Peroral traction-assisted natural orifice trans-anal flexible endoscopic rectosigmoidectomy followed by intracorporeal colorectal anastomosis in a live porcine model
2021-01-11HongShiSuYuChenZhaoFeiXieRuiHuangJiaLiJiangJuanLinFangFenDongJiaXiangXuZhiLiFangJunJieBaiBenLuo
Hong Shi, Su-Yu Chen, Zhao-Fei Xie, Rui Huang, Jia-Li Jiang, Juan Lin, Fang-Fen Dong, Jia-Xiang Xu, Zhi-Li Fang, Jun-Jie Bai, Ben Luo
Abstract BACKGROUND Compared to traditional open surgery, laparoscopic surgery has become a standard approach for colorectal cancer due to its great superiorities including less postoperative pain, a shorter hospital stay, and better quality of life. In 2007,Whiteford et al reported the first natural orifice trans-anal endoscopic surgery(NOTES) sigmoidectomy using transanal endoscopic microsurgery. To date, all cases of NOTES colorectal resection have included a hybrid laparoscopic approach with the use of established rigid platforms.AIM To introduce a novel technique of peroral external traction-assisted transanal NOTES rectosigmoidectomy followed by intracorporeal colorectal end-to-end anastomosis by using only currently available and flexible endoscopic instrumentation in a live porcine model.METHODS Three female pigs weighing 25-30 kg underwent NOTES rectosigmoid resection.After preoperative work-up and bowel preparation, general anesthesia combined with endotracheal intubation was achieved. One dual-channel therapeutic endoscope was used. Carbon dioxide insufflation was performed during the operation. The procedure of trans-anal NOTES rectosigmoidectomy included the following eight steps: (1) The rectosigmoid colon was tattooed with India ink by submucosal injection; (2) Creation of gastrostomy by directed submucosal tunneling; (3) Peroral external traction using endoloop ligation; (4) Creation of rectostomy on the anterior rectal wall by directed 3 cm submucosal tunneling; (5)Peroral external traction-assisted dissection of the left side of the colon; (6) Transanal rectosigmoid specimen transection, where an anvil was inserted into the proximal segment after purse-string suturing; (7) Intracorporeal colorectal end-toend anastomosis using a circular stapler by a single stapling technique; and (8)Closure of gastrostomy using endoscopic clips. All animals were euthanized immediately after the procedure, abdominal exploration was performed, and the air-under-water leak test was carried out.RESULTS The procedure was completed in all three animals, with the operation time ranging from 193 min to 259 min. Neither major intraoperative complications nor hemodynamic instability occurred during the operation. The length of the resected specimen ranged from 7 cm to 13 cm. With the assistance of a transumbilical rigid grasper, intracorporeal colorectal, tension-free, end-to-end anastomosis was achieved in the three animals.CONCLUSION Peroral traction-assisted transanal NOTES rectosigmoidectomy followed by intracorporeal colorectal end-to-end anastomosis is technically feasible and reproducible in an animal model and is worthy of further improvements.
Key Words: Transanal; Natural orifice trans-anal endoscopic surgery;Rectosigmoidectomy; Intracorporeal anastomosis; External traction
INTRODUCTION
Compared to traditional open surgery, laparoscopic surgery has become a standard approach for colorectal cancer due to its great superiorities including less postoperative pain, a shorter hospital stay, and better quality of life. Since the first report of its clinical application in 1991, an increasing number of minimally invasive surgical techniques, including single-incision laparoscopic surgery (SILS),needlescopic surgery (NS), and natural orifice transluminal endoscopic surgery(NOTES), have been developed rapidly. Of these, only NOTES can provide an opportunity for incision-free abdominal surgery. Although NOTES-related techniques continue to evolve, they remain mainly confined to animal models due to technical constraints and instrument limitations. In 2007, Whitefordreported the first NOTES sigmoidectomy using transanal endoscopic microsurgery. To date, all cases of NOTES colorectal resection have included a hybrid laparoscopic approach with the use of established rigid platforms. Our study aimed to introduce the novel technique of peroral external traction-assisted transanal NOTES sigmoidectomy followed by intracorporeal colorectal end-to-end anastomosis by using only currently available and flexible endoscopic instrumentation in a live swine model.
MATERIALS AND METHODS
Animal preparation
Three female pigs weighing 25-30 kg were used in this study. Preoperative work-up and bowel preparation comprised a 3-d liquid diet and a 1-d fast, followed by preoperative polyethylene glycol given orally. The induction of anesthesia was achieved by an intramuscular injection of 100 mg ketamine, 10 mg droperidol, and 1 mg atropine, and the maintenance of anesthesia was achieved by an intravenous drip of propofol at a dosage of 10 mL/h after endotracheal intubation. The heart rate and oxygen saturation of each animal were monitored during the operation. Animals were maintained in a supine Trendelenburg position to allow for optimal access and peritoneal exploration. One dual-channel therapeutic endoscope (GIF-2TQ260M,Olympus) was used. Carbon dioxide insufflation was performed during the operation.This study was approved by the Institutional Animal Use and Care Committee of Beijing Pinggu Hospital and Fuzhou General Hospital of Nanjing Military Command(IACUC-2015-010).
Peroral traction-assisted transanal NOTES sigmoidectomy followed by intracorporeal colorectal end-to-end anastomosis under trans-gastric endoscopic guidance
The anterior wall of the rectosigmoid colon was tattooed with India ink by submucosal injection under trans-anal endoscopic vision (Figures 1 and 2).
Creation of gastrostomy by directed submucosal tunneling under trans-gastric endoscopic vision: A 2-cm transversal mucosal incision was created near the gastroesophageal junction with a dual knife (KD650L; Olympus, Tokyo Japan),followed by the creation of a 3-5 cm longitudinal submucosal pelvis-directed tunnel.The tunnel ended with a seromuscular incision, and the exit site was selected at the anterior wall of the stomach.
Peroral external traction using endoloop ligation under trans-gastric endoscopic vision: An external endoloop knotted to a segment of dental floss was passed through by a twin grasperone of the accessory channels of the endoscope. Then, the dualchannel therapeutic endoscope was again advanced into the peritoneal cavity through the gastrostomy site. After abdominal exploration, the twin grasper was used to catch and pull the anterior wall of the rectosigmoid colon tattooed with India ink so that the endoloop might rope the part of the targeted colon. Once the endoloop was tightened followed by stretching of the floss, peroral external traction was achieved, allowing exposure of the sigmoid mesocolon and subsequent endoscopic dissection of the vessel and mesentery.
Creation of rectostomy on the anterior rectal wall 5 cm distal to the tattooed marker of the rectosigmoid colon by using directed short submucosal tunneling under transanal endoscopic vision: This was the same as the creation of gastrostomy.
Peroral external traction-assisted dissection of the left side of the colon under transanal endoscopic vision: With the help of peroral external traction, the sigmoid colon mesentery was mobilized off the retroperitoneum with a hook knife (model KD-620LR; Olympus). The inferior mesenteric vessels were successfully dissected using a Coagrasper (model FD-410LR; Olympus) and endoscopic clips (HX-600-135;Olympus), which was similar to the description issued by Park. After being dissected for around ten cm in length, the mobilized rectosigmoid colonic segment was transected at the site of the tunnel entrance.
Trans-anal rectosigmoid specimen transection: The mobilized rectosigmoid colon was exteriorized and transected trans-anally. A 25-mm circular stapler anvil(Medtronic) was inserted into the proximal segment after purse-string suturing, and the proximal bowel was then returned into the abdomen.
Intracorporeal end-to-end colorectal anastomosis using a circular stapler by a single stapling technique under trans-gastric endoscopic guidance: The dual-channel therapeutic endoscope was again advanced into the peritoneal cavity through the gastrostomy site. Pneumoperitoneum was reestablished, and then an endoloop was used to ligate the lateral rectostomy by endoscopy. After the stapler was inserted into the rectum and pricked the top wall of the rectum, a trans-umbilical rigid grasper was used to orient the proximal bowel properly and then guide the proximal stapler anvil to mate with the stapler. Once apposed, the stapler was fired. The stapler was then removed, and the anastomotic tissue rings were immediately inspected for completeness by trans-anal endoscopy.
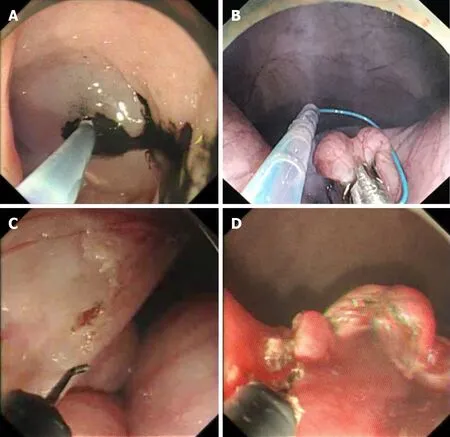
Figure 1 Peroral traction-assisted transanal natural orifice trans-anal endoscopic surgery sigmoidectomy followed by intracorporeal colorectal end-to-end anastomosis under trans-gastric endoscopic guidance. A: The anterior wall of the rectosigmoid colon was tattooed with India ink by submucosal injection; B: An endoloop was placed over the anti-mesenteric side of one colonic segment for traction; C: Dissection of the inferior mesenteric vessels; D: The mobilized rectosigmoid colon was exteriorized and transected trans-anally.
Closure of gastrostomy using endoscopic clips under trans-gastric endoscopic vision: The defect of the gastric tunnel entrance was closed with endoscopic clips.
After the procedure, all three animals were euthanized immediately, abdominal exploration was performed, and the air-under-water leak test was carried out. The pelvis was filled with normal saline, and the rectum was insufflated to confirm whether the anastomosis was airtight.
Euthanasia and outcome measurements
The primary outcome of this study was the procedure success rate. The secondary outcomes were the total operative time, specimen length, completeness of colorectal anastomosis, and adverse event rate in the perioperative period. At necropsy, the anastomosis was tested for leaks using the air-under-water test.
Animal care and use statement
The animal protocol was designed to minimize pain or discomfort to the animals. All animals were euthanized by barbiturate overdose (intravenous injection, 150 mg/kg pentobarbital sodium) for autopsy.
RESULTS
The procedure was completed in all three animals, with the total operation time ranging from 193 min to 259 min (Table 1). Neither intraoperative complications nor hemodynamic instability occurred during the operation. Adequate anatomic exposure around the inferior mesenteric vessels was achieved by peroral external traction using endoloop ligation. Endoscopic dissection of the inferior mesenteric vessels was successful in all cases. The length of the resected specimen ranged from 7 cm to 13 cm,attached by the sigmoid mesentery.

Table 1 Results of the procedure
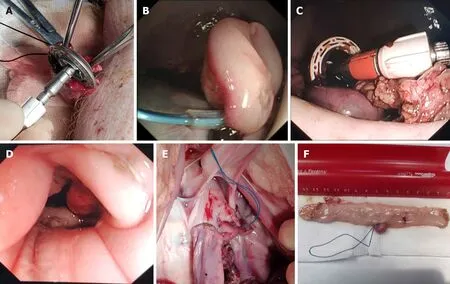
Figure 2 Peroral traction-assisted transanal natural orifice trans-anal endoscopic surgery sigmoidectomy followed by intracorporeal colorectal end-to-end anastomosis under trans-gastric endoscopic guidance. A: A purse-string suture was placed around the top of the open proximal colonic segment after a stapler anvil was inserted; B: An endoloop was used to ligate the lateral rectostomy by endoscopy; C: The anvil was used to approach the stapler with the assistance of a rigid grasper; D: Endoscopic observation of the colorectal anastomotic tissue ring; E: View via laparotomy of the lower abdomen and pelvis showing colorectal end-to-end anastomosis; F: The resected sigmoid colon specimen.
With the assistance of a trans-umbilical rigid grasper, intracorporeal end-to-end colorectal anastomosis was achieved in all three animals. The anastomotic tissue ring in the second case was noted to be incomplete along the posterior rectal wall due to the insufficient occluding purse-string suturing of the proximal colonic segment. This may be a result of excessive resection of the sigmoid colon leading to retraction of the proximal segment, impairing sufficient purse-string suturing. The anastomotic defect was then reinforced with clips by tans-anal endoscopy.
At necropsy, there were no injuries to the adjacent organs. A properly oriented,tension-free colorectal end-to-end anastomosis was achieved in all three animals.Fortunately, the leak test was also negative in all animals regardless of whether anastomotic completeness was achieved.
DISCUSSION
To the best of our knowledge, this is the first study assessing the feasibility and safety of peroral external traction-assisted transanal NOTES sigmoidectomy followed by intracorporeal colorectal end-to-end anastomosis by using only currently available endoscopic flexible accessories except a rigid grasper in a live swine model.
In our study, endoscopic sigmoid mesocolon dissection, major vessel ligation, andretrieval were feasiblethe pure NOTES approach. As Parkstated, “The most important is that the operating field exposure through traction should be performed before dissection itself”. Different from the description of Park, in our study, external traction of the sigmoid mesocolon was achieved through trans-oral introduction of an endoloop knotted to a segment of dental floss. Furthermore, our traction method could be used in the whole colon, while traction through the transanal introduction of a circular stapler was only available for the sigmoid colon.Notably, the direction of traction was fixed both in our study and Park SJ’s study. In the future, gastrointestinal endoscopic robots may enable real-time changes in traction direction by remote control.
The COpneumoperitoneum maintained by an endoscopic insufflator also permitted intra-abdominal visualization. Since it was difficult to monitor the intraabdominal pressure during the procedure, endoscopic discontinuous suction was necessary.
In contrast to extracorporeal colorectal anastomosis published in previous reports, intracorporeal end-to-end anastomosis under trans-gastric endoscopic guidance was introduced in our study to achieve high colorectal anastomosis.According to the updated metaanalysis, compared to extracorporeal anastomosis,intracorporeal anastomosis may be associated with a shorter extraction site incision,faster bowel recovery, fewer perioperative complications, and lower rates of conversion to open surgery, anastomotic leakage, surgical site infection, and incisional hernia. In our study, the most technically challenging and time-consuming step was to mate the proximal stapler anvil with the stapler inserted trans-anally. A transumbilical rigid grasper was used to achieve alignment.
Similar to gastrostomy, lateral rectostomy on the anterior rectal wall was achieved by using directed short submucosal tunneling for subsequent end-to-end anastomotic creation.
To date, gastric closure remains one of the major difficulties, and endoscopic clipping can only achieve mucosal apposition. For secure gastric closure, the creation of gastrostomy by directed submucosal tunneling was applied in this study so that we only needed to close the mucosal defect of the gastric tunnel entrance.
There were also several technical challenges in our study. First, due to the lack of a wide field of vision and the spatial orientation of laparoscopy, accurate endoscopic dissection is still technically demanding. It is difficult to precisely identify the beginning and endpoint of the colon segment to be dissected. Since virtual reality with three-dimensional reconstruction allows an enhanced understanding of crucial anatomical details, it would contribute to improving safety and accuracy in endoscopic surgery. Second, although intracorporeal end-to-end anastomosis was achieved in this study, rigid instrumentation was still needed. Before clinical application of this technique, instrument development, including endoscopic anastomotic equipment,would be required. Third, to determine whether the anastomotic method can achieve histological anastomosis, subsequent survival experiments should be carried out.
CONCLUSION
In conclusion, this novel technique for performing NOTES sigmoidectomy with the assistance of peroral external traction, followed by intracorporeal colorectal end-to-end anastomosis aided by a trans-umbilical rigid grasper, is safe and feasible in a live animal model and is worthy of further improvements.
ARTICLE HIGHLIGHTS
Research background
Since 1991, an increasing number of minimally invasive surgical techniques, including single-incision laparoscopic surgery (SILS), needlescopic surgery (NS), and natural orifice transluminal endoscopic surgery (NOTES), have been developed rapidly. To date, all cases of NOTES colorectal resection have included a hybrid laparoscopic approach with the use of established rigid platforms.
Research motivation
Our research aimed to improve NOTES-related techniques.
Research objectives
Our study aimed to introduce the novel technique of peroral external traction-assisted transanal NOTES sigmoidectomy followed by intracorporeal colorectal end-to-end anastomosis by using only currently available and flexible endoscopic instrumentation in a live swine model.
Research methods
Three female pigs weighing 25-30 kg underwent NOTES rectosigmoid resection. The procedure of trans-anal NOTES rectosigmoidectomy included the following eight steps: (1) The rectosigmoid colon was tattooed with India ink by submucosal injection;(2) Creation of gastrostomy by directed submucosal tunneling; (3) Peroral external traction using endoloop ligation; (4) Creation of rectostomy on the anterior rectal wall by directed 3 cm submucosal tunneling; (5) Peroral external traction-assisted dissection of the left side of the colon; (6) Trans-anal rectosigmoid specimen transection, where an anvil was inserted into the proximal segment after purse-string suturing; (7)Intracorporeal colorectal end-to-end anastomosis using a circular stapler with a single stapling technique; and (8) Closure of gastrostomy using endoscopic clips.
Research results
The procedure was completed in all three animals, with the operation time ranging from 193 min to 259 min. The length of the resected specimen ranged from 7 cm to 13 cm. With the assistance of a trans-umbilical rigid grasper, intracorporeal colorectal,tension-free, end-to-end anastomosis was achieved in the three animals.
Research conclusions
Peroral traction-assisted transanal NOTES rectosigmoidectomy followed by intracorporeal colorectal end-to-end anastomosis is technically feasible and reproducible in an animal model and is worthy of further improvements.
Research perspectives
The techniques of NOTES rectosigmoidectomy need to be improved for clinical application.
杂志排行

World Journal of Gastrointestinal Endoscopy的其它文章
- Anticoagulation and antiplatelet management in gastrointestinal endoscopy: A review of current evidence
- Evaluation of the diagnostic and therapeutic utility of retrograde through-the-scope balloon enteroscopy and single-balloon enteroscopy
- Nonsteroidal anti-inflammatory drug effectivity in preventing post-endoscopic retrograde cholangiopancreatography pancreatitis: A systematic review and meta-analysis
- Endoscopic ultrasound-guided gallbladder drainage in pancreatic cancer and cholangitis: A case report
- Preemptive endoluminal vacuum therapy after pancreaticoduodenectomy: A case report
- Curling ulcer in the setting of severe sunburn: A case report