high-risk surgical patients with acute cholecystitis[5]. We herein report a case of a patient with a known pancreatic head cancer already previously treated with endoscopic stenting who required urgent biliary decompression through cholecystoduodenostomy for severe acute cholangitis.
CASE PRESENTATION
Chief complaints
An 84-year-old female presented to our Emergency Unit with fever (max 39.5 C),jaundice and leukocytosis.
History of present illness
The clinical data suggested a diagnosis of acute cholangitis due to the occlusion of a biliary metal stent positioned previously.
History of past illness
In September 2018, the patient had a diagnosis of an EUS biopsy proven unresectable pancreatic head cancer with biliary, and a duodenal stent was placed to relieve jaundice and symptomatic duodenal substenosis.
Personal and family history
She had a familial history of colorectal ca ncer (her sister).
Physical examination
On presentation her vital signs were temperature of 39.5 °C, pulse of 115 bpm,respiratory rate of 17 rpm, blood pressure of 80/50 mmHg and oxygen saturation of 92%. On general physical examination she looked pale and dehydrated. Abdominal examination revealed nondistended, tender abdomen in the right hypochondrium with a reduction of bowel sounds. The cardiovascular, pulmonary and neurological examination were unremarkable.
Laboratory examinations
Complete blood count analysis revealed a huge increase of the white blood cells (24754 cells/mL) and a significant increase of liver cytolysis and cholestasis enzymes:Aspartate aminotransferase 123 U/L, alanine aminotransferase 234 U/L and gammaglutamyltransferase 431 U/L.
Imaging examinations
Abdominal computed tomography scan showed proximal biliary stent occlusion due to neoplastic progression with presence of stones above it. An ERCP was attempted,but access to the biliary tree was impossible because of worsening duodenal stenosis with complete incorporation of the metallic duodenal stent.
MULTIDISCIPLINARY EXPERT CONSULTATION
In an effort to avoid placement of a percutaneous drainage and due to the presence of new metastatic hepatic lesions, a multidisciplinary team discussed the case and decided to propose a further EUS evaluation with the aim of performing an alternative drainage procedure.
FINAL DIAGNOSIS
Acute cholangitis due to biliary metallic stent occlusion in advanced pancreatic cancer with duodenal infiltration and stenosis.
TREATMENT
Because of the absence of a suitable sonographic window above the biliary obstruction,EUS-guided choledocoduodenostomy was not technically feasible. On the other hand,the cystic duct appeared to be free of neoplastic infiltration, thus we decided to perform an EUS-GBD using an Axios™ stent plus electrocautery enhanced delivery system. The gallbladder was best visualized from the duodenum and penetrated with EC-Axios by applying cautery. A 10 mm × 10 mm Axios™ stent (Figure 1 and Video 1)was placed under EUS guidance from the duodenal bulb through the stent wire meshes into the gallbladder.
OUTCOME AND FOLLOW-UP
The procedure was technically successful without short- and long-term adverse events(Figure 2) and with a dramatic decrease in bilirubin concentration (2.7 mg/dL) and progressive normalization of inflammatory indexes. The patient started to feed after 48 h and was discharged 1 wk later after full antibiotic treatment was completed. No other hospitalizations due to cholangitis or symptoms of the Axios™ stent occlusion/dysfunction were observed before the patient died due to her underlying disease 6 mo later.
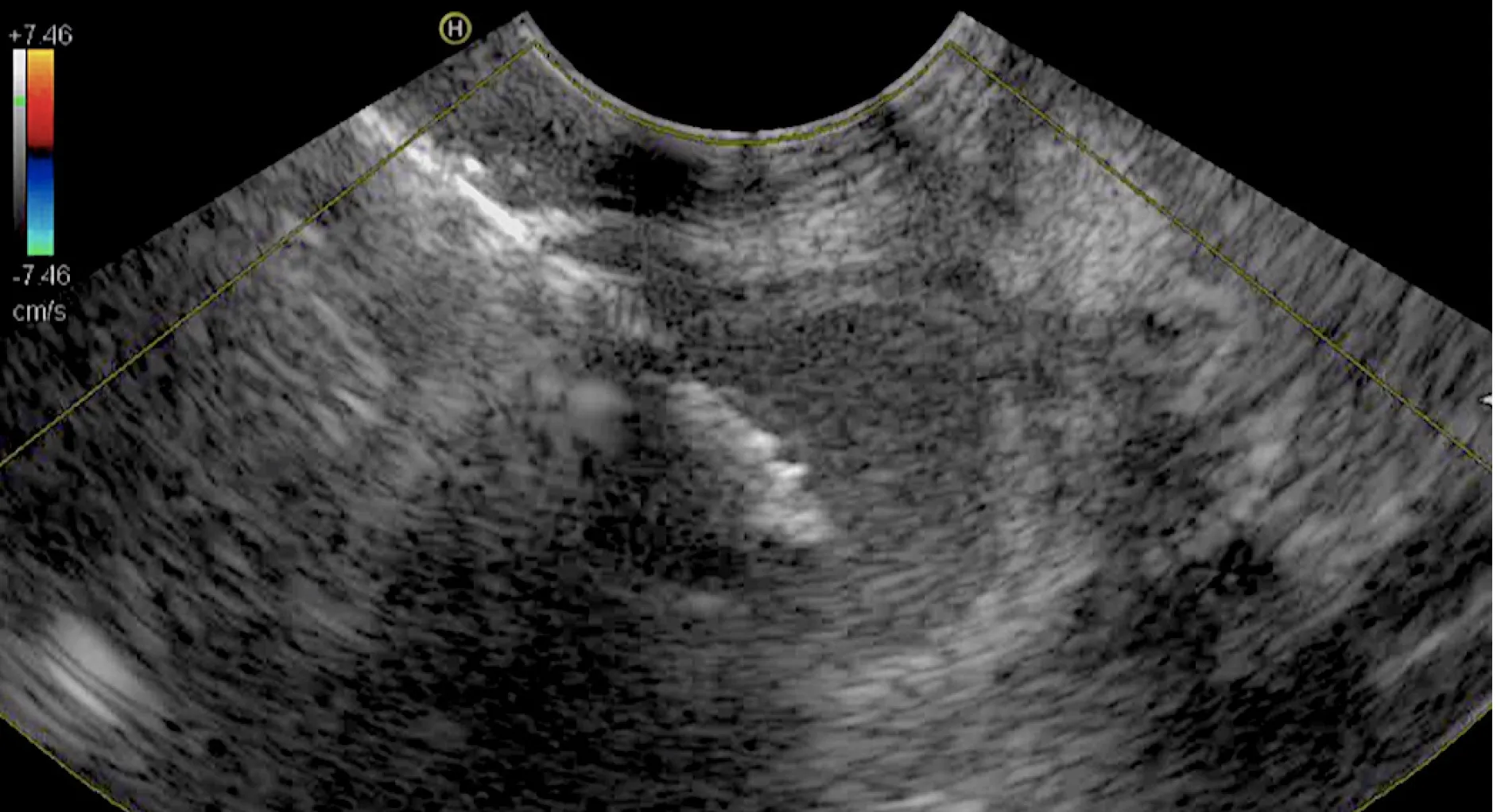
Figure 1 Endoscopic ultrasound guided wound of the gallbladder through the duodenal bulb.
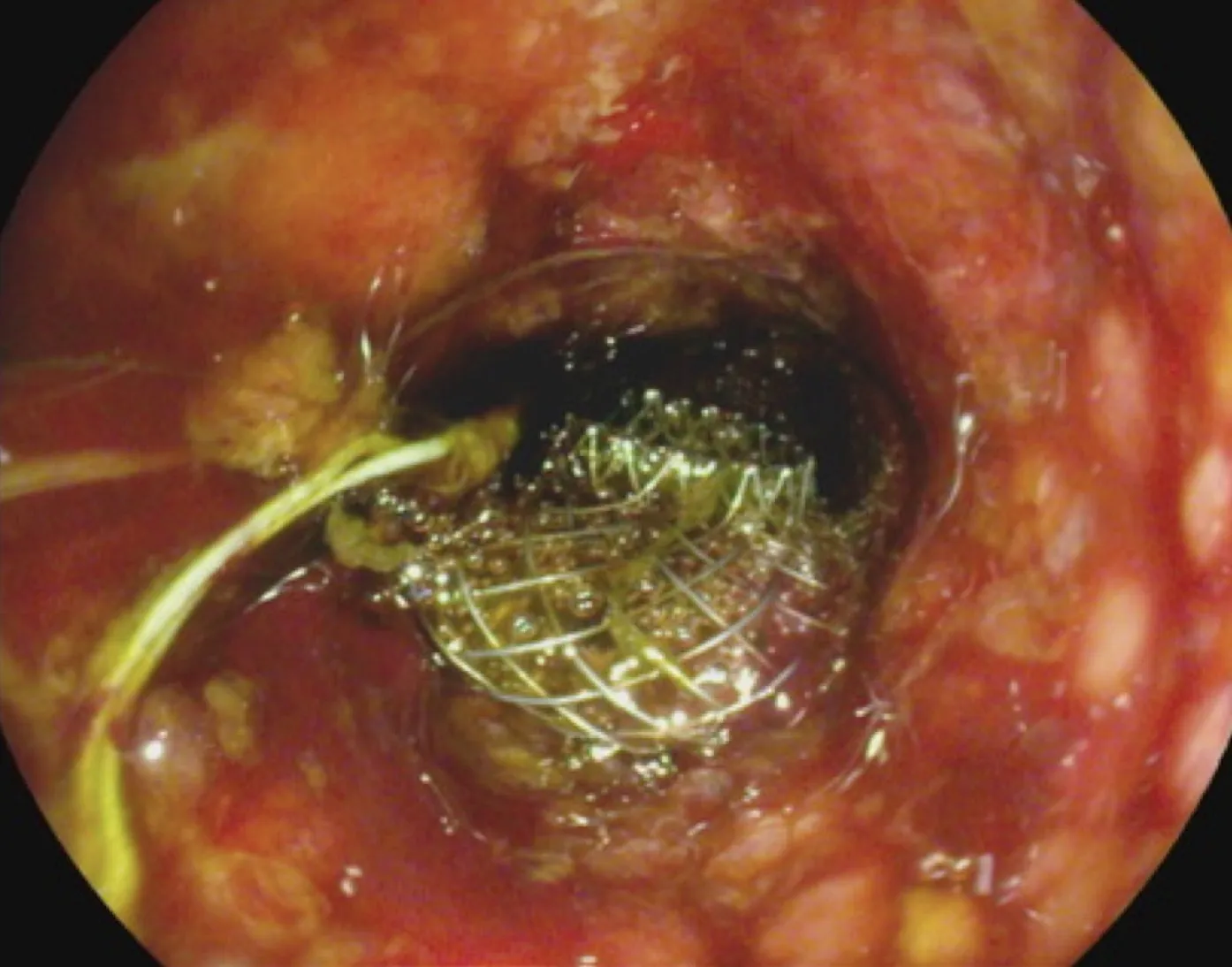
Figure 2 Endoscopic view of gallbladder drainage.
DISCUSSION
ERCP is the gold standard to treat obstructive jaundice due to malignant distal biliary obstruction[6]. However, ERCP can fail or be impossible in cases of duodenal stenosis,no access to Vater’s papilla zone or altered postsurgical anatomy. In these cases, EUSguided biliary drainage techniques, such as EUS-guided rendezvous, EUS-guided choledochoduodenostomy and EUS-guided hepaticogastrostomy are all recognized alternative modalities that have a better outcome than percutaneous drainage[7,8].
Recently, several studies demonstrated that EUS-GBD is useful to treat acute cholecystitis in patients unfit for surgery because of its similarity to percutaneous transhepatic gallbladder in terms of efficacy and safety[9]. Thus, when ERCP and EUSbiliary drainage cannot be performed for technical reasons, EUS-GBD may be a suitable alternative given that the gallbladder is a large organ with better accessibility by EUS from the gastric antrum or duodenal bulb[10].
The key factor to perform an effective EUS-GBD in this clinical scenario was lack of involvement of the cystic duct by the tumor. In our case, we performed EUS-GBD as a rescue procedure to treat severe acute cholangitis in a patient with advanced pancreatic neoplasia, in whom previous biliary and duodenal stenting were done.Before performing drainage, careful visualization of the pancreatic mass and lack of involvement of the cystic duct were done, followed by the drainage procedure that was technically and clinically successful as demonstrated by the rapid decrease of the patient’s inflammatory indexes, disappearance of the septic status and normalization of the bilirubin. The persistent clinical success was demonstrated by the absence of further episodes of jaundice or cholangitis.
CONCLUSION
In conclusion, our report showed that EUS-GBD could be a useful option to obtain an effective biliary drainage in patients in which conventional ERCP or EUS-guided choledocoduodenostomy could not be performed or were unsuccessful.
杂志排行

World Journal of Gastrointestinal Endoscopy的其它文章
- Anticoagulation and antiplatelet management in gastrointestinal endoscopy: A review of current evidence
- Peroral traction-assisted natural orifice trans-anal flexible endoscopic rectosigmoidectomy followed by intracorporeal colorectal anastomosis in a live porcine model
- Evaluation of the diagnostic and therapeutic utility of retrograde through-the-scope balloon enteroscopy and single-balloon enteroscopy
- Nonsteroidal anti-inflammatory drug effectivity in preventing post-endoscopic retrograde cholangiopancreatography pancreatitis: A systematic review and meta-analysis
- Preemptive endoluminal vacuum therapy after pancreaticoduodenectomy: A case report
- Curling ulcer in the setting of severe sunburn: A case report