Tέchne:面向新冠肺炎的多学科应答
——来自非洲和欧洲的案例
2020-12-26米歇尔迪马尔科瓦莱丽娅费德里吉卢卡丰塔纳MicheleDiMarcoValeriaFederighiLucaFontana
米歇尔·迪马尔科,瓦莱丽娅·费德里吉,卢卡·丰塔纳/Michele Di Marco, Valeria Federighi, Luca Fontana
作者单位:米歇尔·迪马尔科,Tέchne,世界卫生组织 瓦莱丽娅·费德里吉,都灵理工大学 卢卡·丰塔纳,世界卫生组织
新冠肺炎治疗中心正迅速成为一种新的建筑设计类型。它诞生于应急时刻,又随着每个新的设计项目而变得更加高效——每个项目都试图最大化流线系统和技术系统在抑制病毒传播上的潜能。在这场疫情爆发逾10 个月之后,很显然,当某个社会的整体医疗体系越脆弱,它所受疫情的影响也越严重。因此,多种设计策略正在全球不同环境进行测试;它们作为新的健康医疗设施概念,在多个层面确立了标准:设计与建造速度、室内空气流通的组织、通风系统与流线系统的创新性整合。2020 年3 月,各类国际组织逐步意识到全球正经历着前所未有的危机,而国家卫生系统——无论国家富有与否——都对于即将到来的挑战措手不及,世界卫生组织为此成立了“医疗技术科学网络”(Tέchne):一个为支持其成员国建设医疗设施等特殊任务的实操性机构。
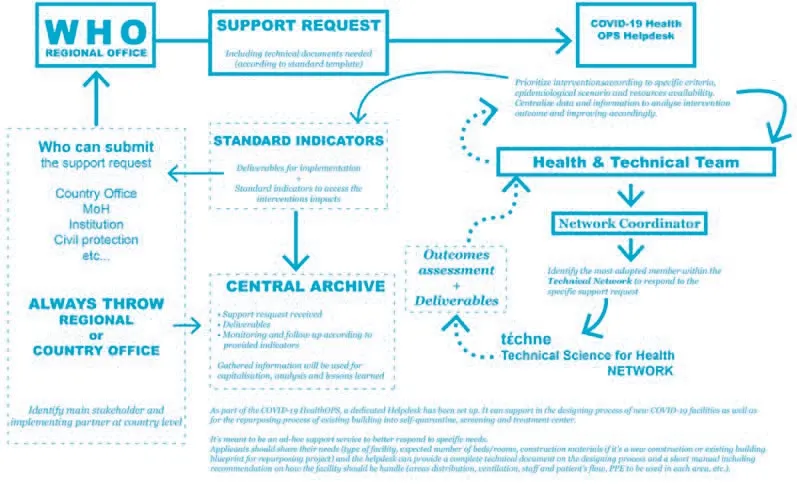
成立Tέchne 是世卫组织应对新冠肺炎疫情所采取的诸多措施之一,更准确地说是为了回应快速建造医疗设施的广泛需求,以此收治感染的及传染性的病人,同时减小医护人员及其他就诊人员的内部感染风险。作为一个多学科合作平台,Tέchne为各类设计提供远程指导:包括修建新冠肺炎医疗设施,将现存建筑改用为隔离、检测及诊疗中心,以及新冠疫情常态化阶段的现存医疗设施改造——让医疗设施变得更具韧性、更为灵活,从而在应急时刻发挥作用。
在过去的5 个月里,Tέchne 逐步成为一个联合了世卫组织各部门以及全球多所专业科研机构的合作网络。Tέchne 的成员包括国际知名的大学和科研院所,支持世卫组织履行职责并实现当下目标。在这些不断加入的学术机构支持下,Tέchne 利用自身的技术优势及特长,为各个向世卫组织地方办公室申请援助的国家机构提供支持。

1 Tέchne的新冠疫情支持/COVID-19 Tέchne support
2 Tέchne的新冠疫情工作模型/COVID-19 Tέchne model of work
Tέchne 的核心优势是其多学科协同路径,这依托于世卫组织内部的专业技能,及其来自建筑、工程、医学等国际学术机构的成员带来的技术能力及科学方法。尽管该组织的创建初衷是应对新冠肺炎疫情相关的特定需求,但如今这个不断壮大的跨学科团体不仅能应对疫情,还能够预防和最小化复杂紧急事件和自然灾害造成的健康后果。
Tέchne 背后的创新理念是,医疗设施的实体空间——它的设计及配置——能够确保它发挥正确作用,开展恰当的医护工作,提升社区的支持能力,减小病人和医护工作者的交叉感染风险。同时,空间方面的知识尚未完善:一条结合设计、防疫措施、流行病学知识的多学科路径也是必须的。
具体来说,Tέchne 的核心目标是:
(1)根据世卫组织的最新指导标准,为医疗设施及传染病治疗设施的建设提供结构及技术设计图纸;
(2)针对世卫组织收到的特定求助,协助制定技术报告和指导意见;
(3)通过分析与特定设施的结构相关的潜在危险因素,协助设施的资本化过程;
(4)研究能够快速建造传染病治疗中心的技术应用;
(5)建立相关教育项目,培训紧急医疗设施的设计以及突发性疫情响应的管理工作。
Tέchne 为应对迥异的环境及特定需求,已发展出非常多样的结构类型,经过7 个多月的探索,包括了传统结构(16 个项目请求)、帐篷结构(8个项目请求)、预制结构或集装箱(10 个项目请求)。通过这些项目,Tέchne 的设计帮助在南美、非洲、欧洲和澳洲各地建造了1900 个救治新冠肺炎病人的床位(图1)。
我们的技术支持被送往世卫组织国家会员、卫生部及其他部门、联合国各部门、国际及国家组织、医疗管理者,他们通过所在地的世卫组织地区办公室,与Tέchne 进行沟通。
一种创新工作模式:4个案例
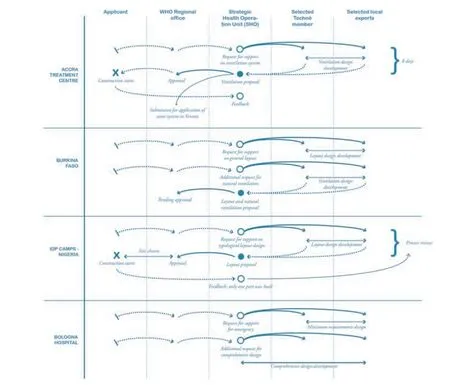
借助Tέchne 的多学科技术支持,世卫组织得以在8 天内就为申请者提供一套完整响应方案,包括相应的技术图纸和示意图,来新建或将现有设施改造为能够满足新冠肺炎救治最低要求的医疗中心(图2、3)。
图2 展现了不同工作阶段的理想工作流程:世卫组织的战略卫生行动组(SHO)是世卫组织地区办公室、申请援助的地方相关者以及Tέchne 的技术支持网络之间复杂沟通过程的支点。图3 则追溯了设计过程中各相关方之间的沟通流程,包括从行动开始到最终落成过程中的讨论和更新。在各个案例中,首先是由申请者向世卫组织地区办公室发出
COVID-19 treatment centres are rapidly becoming a new design typology, born in a time of emergency and becoming more effective as each new design attempts to maximise the potential of distributive systems as well as technical systems in containing the spread of the disease. After more than ten months from the onset of the pandemic, it is clear that the more vulnerable the healthcare system is, the harder the impact of the pandemic is on the society as a whole. Therefore, a number of design solutions are being tested in different contexts around the world and, as new healthcare facility concepts, have set the bar in different respects: velocity of design+construction, organisation of internal flows, innovative combination of ventilation and distributive systems. In March 2020, as international institutions of varying nature were grappling with the realisation that the world was undergoing an unprecedented crisis, and that national health systems – in wealthy and less-wealthy countries alike – were unprepared for what was about to come, the World Health Organisation (WHO) established Tέchne, an operative branch to support its members in the specific task of readying their healthcare facilities.
Tέchne is part of the response of WHO to the COVID-19 pandemic and more precisely to the widespread need to rapidly set up health facilities that are able to hospitalise infected and infectious patients while reducing the risk of nosocomial infections amongst healthcare workers and other patients seeking care. As interdisciplinary platform, Tέchne provides remote support for the design process of new COVID-19 facilities, repurposing existing building into self-quarantine, screening and treatment centres as well as reshaping existing healthcare facilities for the COVID-19 post-acute phase in order to make health structures more resilient and flexible therefore able to easily surge in case of need.
In the course of almost five months, Tέchne has incrementally shaped as a network of WHO departments together with several technical universities and institutions around the world. Tέchne members are internationally recognised universities and institutions that support WHO in implementing its mandated work and achieving its current goal. As we write, Tέchne is composed of universities and technical institutions that, as part of a growing network, make their technical knowhow and competencies available for institutions of various nationalities applying for support to WHO regional offices.
T h e c o r e s t r e n g t h o f T έ c h n e i s i t s multidisciplinary approach, which relies on the internal knowhow of WHO as well as the technical competencies and scientific approach brought by Tέchne's members, which include international Architecture, Engineering and Medical universities and institutions. W hile the network was conceived to meet specific needs connected to the COVID-19 pandemic, it is now developing into a multidisciplinary group able to respond not only to epidemics, but also to prevent and minimise the health consequences of complex emergencies and natural hazards.
The innovative idea behind Tέchne is that the physical space of a healthcare facility, its design and its configuration, are essential to assure a correct functioning, allowing proper medical care, enhancing community support and reducing the risk of nosocomial infections for patients and healthcare workers. At the same time, spatial knowledge is not sufficient: a multidisciplinary approach, combining design, infection prevention and control understanding and an epidemiological overview of the disease, is likewise necessary.
Specifically, Tέchne core objectives are:
(a) Supporting WHO in developing structural and technical drawing for healthcare structures and infectious disease treatment facilities according to latest WHO guidance;
(b) Contributing to technical report and guidance for specific ad-hoc support requests received by WHO;
(c) Contributing in the capitalisation process through analysis of potential risks factors linked to the specific facility's structural aspects;
(d) Investigating the use of technology for rapid deployment of infectious disease treatment centre;
(e) Developing education programmes on emergency health facility design and management for different outbreaks preparedness and response.
Tέchne already responded to a wide array of context specific needs including a high variability of types of structures, which, after almost 7 months of activity, include traditional structures (16 requests), tent structures (8 requests), prefab structures or containers (10 requests). Through its responses Tέchne led to the construction of more than 1900 beds for COVID-19 patients across South America, Africa, Europe and Australia (Fig. 1).
The support is addressed to State Members, Ministries of health and other Ministries, UN agencies International and national organisations, health managers, that apply to their respective WHO regional office which, in turn, manages the exchange with Tέchne.
An Innovative Model of Work, in Four Projects
Thanks to its multidisciplinarity and the support coming from Tέchne, WHO can provide a complete response within 8 days, delivering to applicants layouts and diagrams to set up or repurpose existing facilities into treatment centres able to meet the COVID-19 minimum requirements (Fig. 2,3).
Figure 2 shows the ideal flow of work through the various phases of work: the WHO Strategic Health Operation Unit (SHO) works as pivot of a complex process of exchange between WHO Regional Office, local stakeholders applying for support, and the technical network of Tέchne. Figure 3 traces exchanges between the different actors involved through the design documents that are discussed and updated from the onset of the operation until the final deliverables. In each case, a request technical document is sent from the applicant to the WHO Regional Office, which, in turn, forwards it to the Strategic Health Operation Unit (SHO). The SHO selects one or more local experts to provide details and local technical support, as well as one or more Tέchne members that have the required expertise 一份技术申请文件,这个文件随后会被发送至战略卫生行动组。该行动组会选择一位或多位当地专家来提供技术支持申请的相关细节,同时选择一个或多个具备相关技能专长的Tέchne 成员。这份技术申请文件会由世卫组织地区办公室向工作组的所有成员公示。相关Tέchne 成员会和当地专家一起,提出第一版方案初稿,并交由战略卫生行动组讨论。经过必要修改之后,正式方案将拟定为一份技术报告,呈递战略卫生行动组,同时作为最终成果移交世卫组织地区办公室及申请者。在接受技术报告20天内,申请者需要提交一份反馈报告,战略卫生行动组的团队会负责修正方案。
这样的工作模式让战略卫生行动组作为每一次工作的实际协调者,在多样性的案例和技术支持类型中逐步摸索出一个清晰的行动范式。下面的几个案例是Tέchne 在过去几周支持的项目,也示例呈现了在这样广泛的地理多样性条件下所必须的多种路径。
1 加纳:新冠肺炎临时救治中心
阿克拉的临时救治中心临近机场,面积超过10 万m2。它由7 座纵向分布的长帐篷组成,建造仅花费3 周时间。阿克拉的救治中心项目是由世卫组织与世界粮食计划署合作的结果。这座新建筑主要会作为西非和中非国家的联合国员工及国际人道主义救援者的应急医院。在这一过程中,Tέchne 接到的任务是做一项流体力学分析,让建筑单元满足最低力学要求,并成为设计深化的基础单元。
这个项目严格遵照Tέchne 的行动流程。在接到请求后,Tέchne 成员需要采用计算流体力学模拟软件,研究用于收治新冠肺炎轻症患者的病患空间。他们的任务是分析设施中的空气流向及散布反向——尤其是在病人区——以确保及时稀释和排除病人周边的空气。这项研究中,还进行了不同设计策略的分析比较,以测试对现有通风条件的改良效果。
由于事态紧急,这座医疗设施被设计为一座轻型结构,一个钢框架体系支撑着两层织物表皮,织物之间的空气隔层确保室内外有7℃温差。这个模数化结构的运行还有赖于机械通风系统,系统配备了高效空气过滤器,从而满足新冠肺炎医疗设施的最低限通风要求。团队完成多项计算通风模拟分析,以评估和推荐最合适的建筑体系(图4)。
每座大帐篷都沿着一条中央廊道展开,这条廊道是建筑流线系统的中枢,两侧病房由轻质隔墙分隔,一系列小帐篷将大帐篷连接起来。
这个项目也成为即将实行的类似项目的试验场:一座类似结构将在维罗纳的空军基地建造,作为在机场等地确诊的境外输入病例的救治及隔离设施。由于申请者要求有一个负压独立仓,Tέchne专门对通风系统进行反复校验,确认是否需要技术修正或调整。所有这类联合国设施都是在意大利布林迪西设计的,那里有一个世界粮食计划署的分支机构(联合国人道主义应急仓库)。
3 Tέchne的工作模型应用于4个项目/Tέchne model of work applied to four projects

4 卧床病人周围的通风系统分析,定义每个单元和帐篷的总体布局/Analysis of ventilation system around supine patient, defining each unit and the general layout of the pavillions (图片来源/Courtesy: Tέchne)
2 布基纳法索:灾害韧性的新冠肺炎救治中心
这座新冠肺炎救治中心是一栋新建砖砌单层建筑,面积约3300m2。世卫组织国家办公室和该国卫生部一起提出请求,由Tέchne 设计一栋永久建筑,需满足如下条件:核验并隔离外来人员(因叛乱而从其他城市避难至此,或是因工作原因从拉各斯或阿布贾等中心城市来到这里);识别并隔离无症状病例;识别并隔离新冠肺炎的轻症患者。这个设计试图寻找一种创新解决方案,能够应对各类传播方式不同的传染病——霍乱、出血热、空气传播疾病等。尽管新冠肺炎在非洲已有超过62 万病例,但其他传染病仍是日常威胁,例如在刚果(金)的赤道省正爆发的埃博拉疫情(图5)。
在方案讨论过程中,出现了最大化自然通风以满足最低限度卫生需求的可能性,并发展为最终方案。这个设计目前正在等待审批,它采取了一个尽and know-how. The request technical document is presented by the WHO Regional Office to all members of the working group. The specific Tέchne members, together with the local experts, work on a first draft proposal which is presented to the SHO for discussion. Following necessary revisions, the proposal is formalised into a technical report which is presented to the SHO and then forwarded to the WHO Regional Office as well as the applicant as final deliverable. Within 20 days from the reception of the technical report the applicant is asked to send a feedback report, which the SHO team is in charge to revise.
This model of work allows SHO, as operative coordinator of each operation, to follow a clear protocol within a wide variety of different cases and types of support requests. The following are a few projects that Tέchne supported in the past weeks, and that exemplify the variety of approaches that are necessary in order to work in such geographical variability.
1 Ghana: Temporary COVID-19 Treatment Centre
The treatment centre in Accra is located nearby the airport over a surface of 100,000 square metres. It is organised as a cluster of 7 longitudinal pavilions, it was constructed in the course of 3 weeks. The project for the Accra treatment centre is the result of a joint effort between WHO and World Food Programme (WFP). The newly-built structure is intended to be used as an emergency hospital for UN staff and international humanitarian workers in West and Central African countries. Within this process, Tέchne was asked to develop a fluid dynamic analysis that would allow to meet minimum requirements and would work as a base unit for the development of the design.
The project closely followed the basic protocol of Tέchne. Upon receiving the request, the Tέchne member was asked to investigate the design of the patient space designated for patients with mild symptoms of COVID-19 via the use of computational fluid dynamics (CFD). The task was to analyse the airflow direction and dispersion throughout the facility – and in particular the patient bays – to ensure adequate dilution and extraction of contaminants generated by patients. During the investigation alternate designs were analysed to test improvements to the current ventilation strategies.
Due to the emergency, the facility was designed as a light structure, with a metal frame supporting two strata of fabric that enclose a layer of air providing a thermal difference of 7℃ between the inside and the outside. The modular structure counts as well on a mechanical ventilation system equipped with HEPA filters which allow it to meet the minimum requirements for ventilation within a COVID-19 facility. Several computational fluid dynamic studies have been done to assess and recommend the most suitable systems (Fig. 4).
Each pavilion is organised around a central corridor acting as the main distributive system, light partitions dividing each patient booth, and a series of sub-pavilions connecting each pavilion to the next.
The project also worked as testing ground for similar projects to be implemented: a similar structure will be installed in Verona within the military air force camp, to be used as a treatment and isolation facility for patients identified at points of entry such as airports. As the applicant is requesting an individual room with negative pressure, Tέchne is carrying out initial studies on the ventilation system to check whether any adjustments or modifications are needed. All UN structures of this kind are prototyped in Brindisi (Italy) for the World Food Programme that has a spinoff there (UNHRD).
2 Burkina Faso: COVID-19 Treatment Centre Resilient to All-Hazards
This COVID-19 treatment centre is a new brick, one-floor structure of around 3300 square metres. The WHO Country Office, together with the Ministry of Health, asked Techne to give support through the design of a permanent structure which would allow to: identify and isolate new arrivals (which would arrive from another town because of insurgency, or from main centres like Lagos or Abuja because of work); identify and isolate asymptomatic cases; identify and isolate those who are showing early symptoms of COVID-19. The idea was to develop an innovative solution that would be able to respond to a diverse array of infectious diseases regardless of the mode of transmission: cholera, hemorrhagic fevers, airborne diseases, etc. While COVID-19 is impacting Africa with more than 620,000 cases, other communicable diseases are and remain a daily threat, as shown by the ebola outbreak currently ongoing in the Equator Province in the Democratic Republic of Congo (Fig. 5).
In the course of the exchange, the possibility of maximising natural ventilation so as to meet minimum requirements emerged and was turned into a finalised proposal. The design, which is now pending approval, revolves around one layout designed to be as flexible as possible, for responding to several infectious diseases needs without the need of major adjustments. The design material delivered to the applicant included drawings, 3D, video and schemes showing the different flows of patients, healthcare workers and visitors as well as minimum ventilation requirements per area and use of PPE according to the latest WHO guidance.
3 Nigeria : Self-Quarantine for IDP Camps
The International Organisation for Migration (IOM) approached WHO with a request for support in the development of a design for spaces where people and families entering camps can spend a period of quarantine. The main requirement was for the structure to be an emergency-like shelter with integrated washing facilities per unit as well as front porch with cooking options. In the high-medium income settings, quarantine for asymptomatic individuals and mild-moderate cases is generally carried out at home. In most low-income settings, and especially in fragile contexts such as Internally Displaced People (IDP) Camps, informal settlements and refugee camps, quarantine is more difficult to carry out because of an obvious lack of facilities and infrastructures, but necessary in order to avoid the spread of the disease which would then prove even more difficult to be contained in an overcrowded and dense built environment. This project is intended to describe the core objective of a COVID-19 Selfquarantine facility and its functioning as the protective and preventive system for camps and camplike setting, supporting governments in including people affected by humanitarian crises within the outbreak readiness and response strategies.
The facility proposed by the WHO is meant to be placed next to the main camps in order to allows a safe, controlled, dignified and comfortable selfquarantine for new arrivals in order to (a) limit human to human transmission, including reducing secondary infections among close contacts and healthcare workers, preventing transmission amplification events, strengthening health facilities, identifying and provide optimised care for infected patients early, communicating critical risk and information to all communities, and 可能灵活的平面布局,从而在无需显著调整的前提下应对不同类型的传染病。提交给申请者的设计材料包括图纸、三维模型、视频及使用方案,展示了病人、医护工作者及访客的不同流线;以及根据最新世卫组织指导方案,如何满足单位面积的最低通风要求并采取个人防护措施。
3 尼日利亚:国内收容营的自我隔离
国际移民组织向世卫组织发出支持请求,需要设计一处可供初进收容营的个人或家庭进行一段时间隔离的设施。对这座设施的主要要求是,它应该发挥类似应急避难所的作用,每个居住单元应配有盥洗设施以及可用于烹饪的前门廊。对大部分中高收入者而言,无症状患者及轻微症状患者通常在家进行隔离。而对大部分低收入者而言,尤其是在类似收容营、非正规聚落、难民营这类脆弱环境下的人群,隔离会较难进行,因为他们显然缺乏必要的设备和基础设施;但这对于避免疾病传播又非常必要,而这类过度拥挤和高密度的居住环境会让隔离变得更困难。这个项目试图摸索新冠肺炎自我隔离设施的基本目标,以及它如何成为难民营或类似环境下的保护及预防体系,支持政府去帮助那些受人道主义危机威胁的人群,赋予其应急准备和回应策略。
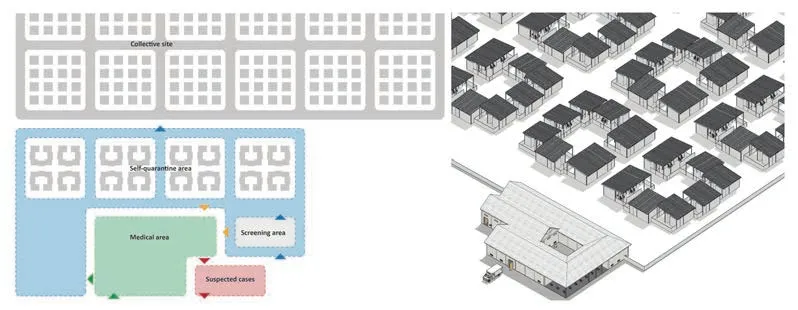
世卫组织建议建造的设施位于主收容营近旁,为新到者提供了一处安全、受约束、有尊严而舒适的自我隔离场地,以减少人际传染——包括降低密切接触者及医疗工作者的二次感染风险,避免可能扩大感染范围的活动,完善医疗设施,尽早识别感染患者并提供优化治疗,将关键风险信息传达给所有社区,以及辟谣等。这个项目与Tέchne 大部分其他项目不同,其设计请求是类型化的:Tέchne将设计一个收容营的理想模型,这个图解式方案将经过微调后应用于多个实际项目(图6)。
Tέchne 提出的方案包括一个居住区,以及配套的入住、筛查和医疗区域。隔离区域的大片居住区由一组独立结构组成,包括5 座单间单元(每套单间最多可容纳两人)以及两座双间单元(每套双间最多可容纳4 人)。每个单元都配备了厨房角、厕所、淋浴设施、床位及一个面向中心庭院的小平台。单元之间用矮墙隔开,保持视线沟通的同时确保必要的社交距离。

5 布基纳法索治疗中心的分布系统/Distributive system of the Burkina Faso treatment center (图片来源/Courtesy: Tέchne)
国际移民组织用本设计在尼日利亚东北部建造了一处自我隔离设施。该设施实现了设计中的居住方案,而医疗区域则没有建造。
4 意大利:未来的医院
该项目始于博洛尼亚医院提出的协助应对新冠肺炎紧急情况的申请,当时意大利卫生系统正面临危机,经受着病房人满为患、医护人员严重不足的考验。在第一次头脑风暴之后,项目的定位提高,希望能设计一个未来医院的示范项目。医院要求在应急响应组织的各个层面提供技术支持,包括基本医疗健康层面:为了找出应对这种复杂度的方案,世卫组织投入大量时间和人力,包括一位来自战略卫生行动组的专员负责流程,与医院管理及其技术部门人员、以及若干位参与设计工作的Tέchne 成员密切合作。这个项目被选为示范项目,主要出于以下原因:它临近一个新冠肺炎高发地区;它能够比其他类似境况的医院更好地控制医护人员感染;它已经集聚了一批创新成果,并投资于可再生能源、绿植屋顶等项目。
这座医院的城市尺度总平面是在1925 年由工程师朱利奥·马尔科维吉设计的,它由25 栋5 层高的建筑组成,容纳了不同的病房,自建成以来未经历大幅改造。项目由世卫组织与博洛尼亚医院合作,试图通过重新思考使用者的进入、离开和移动流线,将其改造为一栋韧性建筑。房间里不会布置超过两个床位——医院的容量会随之减小,为此地方管理者需合理地应对。
第一栋重点改造的建筑是妇产科病房,这一病房是在疫情的第一阶段危机最严重的区域,仅次于急救室。如今规范要求,在医院外部需设置一处检验筛查设施,包括分诊室、等候室、化验室等;此外,还将设置一条非新冠肺炎患者可以穿行整座医院的流线。设计理念是避免新冠肺炎区及非新冠肺炎区之间的空间区隔,而通过严格但灵活的流线区分来彻底控制感染,这样,医院也能够韧性地应对其他传染病(图7)。
设计在控制疫情方面能发挥怎样的作用?
在西非疫情爆发期间,尽管相关领域的机构和组织仍在建立和改善应对埃博拉疫情的经验,但科学界也见证了显著的研究进展,这带来了专属的疫苗以及新的实验性疗法。
自此,随着埃博拉病毒医疗手段的演进以及来自西非地区的经验积累,人们已采取重要的改良措施。在刚果(金)北部基伍和伊图里爆发疫情期间,多方行动者及专家积极响应,该领域也出现了多项创造性举措。其中包括卡特瓦医疗中心的创新设计,使得更高强度的医疗措施成为可能,并强化了人类学和社区参与的路径。
新的埃博拉病毒病医疗中心设计,采取先进的医疗设备和扩容的员工配置,得以从一个简单的隔离设施转型为一个具备更好的个人化医护条件的医疗中心,能够进行持续的患者观察及监控,并迅速采取反应措施。创新设计采取透明表皮,低风险区和病房区直接连通,以便促进更先进、密集的医疗措施。
设计采用私密的独立式病房,取代共用的开放式病房,这提升了患者隐私性及护理工作的强度,即便针对婴儿和孕妇等弱势人群也是如此。这是一个根本性转变,从一个隔离及控制性设施,转变为一个更全面的、以病人为中心的、精确护理的设施,拥有多学科的员工群体,全部设施都面向家庭和社区开放。它允许家庭探望在埃博拉病毒病医疗中心的亲人,这是一项革命性创举。
这项以病人为中心的设计,直接应用了该领域的技术及管理创新,充分结合西非积累的经验和专业技术,并在新冠肺炎疫情影响下进一步发展,为疫情爆发的准备和应急响应树立了新的里程碑,也为多项新冠肺炎疫情应对响应的相关行动提供了启示。
6 国内收容营方案自我隔离区中心布局及轴测/Layout of the center and axonometry of self-quarantine area for IDP Camp proposal(图片来源/Courtesy: Tέchne)
今天,我们与世界各地的大学及科研院所合作,试图强化这种医疗部门与建成环境间的新型多学科工作模式,以重塑空间与设计概念,及其在公共健康与突发卫生事件中的实用性。countering misinformation. Differently from most other Techne projects, the request for this project was typological: Tέchne would design a model camp, a diagrammatic layout which could then be applied to a number of real situations with minor modifications (Fig. 6).
The design proposed by Tέchne includes a residential sector as well as a registration, screening and medical area. The large residential sector of the quarantine area consists in a series of clusters of independent structures containing five single units (hosting up to two people) and two double units (hosting up to four people). Each unit includes a cooking corner, latrine and shower facilities, bed, and small outside terrace that opens up towards the central courtyard, and is separated from other units by a low fence allowing visual communication while allowing required distancing.
The IOM used the design for the construction of a self-quarantine facility in the Northeast of Nigeria, in which the scheme for the residential sector was applied, while the medical area was not built.
4 Italy: The Hospital of the Future
This project started out as a request of support for the Hospital of Bologna in the face of the COVID-19 emergency, as the Italian health system was struggling with full intensive therapy wards and too little staff to run them. After the first brainstorming phase, the project has gained in ambition, and is now intended to work as a model project for what a hospital should be in the future. The hospital requests technical assistance for the organisation of response at all levels, including at the primary health care level: to work out this level of complexity, the World Health Organisation is investing in it in terms of time and human resources, with one staff from the SHO team working specifically on this process, working closely with the hospital management and its technical department, as well as several Tέchne members that will be part of the design task force. This project was chosen as showcase for a number of reasons: because it was close to one of the major COVID-19 hotspots, because it was able to contain the infection of healthcare workers much better than other hospitals in similar conditions, and because there is already a network of innovation that gravitates around it and that has been investing in renewable energies, green roofs, etc.
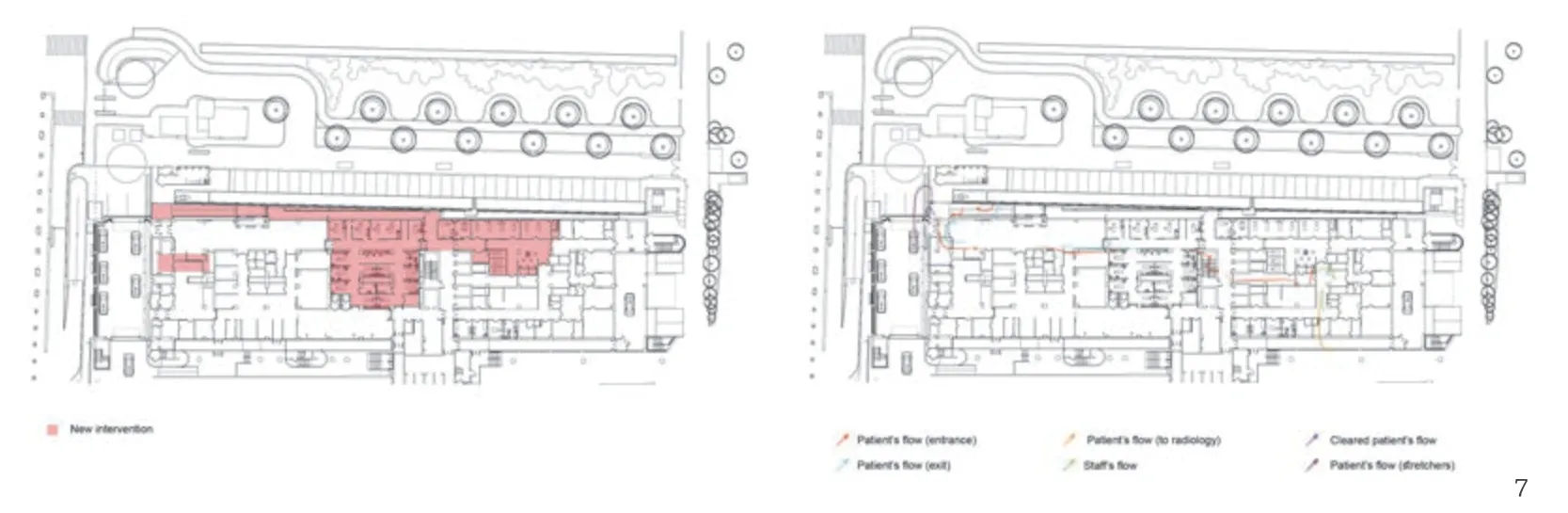
7 医患流线图/Diagram of patient-staff flow(图片来源/Courtesy: Tέchne)
The Hospital's urban-scale layout was designed in 1925 by Engineer Giulio Marcovigi as a series of twenty-five 5-storeys pavilions hosting different wards, and hasn't been subject to major interventions since. The project carried out by WHO and the Hospital of Bologna intends to turn it into a resilient structure, by a complete rethinking of users' fluxes of entrance, exit and movement throughout. Rooms will have no more than two beds – with a consequent reduction of the hospital's capacity, a factor that the Regional administration will have to cope with creatively.
The first pavilion to undergo major change will be the one hosting the Maternity Ward, which was the ward to have typically the most trouble during the first phase of the pandemic, after the Emergency Room. Norms now require that there be a screening outside of the hospital, that includes triage, waiting room, sampling test; in addition, there will be a non-COVID itinerary that patients can follow throughout the hospital. The idea is to avoid spatial separation between COVID- and non-COVID areas, but to obtain full containment through a strict but flexible separation of distributive fluxes, so that the hospital can be resilient to other infectious diseases as well (Fig. 7).
What Is the Role of Design Towards Containing the Pandemic?
During the Western Africa outbreak, while institutions and organisations working in the field were building and enhancing their own experience in ebola outbreak management, the scientific community witnessed an important research boost which led to specific vaccine and new experimental treatments.
Since then, following the evolving trend of Ebola Virus Diseases (EVD) medical care and based on the West Africa's lessons learned, important steps forward have been made. During the North Kivu and Ituri outbreak in D.R. Congo, with different actors and expertise engaged in the response, several innovations have been seen in the field. Amongst them the innovative design of Katwa treatment centre which allowed more intensive medical care and strengthened the anthropological and community engagement approach.
New Ebola Treatment Centre (ETC) design with advanced medical tools and expanded staff have enabled the transition from a simple isolation facility to a centre which allows better, individualised, patient care through continuous patient observation and monitoring, and fast response. The innovative design, the use of transparent surfaces and the direct access to the patients from the low risk zone have facilitated and enhanced more advanced, intensive care interventions.
The use of private, self-contained rooms instead of shared, open-ward facilities have allowed for patient privacy as well as intensive care, even to the most vulnerable populations, the very young and pregnant. This has been a fundamental change from being an isolation and containment facility to a more holistic, patient-centred, acute-care facility with multi-disciplinary staff, all accessible to families and communities. Allowing families to communicate with their loved ones being cared for in ETCs has been a major milestone.
This patient-oriented approach, supported by technical and management innovations directly developed in the field, nestled in the experience and expertise built from Western Africa and further developed during the current COVID-19 pandemic, placed a new fundamental milestone for outbreaks preparedness and responses and inspired several activities part of the COVID-19 pandemic's preparedness and response.
Today, working with several universities and technical institutions around the world, we are trying to strengthen this new multidisciplinary model of work in between the health sector and building environment reshaping the concept of space, design and its usability within public health and health emergencies.
