Nonsteroidal anti-inflammatory drug effectivity in preventing post-endoscopic retrograde cholangiopancreatography pancreatitis: A systematic review and meta-analysis
2021-01-11JuanPabloRomSerranoJosJukemuraSamuelGalanteRomaniniPaFernandoGuamAguilarJulianaSilveiraLimadeCastroIsabelaTrindadeTorresJosAndresSanchezPullaOtavioMicelliNetoEloyTaglieriJosCelsoArdengh
Juan Pablo Román Serrano, José Jukemura, Samuel Galante Romanini, Paúl Fernando Guamán Aguilar,Juliana Silveira Lima de Castro, Isabela Trindade Torres, José Andres Sanchez Pulla, Otavio Micelli Neto, Eloy Taglieri, José Celso Ardengh
Abstract BACKGROUND Endoscopic retrograde cholangiopancreatography (ERCP) is the primary therapeutic procedure for the treatment of diseases affecting the biliary tree and pancreatic duct. Although the therapeutic success rate of ERCP is high, the procedure can cause complications, such as acute pancreatitis [post-ERCP pancreatitis (PEP)], bleeding and perforation.AIM To assess the efficacy of non-steroidal anti-inflammatory drugs (NSAIDs) in preventing PEP during follow-up.METHODS Databases such as MEDLINE, EMBASE and Cochrane Central Library were searched. Only randomized controlled trials (RCTs) comparing the efficacy of NSAIDs and placebo for the prevention of PEP were included. Outcomes evaluated included the incidence of PEP, severity of pancreatitis, route of administration, types, dose, and timing of administration of NSAIDs.RESULTS Twenty-six RCTs were considered eligible with a total of 8143 patients analyzed.Overall, 4020 patients used NSAIDs before ERCP and 4123 did not use NSAIDs(control group). Ultimately, 298 cases of post-ERCP acute pancreatitis were diagnosed in the NSAID group and 484 cases in the placebo group. The risk of PEP was lower in the NSAID group risk difference (RD): -0.04; 95% confidence interval (CI): -0.07 to - 0.03; number needed to treat (NNT), 25; P < 0.05. NSAID use effectively prevented mild pancreatitis compared to placebo use (2.5% vs 4.1%; 95%CI: -0.05 to -0.01; NNT, 33; P < 0.05), but information on moderate PEP and severe PEP could not be fully elucidated. Only rectal administration reduced the incidence of PEP with RD: -0.06; 95%CI: -0.08 to -0.04; NNT, 17; P < 0.05).Furthermore, only the use of diclofenac or indomethacin was effective in preventing PEP, at a dose of 100 mg, which must be administered before performing ERCP.CONCLUSION Rectal administration of diclofenac and indomethacin significantly reduced the risk of developing mild PEP. Additional RCTs are needed to compare the efficacy between NSAID routes of administration in preventing PEP.
Key Words: Pancreatitis; Endoscopic retrograde cholangiopancreatography; Diclofenac;Indomethacin; Rectal
INTRODUCTION
Endoscopic retrograde cholangiopancreatography (ERCP) is a useful tool in the treatment of biliopancreatic duct diseases with high technical and clinical success rates. The most common post-ERCP adverse events (AEs) are acute pancreatitis (AP),bleeding, perforation, and cholangitis[1]. AP is the most common, with an incidence between 3.5% and 9.7% and mortality ranging from 0.1% to 0.7%[2].
Mild AP is defined as the absence of organ failure and/or local and systemic complications, moderate AP as the presence of transient organ failure or local or systemic complications, and severe AP as the presence of persistent organ failure with or without complications. Persistent organ failure has a risk of mortality between 36%and 50% within the first phase[3]. Post-ERCP pancreatitis (PEP) is mild in 4%, moderate in 1.8% to 2.8%, and severe in 0.3% to 0.5%[4,5].
Risk factors associated with PEP are divided into patient- and procedure-related factors. Patient-related factors include sphincter of Oddi dysfunction (SOD), female gender, history of AP, and history of PEP, whereas procedure-related factors include difficult catheterization, passage of a guidewire in the main pancreatic duct (MPD) ≥ 1 time, and pancreatic injection ≥ 1 time[2]. The search for methods to prevent the occurrence of PEP is important to increase patient safety and reduce the incidence rate.
Studies have described preventive measures to avoid the occurrence of PEP, such as the use of nonsteroidal anti-inflammatory drugs (NSAIDs) and pancreatic stent implantation. Theoretically, the use of NSAIDs that inhibit cyclooxygenase 2 (COX-2)improves the acute inflammatory effects of AP and reduces its systemic sequelae[6].NSAIDs that inhibit phospholipase A2 (indomethacin and diclofenac) play a role in the early phase of the inflammatory cascade in AP. Research on the use of NSAIDs to prevent PEP started in the 1980s[7]. Randomized trials in animals have shown that indomethacin has a low mortality rate[7]. Its properties prevent papillary edema, at least theoretically decreasing the occurrence of PEP.
This systematic review and meta-analysis was performed to determine the effectiveness of NSAIDs in preventing PEP. The objective was to analyze the appropriate dose, route, time of administration, and the best NSAIDs to reduce the incidence of PEP.
MATERIALS AND METHODS
Protocol and registration
This systematic review and meta-analysis was carried out in accordance with the recommendations of theCochranemanual, following the items in the preferred reporting items for systematic reviews and meta-analyses (PRISMA)[8]. The review was registered in the International Prospective Register of Systematic Reviews(PROSPERO) database, under registration number 42016049582, and approved by the ethics committee of the Moriah Hospital, São Paulo, Brazil.
Eligibility criteria and search procedure
The eligibility criteria were organized according to the international standards for patient, intervention, comparison, and outcome. “Patient” (P) was those submitted to ERCP, “intervention” (I) was administration of different types of NSAIDs described in the literature, “comparison” (C) was the administration of placebo or other similar drugs to NSAIDs, and “outcome” (O) was the main outcome of PEP. The research was carried out using different databases or virtual libraries, among which were MEDLINE/PubMed, Embase, and central Cochrane library. The dates used were from the beginning of our study in July 2016 to December 2019.
The key words used in the MEDLINE research were ERCP, NSAIDs, pancreatitis,diclofenac, and indomethacin. For other databases, we used simpler terms, such as ERCP, pancreatitis, and NSAID. All types of studies that assessed the reduction in the incidence of PEP were researched. In this systematic review and meta-analysis, we included only randomized clinical trials (RCTs) that studied the incidence of PEP with the use of NSAIDs.
We excluded meta-analyses, prospective nonrandomized, retrospective studies, case series, pancreatic stent studies, NSAIDvsNSAID, drugs that were not in the NSAID group, and abstracts and papers that were requested by the author without response.There was no restriction on the language and date of publication.
We included patients of any gender > 18 years old who underwent ERCP for the first time and with signed informed consent. We excluded those with previous sphincterotomy, periampullary tumor, signs of evident AP, chronic pancreatitis,allergies to NSAIDs, and active and healing gastric and duodenal ulcers.
The main outcome was the reduction in the overall incidence of PEP with the use of NSAIDs. We evaluated the reduction in incidence in relation to the severity of PEP(mild, moderate, and severe), types of NSAIDs (diclofenac, indomethacin, valdecoxib,ketoprofen, naproxen, and celecoxib), different routes of administration [rectal (R),oral (O), intramuscular (IM), and intravenous (IV)], and dose and time of administration (before, during, after, and before/after ERCP).
Evaluation of eligibility criteria and study selection
Two reviewers selected RCTs independently and by group analysis. Any disagreement was resolved by the reviewers and group members after consensus. The study selection process was described in the PRISMA flowchart[8]. This systematic review and meta-analysis was organized in relation to the critical assessment instruments according to the type of design of the JADAD scale[9]. Each study was classified according to the risk of bias, randomization, allocation, blinding, losses,prognostic factors, results, and patient number needed to treat (NNT).
Data analysis
Data were extracted based on the information on treatment intention. For all outcomes, risk difference (RD) was considered for analysis with a 95% confidence interval and statistical significance ofP< 0.05. The difference between the outcomes of the analysis of each subgroup was calculated through RD together with dichotomous variables.
The analysis was performed with the statistical software RevMan 5.3 using the Mantel–Haenszel (MH) test withfixed effect(FE). Heterogeneity was considered by I2,with a cutoff of 50%. When a value ≥ 50% was found, sensitivity analysis was performed to try to identify a study with a higher probability of publication bias(“outlier”), through graphic expression of the “funnel plot” with the model or FE.
The sensitivity study aimed to identify the publication bias that justifies heterogeneity through the Egger funnel plot test. Once the publication biases were identified, which maintained heterogeneity ≥ 50%, it was decided to work with RD and randomized effect (RE) and work or interpret within the present systematic review and meta-analysis with a substantial or true heterogeneity.
RESULTS
Selection of studies
The evaluated articles are presented in the PRISMA flowchart and include 26 RCTs,142 article were excluded (Figure 1). The 26 RCTs selected[6,7,10-33]were considered eligible and included a total of 8143 patients. The intervention group (NSAID)included 4020 patients and the comparison group (control) included 4123 patients(placebo and other substances).
Study characteristics
We organized the studies after the consensus of two independent reviewers and after the group's consensus. Table 1 shows the included studies in alphabetical order, year,country of publication, route of administration, dose, and type of NSAIDs. Of the 26 RCTs, diclofenac was used in 12[10-21], indomethacin in 10[7,22-30], COX-2 inhibitors in 2[6,31], and other NSAIDs in 2[32,33]. Table 2 shows the included studies in alphabetical order, type of substance used (comparison) and number (n), and time of NSAID administration.
Description of articles
In assessing the risk of bias, all articles had adequate randomization, allocation, and blinding. The losses did not reach 20%. The JADAD score was above 3, which was satisfactory for inclusion in all studies. The description of each article is shown in Table 3. The time to diagnosis of PEP described in the RCTs ranged from 24 to 72 h and patients met at least two of Banks’ three diagnostic criteria: History of abdominal pain, nausea, or vomiting, increase in serum amylase, and images compatible with AP.
PEP frequency
The overall incidence of PEP and a forest plot can be seen in Figure 2 and 3. In total there were 298 and 484 episodes of PEP in the intervention (4020) and comparison group (4123), respectively. RD was 95%CI -0.04 (-0.07, -0.03),P< 0.05, and NNT = 25.
PEP severity
Fourteen articles evaluated the incidence rate of mild PEP. A total of 2600 and 2569 patients were allocated to the intervention and comparison groups, respectively. There were 136 and 203 episodes of mild AP in the intervention (2600) and comparison group (2569), respectively. RD was 95%CI 0.03 (-0.05, -0.01),P< 0.05, and NNT = 33.Eleven articles evaluated the incidence of moderate PEP. A total of 2134 and 2150 patients were allocated to the intervention and comparison groups, respectively.Moderate PEP was observed in 54 and 203 patients in the intervention and comparison group, respectively. RD was 95%CI -0.01 (-0.02, 0.00) andP> 0.05. Seven articles reported the incidence of severe PEP. A total of 1740 and 1747 patients were allocated to the intervention and comparison groups, respectively. Severe PEP was observed in 16 and 23 patients in the intervention and comparison group, respectively. RD was 95%CI -0.00 (-0.01, 0.00) andP> 0.05. The forest plot shows the severity of PEP(Figure 4 and 5).
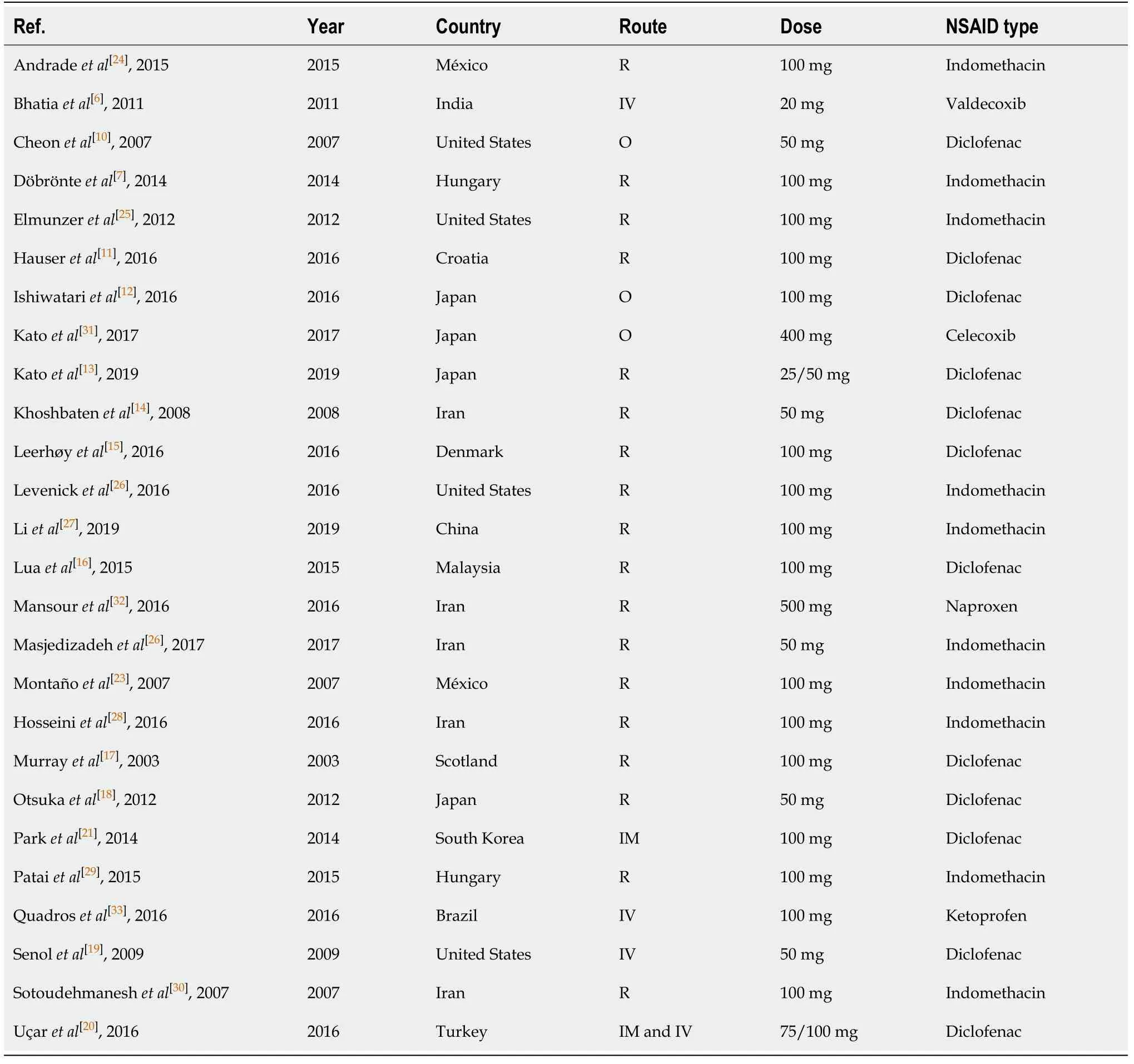
Table 1 Characteristics of the 26 randomized controlled trials, including administration route, dose, and type of non-steroidal antiinflammatory drug
Administration route
Nineteen articles described the rectal route for administering NSAIDs. A total of 3000 and 3017 patients were allocated to the intervention and comparison groups,respectively. PEP was observed in 208 and 388 patients in the intervention and comparison group, respectively. RD was 95%CI -0.06 (-0.08, -0.03),P< 0.05, and NNT= 17. In three articles, the IV route was described and the number of patients allocated to the intervention and comparison groups was 391 and 420 patients, respectively. PEP was observed in 20 and 24 patients in the intervention and comparison group,respectively. RD was 95%CI -0.00 (-0.04, 0.03) andP> 0.05. In three articles, the oral route of administration was described and the number of patients allocated to the intervention and comparison groups was 223 and 401 patients, respectively. PEP was observed in 47 and 49 patients in the intervention and comparison group, respectively.RD was 95%CI -0.00 (-0.05, 0.04) andP> 0.05. In two articles, the IM route was described, with 223 and 195 patients allocated to the intervention and comparison groups, respectively. PEP was observed in 23 and 23 patients in the intervention group and comparison group, respectively. RD was 95%CI -0.03 (-0.13, 0.07) andP> 0.05. The forest plot describes the different routes of administration (Figure 6 and 7).
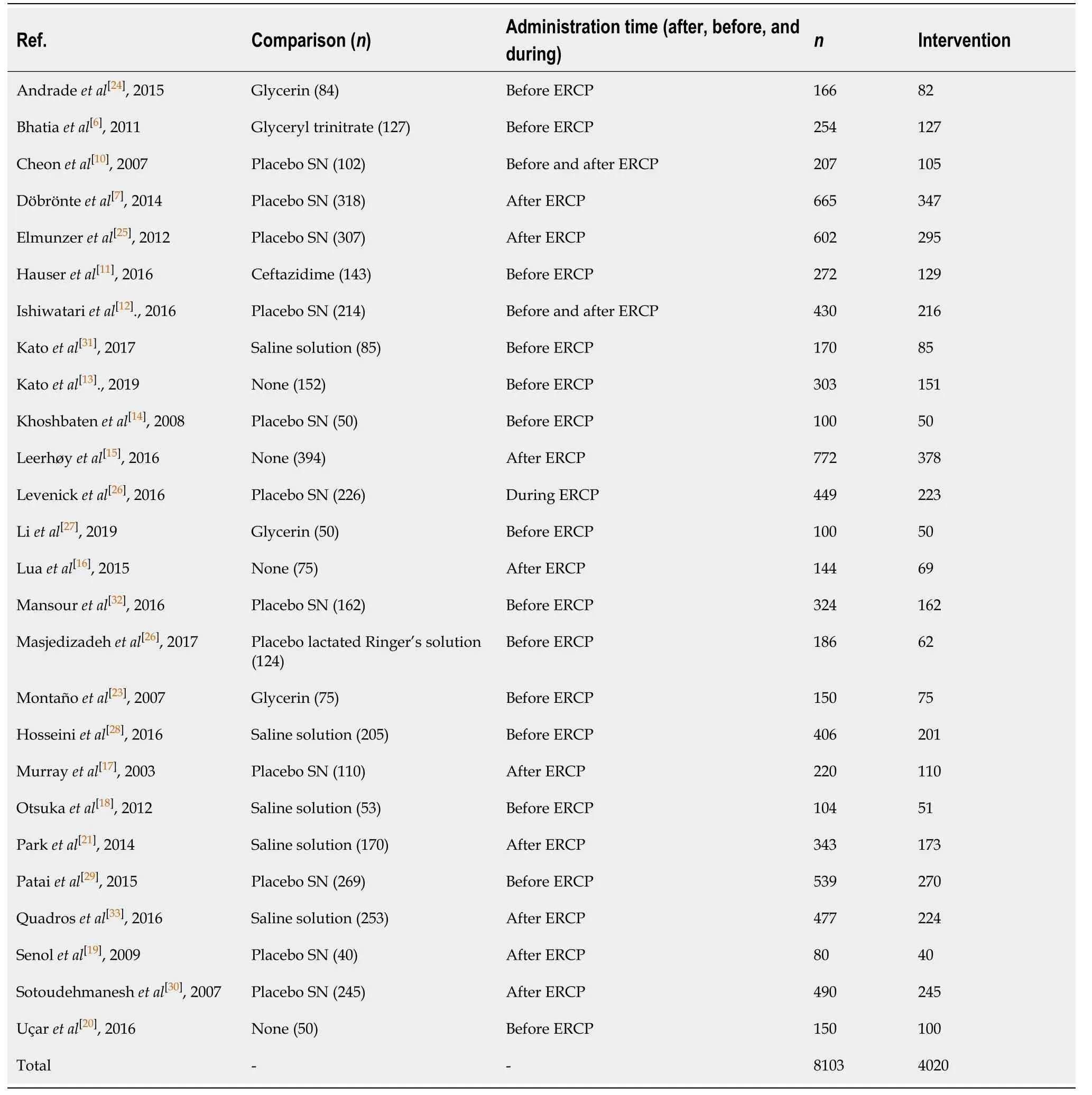
Table 2 Characteristics of 26 randomized controlled trials, including comparison group (number), administration time (before, during,after, and before/after endoscopic retrograde cholangiopancreatography)
Types of NSAIDs
Diclofenac was used to prevent PEP in 15 articles. A total of 1709 and 1792 patients were allocated to the intervention and comparison groups, respectively. In the intervention and comparison group, PEP was observed in 150 and 229 patients,respectively. RD was 95%CI -0.04 (-0.08, -0.01),P< 0.05, and NNT = 25. Indomethacin was described in seven articles. A total of 1713 and 1704 patients were allocated to the intervention and comparison groups, respectively. In the intervention and comparison group, PEP was observed in 109 and 197 patients, respectively. RD was 95%CI -0.06 (-0.09, -0.02),P< 0.05, and NNT = 17. Two articles described the use of COX-2 inhibitors in the prevention of PEP. A total of 212 patients were allocated to the intervention and 212 to the comparison group. In the intervention and comparison groups, PEP was observed in 22 and 25 patients, respectively. RD was 95%CI -0.01 (-0.07, 0.05) andP>0.05. Naproxen (1) and ketoprofen (1) have been described in the prevention of PEP. In the global analysis of both NSAIDs, 386 and 415 patients were allocated to theintervention and comparison group, respectively. In the intervention and comparison groups, 17 and 33 patients had PEP, respectively. RD was 95%CI -0.04 (-0.18, 0.09) andP> 0.05. Figure 8 and 9 shows the forest plot of the incidence of PEP using different types of NSAIDs.
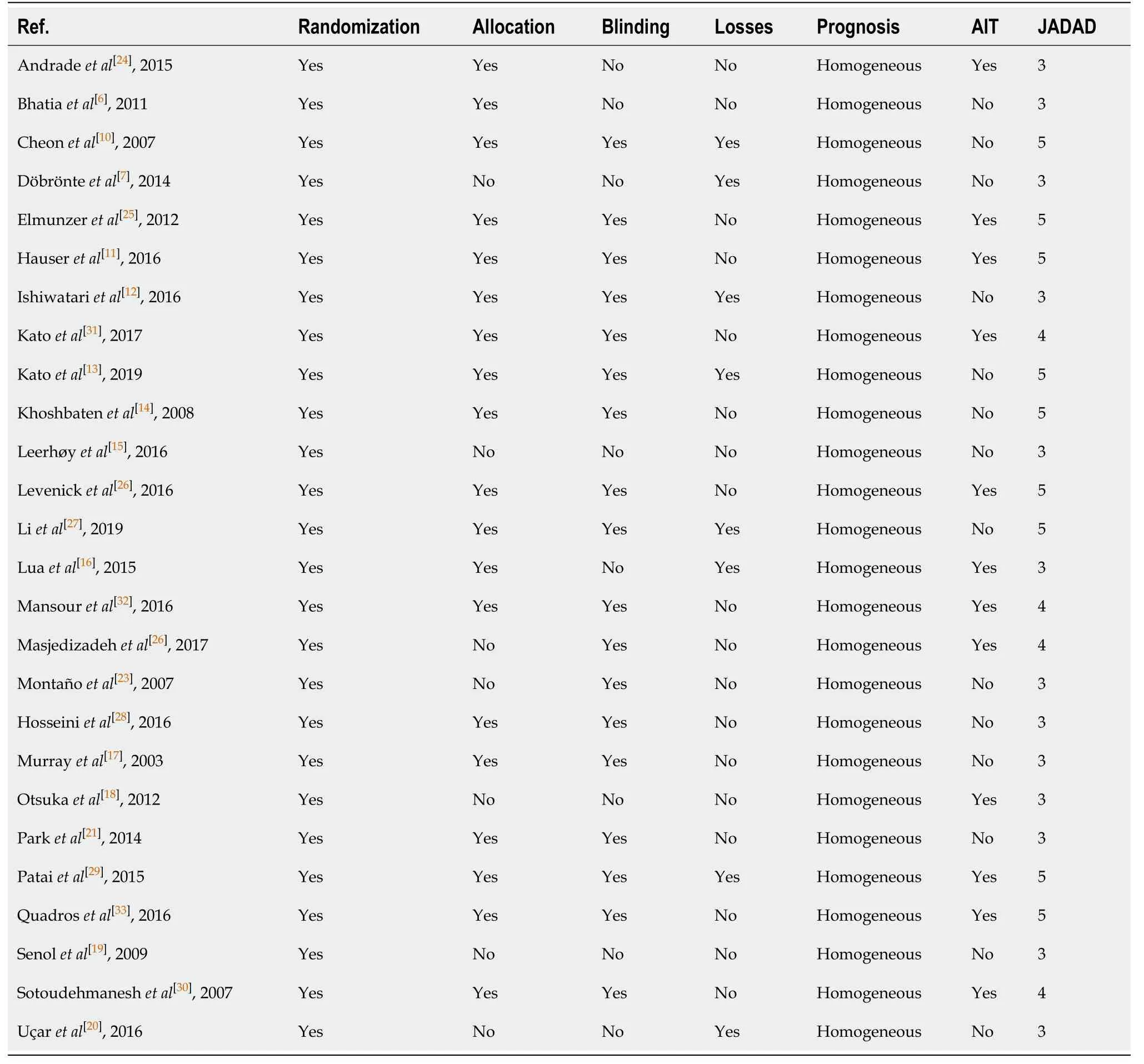
Table 3 Description of 26 randomized controlled trials in relation to allocation, losses, blinding, prognosis, and JADAD
Timing of NSAID administration
Thirteen articles described the use of NSAIDs before ERCP to prevent PEP. A total of 1513 and 1585 patients were allocated to the intervention and comparison groups,respectively. PEP was observed in 115 and 229 patients in the intervention and comparison groups, respectively. RD was 95%CI -0.07 (-0.11, -0.03),P< 0. 05, and NNT= 14.
Ten articles described the use of NSAID after ERCP to prevent PEP. A total of 1963 and 1996 patients were allocated to the intervention and comparison groups,respectively. PEP was observed in 130 and 208 patients in the intervention and comparison groups, respectively. RD was 95%CI -0.04 (-0.07, -0.01),P< 0. 05, and NNT= 25. Two articles described the use of NSAID before and after ERCP to prevent PEP.A total of 321 and 316 patients were allocated to the intervention and comparison groups, respectively. PEP was observed in 37 and 36 patients in the intervention and comparison groups, respectively. RD was 95%CI 0.00 (-0.05, -0.05) andP> 0.05. Only one article described the use of NSAIDs during ERCP to prevent PEP. A total of 223 and 226 patients were allocated to the intervention and comparison groups,respectively. PEP was observed in 16 and 11 patients in the intervention and comparison groups, respectively. In this work, detailed statistical analysis was not possible. The forest plot in Figure 10 and 11 shows the incidence of PEP in relation to the timing of NSAID administration.
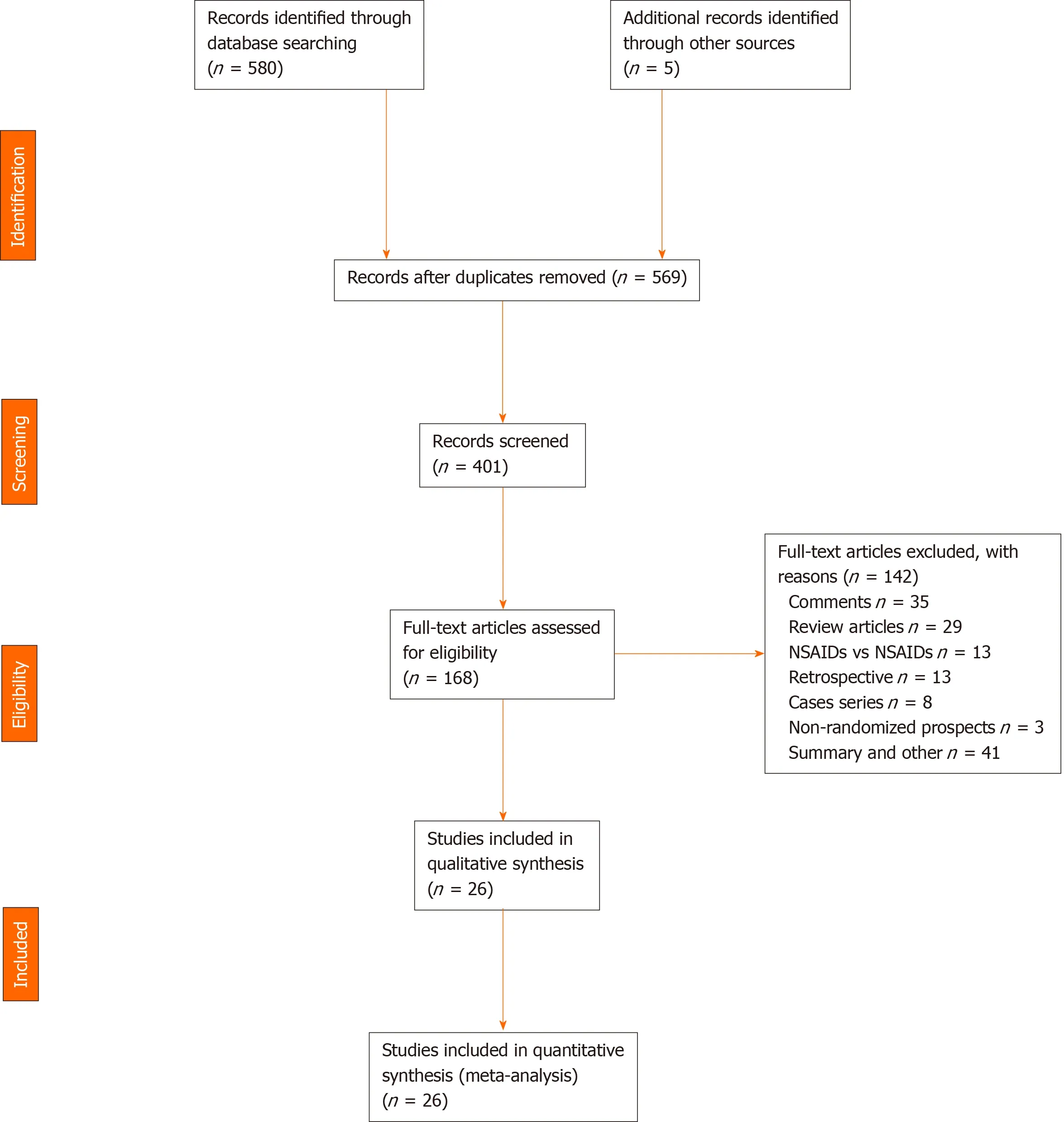
Figure 1 Inclusion of 26 randomized controlled trials in the PRISMA flowchart. NSAIDs: Non-steroidal anti-inflammatory drugs.
DISCUSSION
The use of NSAIDs and their impact on the prevention of PEP has been described in numerous RCTs. Although the number of RCTs is small and no convincing results have been presented, the major international societies of endoscopy and gastroenterology recommend its use in daily clinical practice, but make it clear that it is up to the endoscopist to decide whether or not to use it.
The European Society of Gastrointestinal Endoscopy (ESGE) recommends the use of diclofenac or indomethacin at a dose of 100 mg before ERCP in all patients whether they are at high, medium, or low risk for PEP and when there are no contraindications[2]. Japan Gastroenterological Endoscopy Society advocates a similar policy for the intrarectal administration of NSAIDs in all cases of ERCP when there are no contraindications[34]. The American Society for Gastrointestinal Endoscopy[35]recommends the administration of indomethacin in medium- and high-risk patients.
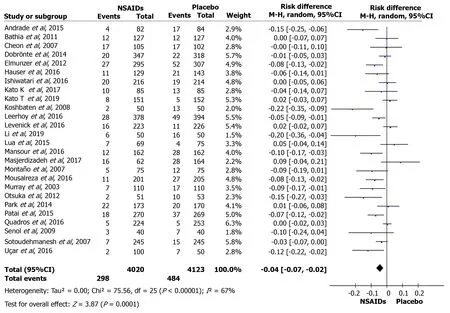
Figure 2 Forest plot of the global incidence of post-endoscopic retrograde cholangiopancreatography pancreatitis. NSAIDs: Non-steroidal anti-inflammatory drugs; CI: Confidence interval.
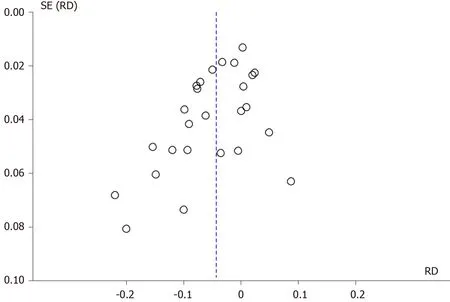
Figure 3 Funnel plot of the global incidence of post-endoscopic retrograde cholangiopancreatography pancreatitis. SE: Standard error; RD:Risk difference.
The Brazilian Society of Digestive Endoscopy does not define an effective method to prevent PEP. In Brazil, there are books dedicated to the subject that recommend the use of indomethacin as a method of preventing PEP[36]. A systematic Brazilian review showed a statistical significance with the use of indomethacin and diclofenac after analyzing 21 studies[37].
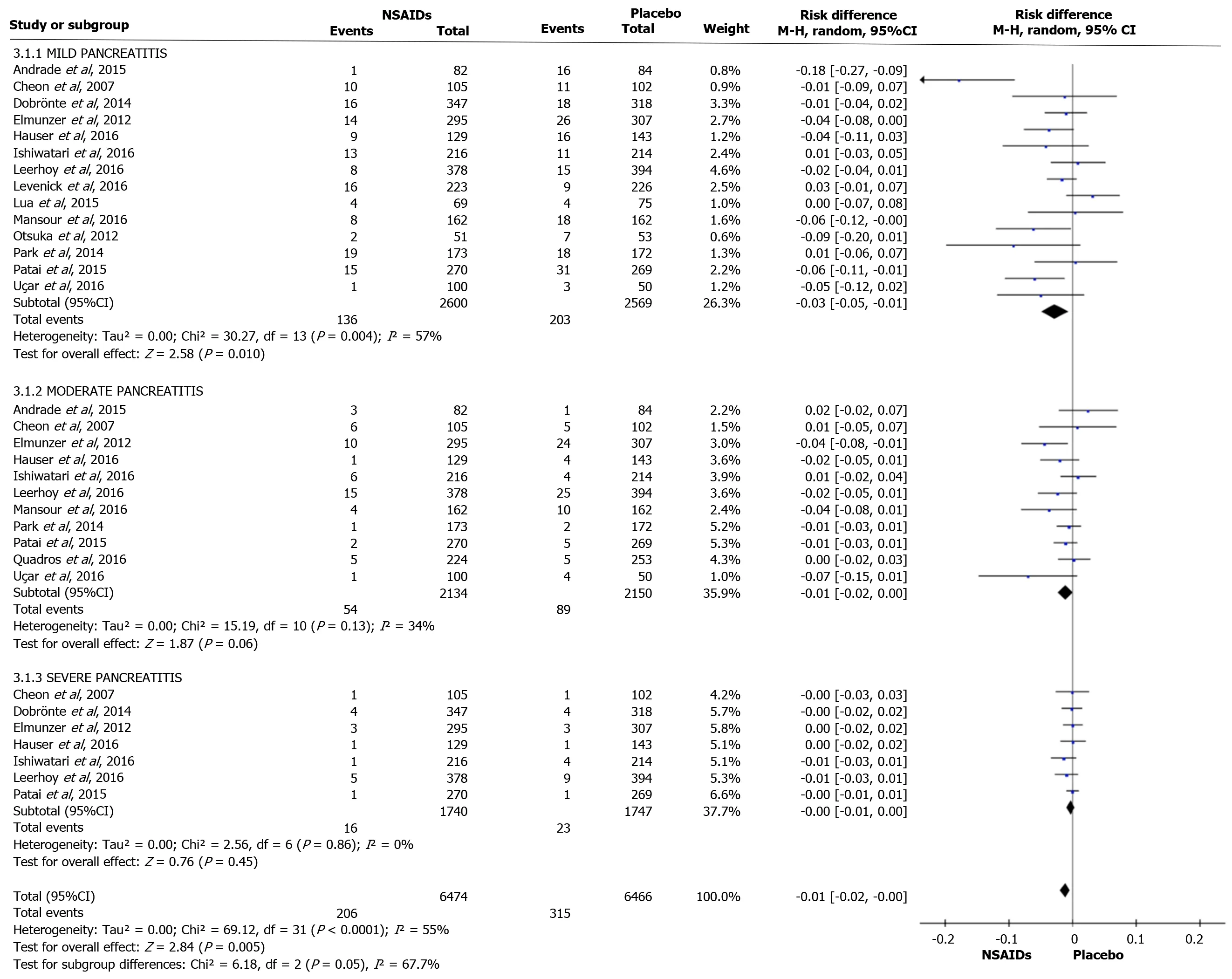
Figure 4 Forest plot of the incidence according to post-endoscopic retrograde cholangiopancreatography pancreatitis severity. NSAIDs:Non-steroidal anti-inflammatory drugs; CI: Confidence interval.
Unlike systematic reviews already published on NSAID use to reduce the risk of PEP, the current study included only RCTs, with a more robust methodology, in which an analysis was carried out in relation to the prevention of PEP and its incidence. This analysis according to the severity of AP episode, type of NSAID, dose, and time and route of administration showed a more detailed perception of important details, which contributed to a more robust conclusion.
The analysis of 26 RCTs showed a significant reduction in the risk of PEP with the use of NSAIDs in both high and low risk patients. However, this study revealed that AEs prevented by the use of NSAIDs mainly involved mild AP. This study showed the efficacy of rectal indomethacin (100 mg) or diclofenac (100 mg) before ERCP, with statistical significance and lower NNT compared to post-ERCP administration.
Due to the small number of RCTs published in the literature, it was not possible to identify whether another route of administration (oral, IV, and IM), another type of NSAID, another time of administration, and doses lower or greater than 100 mg are effective in preventing PEP. Thus, further large multicenter RCTs comparing other NSAIDs, other routes, and times and doses of administration are required to obtain robust conclusions. However, decisions on NSAIDs may be influenced by cost, as indomethacin is more expensive than diclofenac. A cost comparison of the types of NSAIDs to decrease the incidence of PEP should be conducted, in order to obtain more data on this issue. To our knowledge, this is the first meta-analysis on the prevention of PEP using NSAIDs, which includes all types of NSAIDs described in the literature,such as diclofenac, indomethacin, naproxen, valdecoxib, celecoxib, and ketoprofen.
She loosened little Gerda’s dress, and took off the fur boots and the mittens2, or Gerda would have been unable to bear the heat; and then she placed a piece of ice on the reindeer’s head, and read what was written on the dried fish
COX-2 inhibitors, regardless of the initial trigger (the injured pancreatic acinar cell),quickly lead to a pro-inflammatory cascade with a short therapeutic intervention window for some types of interventions. COX enzymes play an important proinflammatory role in AP. The isoform of COX-2 is overexpressed in AP, while the expression of COX-1 remains constant. Pharmacological inhibition of COX-2 improves the severity of the acute effects on AP and its systemic and ischemic sequelae. COX-2 inhibitors may show some benefit in AP[6].
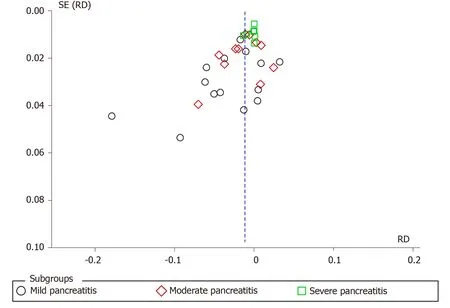
Figure 5 Funnel plot of the incidence according to post-endoscopic retrograde cholangiopancreatography pancreatitis severity. SE:Standard error; RD: Risk difference.
Diclofenac and indomethacin, by inhibiting phospholipase A2, play a role in the early phase of the inflammatory cascade in AP. Phospholipase A2 inhibition results in the suppression of several important classes of pro-inflammatory lipids(prostaglandins, leukotrienes, and platelet-activating factor). NSAIDs further inhibit neutrophil-endothelial cell binding. Of the NSAIDs studied in animals, indomethacin showed a lower mortality rate[7]. However, the effectiveness of other NSAIDs should be investigated.
It is important to emphasize that the results of this meta-analysis may have been influenced by heterogeneity > 50%, in relation to the weight of each RCT included in this study. When we refer to the weight of each study, we refer to the number of patients in each of them which was observed within the forest plot with a minimum weight of 1.5%[26]and a maximum weight of 6.3%[34]. These weights influence the time interpreted in the RevMan 5.3 software.
As mentioned by the ESGE, different demographic factors influence the development of PEP, such as patients with suspected SOD, females, previous AP,previous PEP, difficult cannulation, guidewire passage and MPD contrast, children,fine bile duct, absence of chronic pancreatitis, normal serum bilirubin, end-stage renal disease, previous sphincterotomy, pancreatic sphincterotomy, balloon sphincteroplasty, and failure to remove bile duct stones[38]. For these reasons, PEP prevention is important to increase patient safety.
This study emphasized how each RCT reached the diagnosis of AP, with each of the authors defining an episode of AP as the presence of abdominal pain 24 to 72 h after ERCP, increased pancreatic enzymes, and an image compatible with inflammatory alteration of the pancreatic gland (6.8, 11-34). The recent ESGE guideline suggests testing serum amylase and/or lipase 2 to 6 h after ERCP in patients with post-ERCP abdominal pain who should be discharged on the same day of ERCP. Patients with serum amylase and lipase values below 1.5 to 4 times the normal limit can be discharged without concern for PEP development[2]. Another limitation of the study was that not all RCTs stratified the severity of AP in order to be able to adequately interpret at what level of severity the use of NSAIDs may be most beneficial.
Of the 26 RCTs, 521 episodes of AP were assessed for severity. In 339, the AP episode was mild, representing 65% of stratified patients (339/521). Thus, our results demonstrated that the use of NSAIDs prevents the development of mild PEP. Finally,this systematic review focused solely and exclusively on PEP and its severity, but it is important to note that other AEs can occur post-ERCP which were not included in this review.
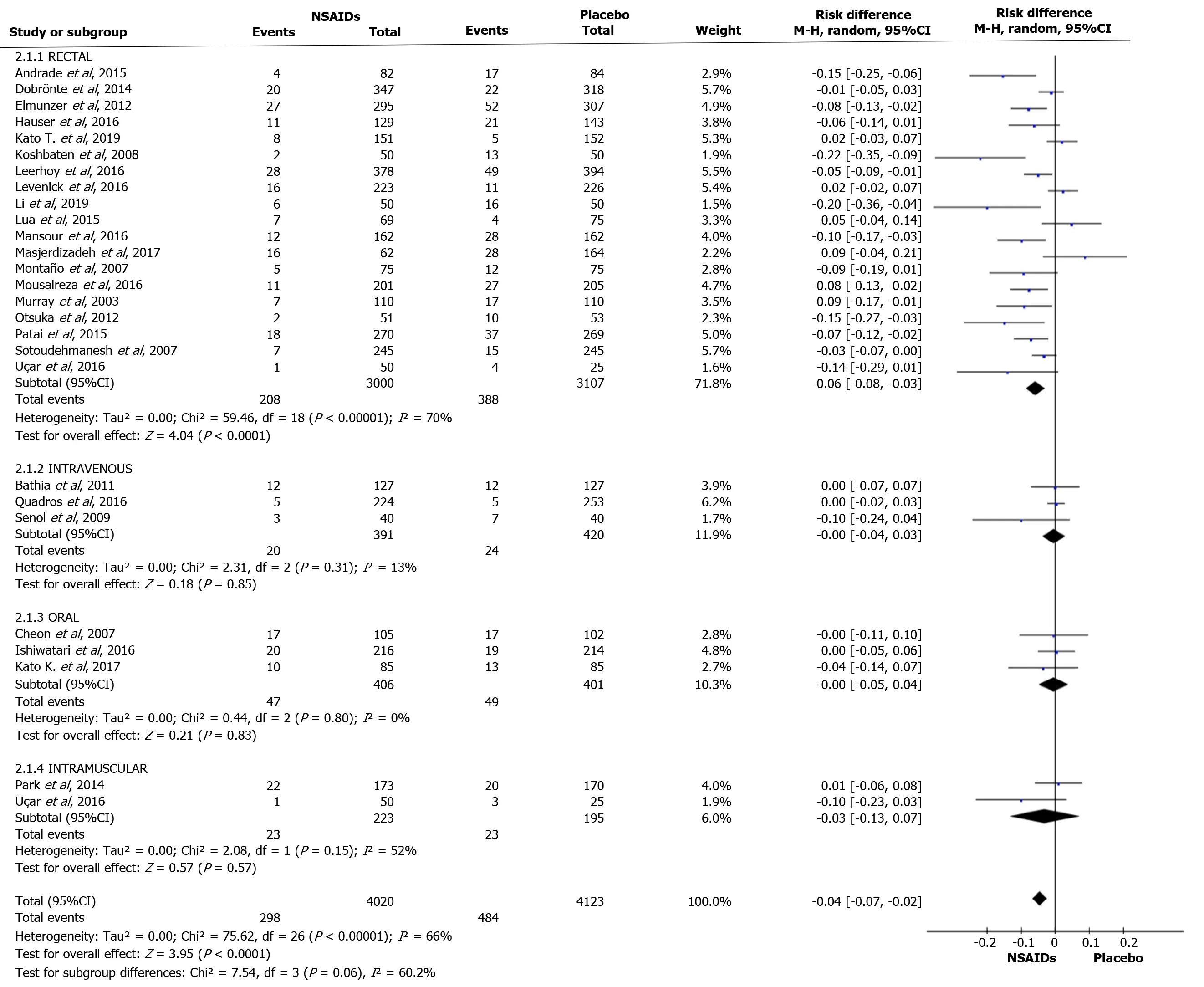
Figure 6 Forest plot of the incidence of post-endoscopic retrograde cholangiopancreatography pancreatitis according to different routes of administration. NSAIDs: Non-steroidal anti-inflammatory drugs; CI: Confidence interval.
Thus, in relation to the subgroups examined, the rectal route adequately reduced the incidence of PEP. The use of NSAIDs was shown to be better in mild AP episodes.Both diclofenac and indomethacin were effective in preventing PEP. The best time to administer NSAIDs is before ERCP and the most appropriate dose that achieved the best results was 100 mg.
Other RCTs are needed to resolve some remaining doubts, such as: Would other NSAIDs be more effective? Would the IV route be better? Could smaller doses of more potent NSAIDs be more effective in preventing PEP?
CONCLUSION
It is concluded that rectal administration of 100 mg diclofenac or 100 mg indomethacin before ERCP prevents the occurrence of mild episodes of PEP.
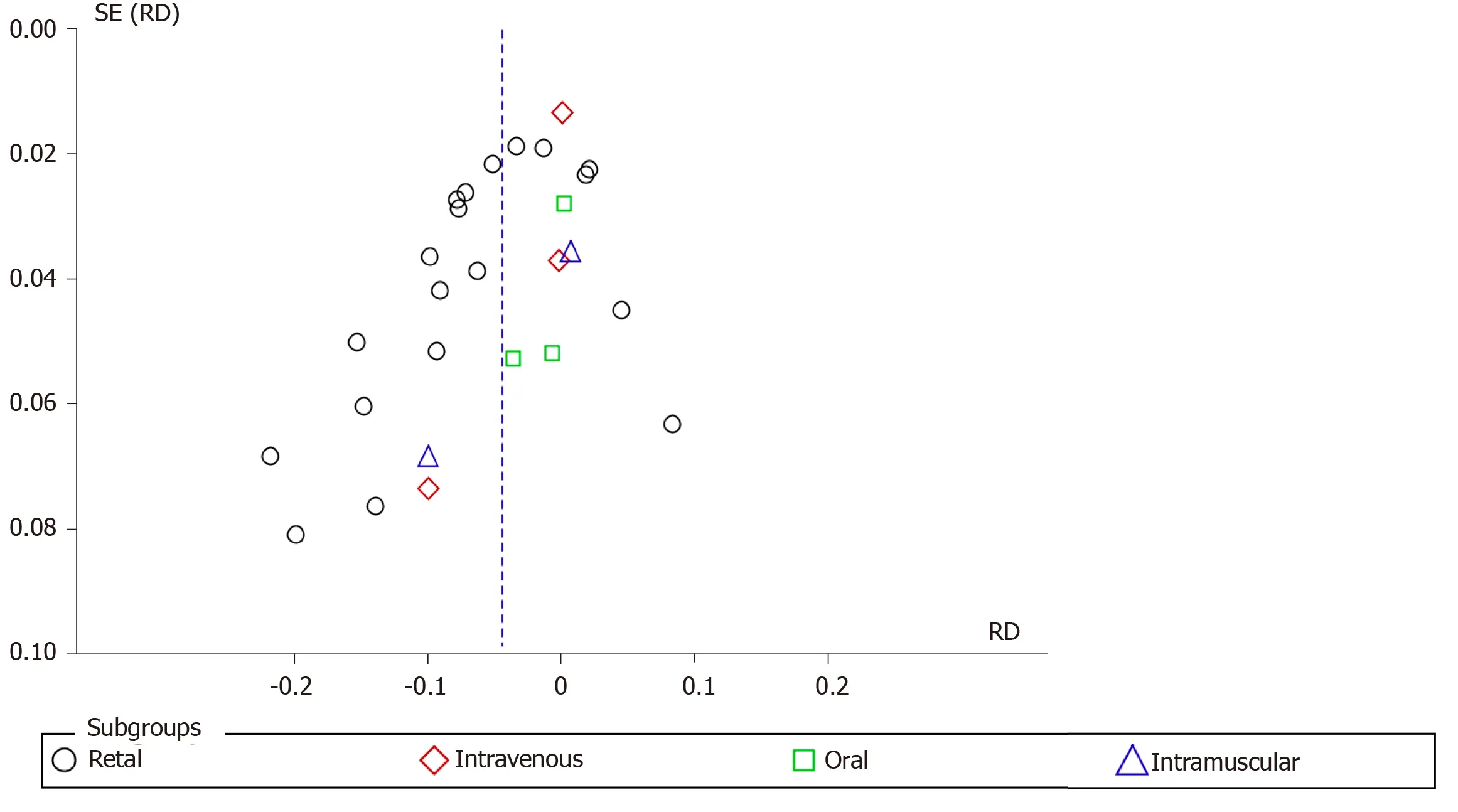
Figure 7 Funnel plot of the incidence of post-endoscopic retrograde cholangiopancreatography pancreatitis according to different routes of administration. SE: Standard error; RD: Risk difference.
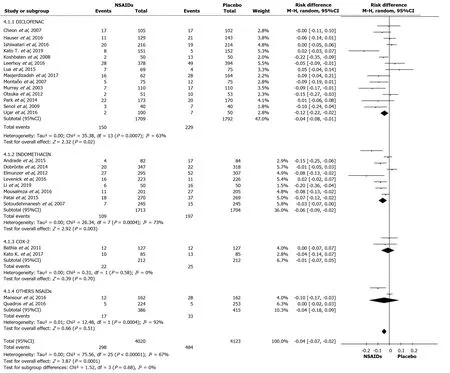
Figure 8 Forest plot showing the incidence of post-endoscopic retrograde cholangiopancreatography pancreatitis with different types of non-steroidal anti-inflammatory drugs. NSAIDs: Non-steroidal anti-inflammatory drugs; CI: Confidence interval.
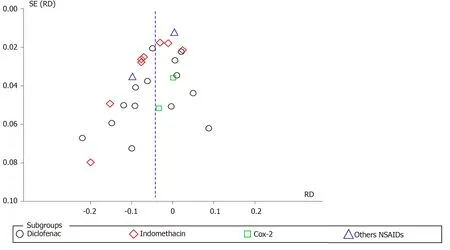
Figure 9 Funnel plot showing the incidence of post-endoscopic retrograde cholangiopancreatography pancreatitis with different types of non-steroidal anti-inflammatory drugs. SE: Standard error; RD: Risk difference; NSAIDs: Non-steroidal anti-inflammatory drugs.
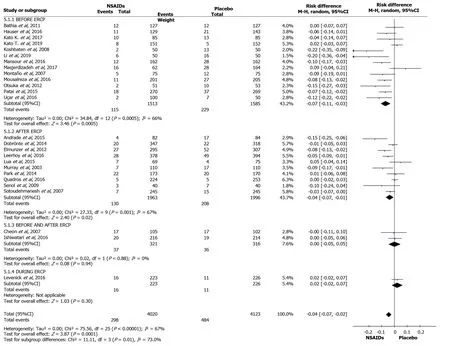
Figure 10 Forest plot showing the incidence of post-endoscopic retrograde cholangiopancreatography pancreatitis in relation to the timing of non-steroidal anti-inflammatory drug administration. NSAIDs: Non-steroidal anti-inflammatory drugs; CI: Confidence interval.
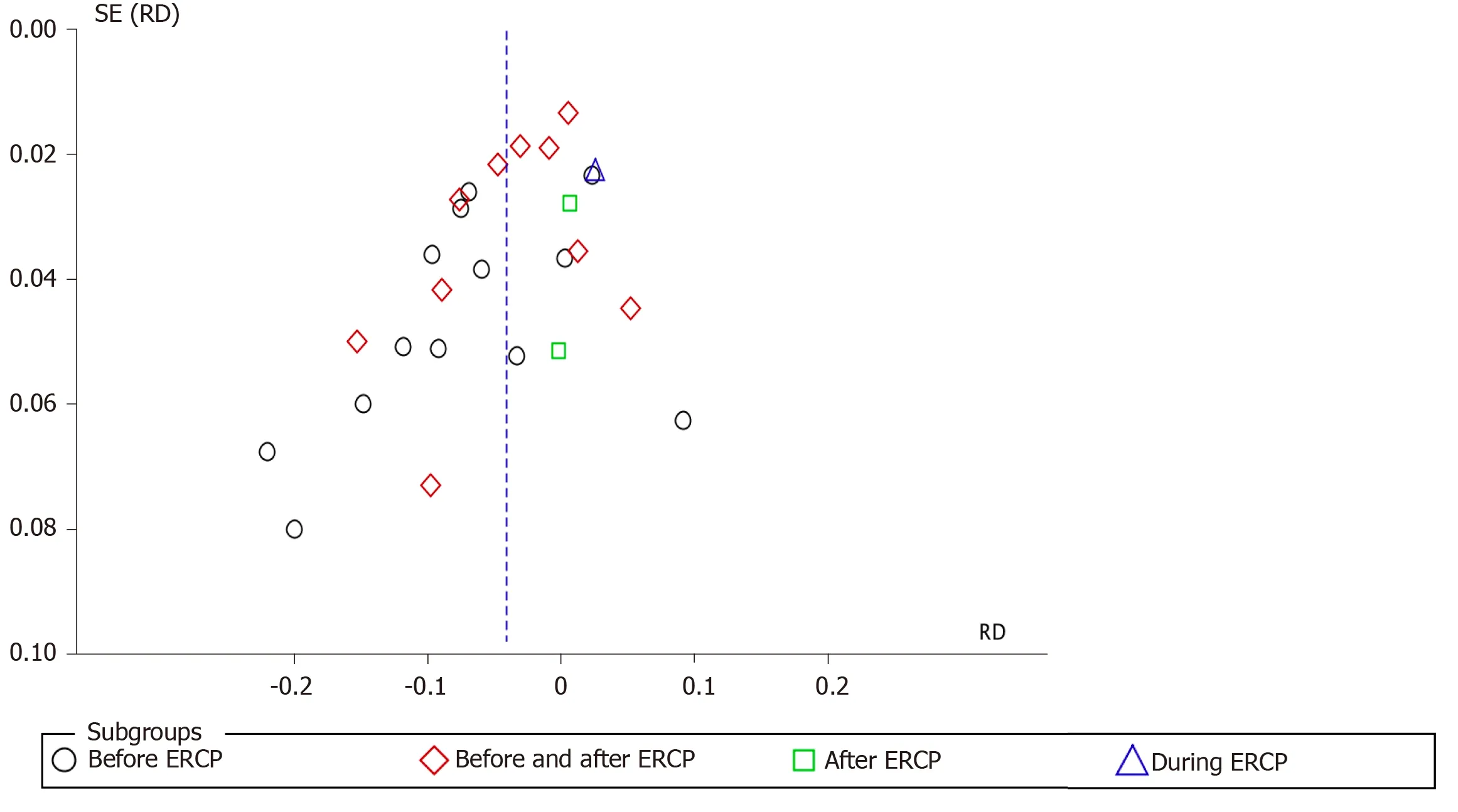
Figure 11 Funnel plot showing the incidence of post-endoscopic retrograde cholangiopancreatography pancreatitis in relation to the timing of non-steroidal anti-inflammatory drug administration. SE: Standard error; RD: Risk difference; ERCP: Endoscopic retrograde cholangiopancreatography.
ARTICLE HIGHLIGHTS
Research background
Endoscopic retrograde cholangiopancreatography (ERCP) is one of the most widely performed therapeutic procedures for bile duct access. However, important complications can occur such as: Post-ERCP pancreatitis (PEP), bleeding, puncture and cholangitis. PEP is considered the main complication after the procedure. Large societies such as ASGE, European Society of Gastrointestinal Endoscopy and Japan Gastroenterological Endoscopy Society describe it as a very important complication and methods must be used to prevent and reduce this pathology. Various methods such as using non-steroidal anti-inflammatory drugs (NSAIDs), prostheses,somatostatin and others have been used, but NSAIDs showed a higher rate of effectiveness.
Research motivation
In many studies, NSAIDs have demonstrated good results, but there are also conflicting results. As there is still controversy as to whether the use of NSAIDs would help in reducing PEP, our group carried out the present study including all the randomized controlled trials (RCTs) described in the literature and the results showed that NSAIDs can help in the prevention of PEP.
Research objectives
Our main objective was to determine the effectiveness of NSAIDs vs “Placebo” as a method of choice or first-line therapy to reduce PEP, using the most recent RCTs. All NSAIDs mentioned in the literature, their route of administration and when they should be administered were investigated. In addition, we hope that this research will have important implications within the medical community.
Research methods
We performed this meta-analysis according to the PRISMA guidelines. Virtual databases were searched up to December 2019 to identify RCTs without date or language restrictions. Following selection of the studies, they were organized according to the PICO criteria and the design followed the JADAD scale. Statistical analysis of the data was performed using RevMan 5.3 software. The main endpoint evaluated in this study was the reduction in the incidence of PEP. Subgroup analyses were also performed and included the severity of pancreatitis, route of administration,time of administration and the types of NSAIDs administered. The results were evaluated with the Higgins test method, using a risk difference with a random effect with a significance ofP< 0.05, 95% confidence interval (CI) and interpreted as true heterogeneity.
Research results
Twenty-six high quality RCTs examining the use of NSAIDsvsPlacebo for the reduction of PEP were included, involving a total of 8143 patients. 4020 patients used NSAIDs before ERCP and 4123 did not use NSAIDs (control group). A total of 298 cases of acute pancreatitis after ERCP were diagnosed in the NSAID group and 484 cases in the placebo group. The risk of PEP was lower (risk difference (RD)) in the NSAID group: -0.04; 95%CI: -0.07 to -0.02; number needed to treat (NNT), 25;P< 0.05.The use of NSAIDs effectively prevented mild pancreatitis compared to the use of placebo (2.5%vs4.1%; 95%CI: -0.05 to -0.01; NNT, 33;P< 0.05), but data on moderate and severe PEP could not be fully elucidated. Only rectal administration reduced the incidence of PEP with the RD: -0.06 95%CI, -0.08 to -0.04; NNT, 17;P< 0.05.
Research conclusions
In conclusion, the use of NSAIDs does reduce the incidence of PEP. In particular,NSAIDs reduce the incidence of mild acute pancreatitis. The most effective drugs were diclofenac and indomethacin. The best route of administration was rectal and the best time for NSAIDs administration was before ERCP.
Research perspectives
It is hoped that these findings will help clinicians decide on the best treatment to prevent PEP.
杂志排行

World Journal of Gastrointestinal Endoscopy的其它文章
- Anticoagulation and antiplatelet management in gastrointestinal endoscopy: A review of current evidence
- Peroral traction-assisted natural orifice trans-anal flexible endoscopic rectosigmoidectomy followed by intracorporeal colorectal anastomosis in a live porcine model
- Evaluation of the diagnostic and therapeutic utility of retrograde through-the-scope balloon enteroscopy and single-balloon enteroscopy
- Endoscopic ultrasound-guided gallbladder drainage in pancreatic cancer and cholangitis: A case report
- Preemptive endoluminal vacuum therapy after pancreaticoduodenectomy: A case report
- Curling ulcer in the setting of severe sunburn: A case report