Cholecystoenteric fistula with and without gallstone ileus: A case series
2020-03-03MuricioGonzlezUrquijoMrioRodrteShdeGerrdoLoznoBldersGerrdoGilGlindo
Muricio Gonzlez-Urquijo , , , Mrio Rodrte-Shde , , Gerrdo Lozno-Blders , Gerrdo Gil-Glindo ,
a Tecnologico de Monterrey, Escuela de Medicina y Ciencias de la Salud, Dr. Ignacio Morones Prieto O 30 0 0, Monterrey 64710, México
b Department of Surgery, Hospital Metropolitano “Dr. Bernardo Sepúlveda”, Secretaria de Salud de Nuevo León, Adolfo López Mateos No. 4600, San Nicolás de los Garza 66400, México
Keywords: Cholecystoenteric fistula Gallbladder disease Biliary-enteric fistula Gallstone ileus Intestinal obstruction
ABSTRACT Background: A cholecystoenteric fistula (CEF) is an uncommon complication of gallstone disease. The aim of this study was to present our experience of a series of patients with CEF, presenting with or without gallstone ileus, along with their surgical outcomes. Methods: From 2015 to 2018, 3245 consecutive patients underwent cholecystectomy for gallbladder dis- ease at our institution, of which 15 were diagnosed with a CEF. All electronic medical records were ret- rospectively reviewed. Results: Fifteen patients presented with CEF. Ten patients presented cholecystoduodenal fistula, four pa- tients cholecystocolonic, and one patient cholecystogastric counterparts. Twelve patients were female. The median patient age was 61 years (range 33-86 years). Five patients presented with gallstone ileus treated by laparotomy and enterolithotomy. In ten patients, a laparoscopic approach was attempted, but conver- sion to open surgery was necessary for eight of them. The median operative time was 140 min (range 60-240 min), and the median operative blood loss was 50 mL (range 10-600 mL). The procedure-related morbidity and mortality rates were 13.3% and 6.7%, respectively. Conclusions: There is no consensus on the best treatment modality for a CEF, as the treatment outcome is mostly dependent on the surgeon’s expertise and the patient’s condition. Not all CEFs are accompanied by gallstone ileus. For such case, the main purpose is to resolve the intestinal obstruction and, unless necessary, avoidance of the gallbladder area.
Introduction
A cholecystoenteric fistula (CEF) first described by Bartholin in 1654, is relatively rare. This type of fistula, is a well-recognized complication of biliary disease, with a reported incidence of 3%-5% in patients with cholelithiasis, and is designated as a sponta- neous anomalous tract between any part of the gallbladder and a segment of the surrounding gastrointestinal tract, the most fre- quent localization being the duodenum, accounting for 75%-80% of all such fistulas, followed by the colon and stomach [1-4] .
Because of the lack of particular symptoms, as compared with cholecystitis, it is difficult to diagnose a CEF preoperatively. Pre- viously, CEF was always an incidental finding during surgery, but with the improvement of imaging modalities, such as computed tomography (CT) and magnetic resonance imaging, along with the application of endoscopic technology, the preoperative diagnosis of a CEF has been significantly improved, but is achieved in only 8%-17% of cases [4 , 5] .
The common causes of CEF include chronic cholelithiasis, peptic ulceration, malignant neoplasms, Crohn’s disease, among others [5-8] . The present study aims to present a case series of patients with CEFs due to chronic cholelithiasis and to display our personal surgical experience treating this uncommon type of bil- iary disease, along with their surgical outcomes.
Methods
The Institutional Review Board approved the study protocol (approval No. 031). From 2015 to 2018, 3245 consecutive patients underwent cholecystectomy for gallbladder disease at our in- stitution. Among them, 15 patients were diagnosed with a CEF, either preoperatively or intraoperatively. We searched the surgical database for all patients diagnosed with this type of fistula and retrospectively reviewed all electronic medical records. The patient demographics, clinical characteristics, diagnostic meth- ods, surgical procedures, treatment outcomes, and follow-ups were all documented and organized. All patients underwent a physical examination, laboratory testing, and evaluation of the gallbladder either by ultrasonography (US) or CT. Based on the patient’s condition, other imaging modalities, such as magnetic resonance cholangiopancreatography (MRCP), or endoscopic ret- rograde cholangiopancreatography (ERCP), were performed. If choledocholithiasis was encountered, the patient underwent ERCP with subsequent cholecystectomy. Laparoscopic cholecystectomy under general anesthesia with a standard four-port technique was attempted in most patients. Conversion to open surgery was left to the discretion of the surgeon. When dense adhesions to adjacent organs and impacted stones in Hartmann’s pouch rendered access to Calot’s triangle difficult, a fundus-first dissection technique was applied, and subtotal cholecystectomy was performed.
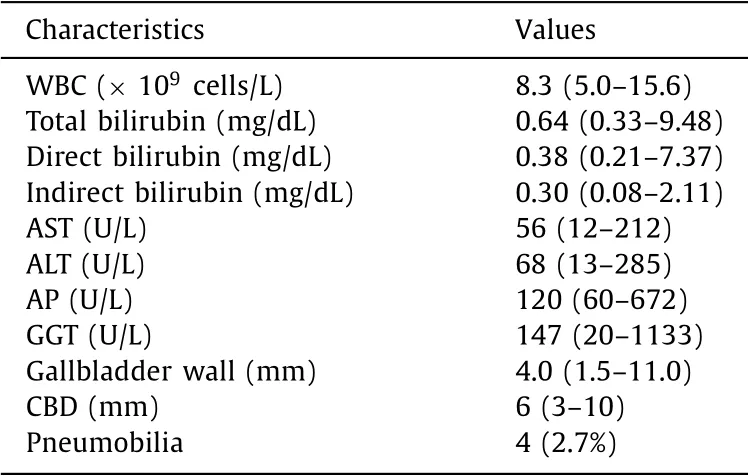
Table 1 Paraclinical characteristics.
All patients were followed up in the outpatient clinic within the first week, the first month, and then yearly. Patients were exam- ined clinically, and liver function was evaluated at each follow-up visit.
Statistical analysis
Continuous variables were reported as the median, and range while categorical variables were reported as frequencies and per- centages. Data analysis was performed with a combination of Excel 16.0 (Microsoft Corporation, Redmond, WA, USA) and R software 3.4 (R Core Team, Auckland, New Zealand).
Results
In our series, 12 patients were women, and three were men. The median age was 61 years (range 33-86 years). Ten patients had cholecystoduodenal fistula (CDF), four patients cholecystocolonic fistula (CCF), and one patient cholecystogastric fistula (CGF). Five patients had concomitant diabetes mellitus (DM) and systemic ar- terial hypertension (SAH), four had only SAH, and two had only DM. All patients had > 2-year history of abdominal pain, with a median time of exacerbation of pain in the right upper quadrant before surgical treatment of 3 days (range 1-10 days). Only two pa- tients had jaundice due to choledocholithiasis at presentation. Four patients presented with an elevated white blood cell count, with a median value of 8.3 × 109cells/L (range 5.0 × 109-15.6 × 109cells/L). Liver function test results were detailed in Table 1 .
The US was the initial imaging modality in 11 patients, which revealed gallstones and features of acute cholecystitis in all cases, with a median gallbladder wall thickness of 4.0 mm (range 1.5-11.0 mm). Two patients presented with choledocholithiasis, de- tected by US, resolved with ERCP. During the ERCP, visualization of a CDF was seen in one of the patients, while there was no fis- tulous opening in the other. Both patients underwent sphinctero- tomy with the placement of a common duct stent in the patient with a CDF. Overall, a preoperative diagnosis of CEF was achieved in six patients, one with an initial diagnosis of choledocholithiasis by ERCP and five with a CT scan ( Fig. 1 ).
Of the 10 patients with CDF, four converted from laparoscopy to open procedure, performing partial cholecystectomies. Primary closure of the duodenum and a Graham patch was achieved in two patients each, respectively. In one patient, a laparoscopic pro- cedure was auspiciously completed, and total cholecystectomy was completed while performing a Graham patch on the second por- tion of the duodenal wall. Laparotomy was performed for four pa- tients with gallstone ileus, completing an enterolithotomy in the terminal ileum. Furthermore, in half of those patients ( n = 2) dis- mantling of the fistula was accomplished by total cholecystectomy and primary closure of the duodenum. The fistula was left intact in the other two patients, and only the intestinal obstruction was resolved. An open approach was completed in one patient, during which the common bile duct (CBD) was found to be firmly adhered to the duodenum along with the fundus of the gallbladder; hence, partial cholecystectomy with T-tube insertion within the CBD and a Graham patch on the duodenum was done.
Of the four patients with CCF, a laparoscopic approach was at- tempted in three of them, with conversion to open surgery in two patients. In one patient, a colostomy at the site of the fistula was performed, and a partial cholecystectomy was achieved. Two pa- tients were treated with primary closure of the transverse colon. In one patient, conversion to open surgery was needed, performing a partial cholecystectomy, and in the other a laparoscopic chole- cystectomy was auspiciously performed. One patient was treated with enterolithotomy alone, for intestinal obstruction due to sig- moid gallstone ileus.
One patient presented a CGF on the lesser curvature, treated with a partial cholecystectomy. An omental patch was placed at the site of the defect in the lesser curvature.
The patient characteristics and surgical outcomes were summa- rized in Table 2 .
In global, trans-operative cholangiography was performed in six of the 12 patients who previously underwent cholecystectomy, but no filling defect of the biliary tract was detected. Each had anoma- lous communications from the gallbladder to the duodenum, colon or stomach. In the 12 patients, a tube drain was left in the subhep- atic space and was removed within a median of 3.5 days (range 2-10 days).
The median operative time was 140 min (range 60-240 min), and the median intraoperative blood loss was 50 mL (range 10-600 mL). Regarding the site of the fistula, on the gallbladder side, the fundus was the site of the fistula in six patients, the body in four, the Hartmann pouch in two, and in three patients, the site was uncertain due to firm adhesion and a significant fibrotic pro- cess.
Overall, procedure-related morbidity and mortality were found in two patients and one patient, respectively. One patient had a remaining stone within the CBD that was treated 4 days after the initial procedure with ERCP, which achieved an outstanding outcome, another patient presented paralytic ileus on postopera- tive day (POD) 3 treated with prokinetic agents, and one geriatric patient died from septic shock due to intestinal obstruction sec- ondary to gallstone ileus. Only enterolithotomy was performed, but the patient did not recover from renal failure and died on POD 20 in the intensive care unit. The median length of hospital stay was 7 days (range 3-20 days). Fourteen patients were currently followed up in our clinic, with a median follow-up period of 14 months (range 8-40 months). All are symptom-free with normal liver function. None of the three patients with gallstone ileus, for whom the gallbladder area was not addressed, have reported col- icky biliary pain. Final histopathological analysis revealed chronic cholecystitis in all patients.
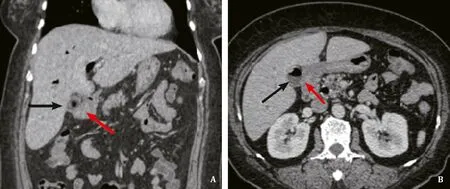
Fig. 1. CT of the abdomen with intravenous contrast of a 61-year-old female patient. The black arrow identifies the gallbladder with aerobilia. Red arrow identifies the duodenal stump . The gallbladder is in communication with the duodenum. A: Coronal view; B: Axial view.
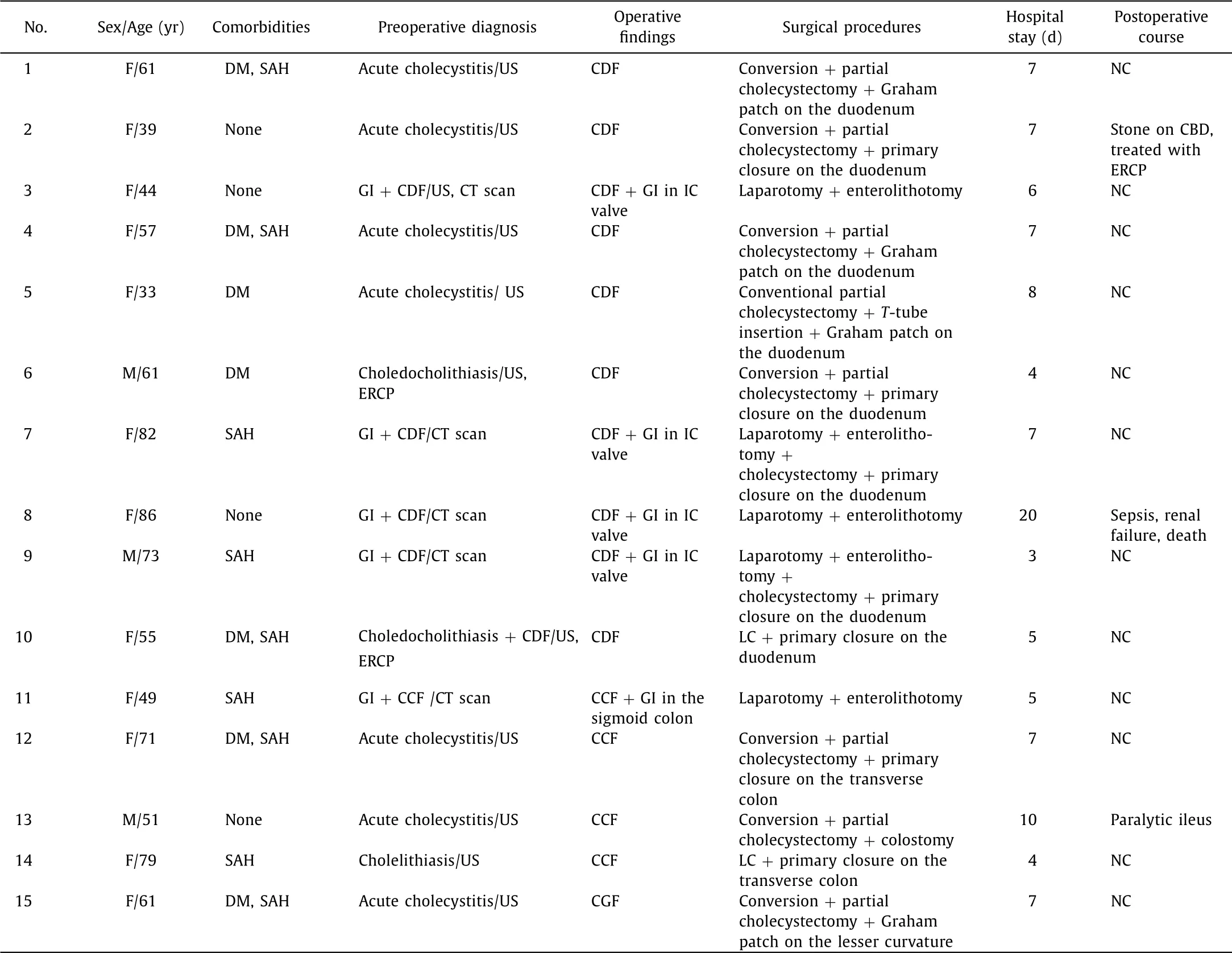
Table 2 Patient characteristics, surgical treatments, and outcomes.
Discussion
A CEF is a rare clinical condition that occurs primarily in the fe- male geriatric population [9] . In the present study, more than half of the patients were geriatric, and 80% of the population were fe- male. CEF has been reported to occur in 3%-5% of patients with cholelithiasis and 0.15%-4.8% of all who undergo surgery to the bil- iary tract. The incidence (0.46%) in the present study was lower than in early reports [9 , 10] , and was almost the same as that re- ported by Li et al. [4] , Duzgun et al. [5] and Chowbey et al. [2] . The most frequent type of biliary fistula is CDF, followed by CCF and CGF [1 , 3] . In our patients, 66.7%, 26.7%, and 6.7% presented with these types of fistulas, respectively.
An inflamed, contracted gallbladder stuck firmly to contiguous viscera in a patient with a long history of chronic cholecystitis should alert the surgeon to the possibility of a cholecystoenteric fistula [2] . Li et al. [4] advised that a long history of cholecystolithi- asis, especially > 5 years, should increase suspicion for the presence of CEF when encountering the gallbladder firmly adhered to a part of the gastrointestinal tract.
The clinical presentation of this condition is mostly chronic. In this series, all patients had a history of abdominal pain for a min- imum of 24 months, and these symptoms (i.e., epigastric or right upper quadrant pain, nausea, and vomiting) were not discernable from the symptoms of most gastrointestinal conditions, such as cholelithiasis or acute cholecystitis [5 , 11] . In our series, seven pa- tients had an initial diagnosis of acute cholecystitis, and one pa- tient had a diagnosis of cholelithiasis, which was operated in an elective manner. We made the preoperative diagnosis of CEF in 40% of our patients, making it higher than other series, where a preop- erative diagnosis was achieved in 8% -31% [4 , 12] .
The majority of the diagnoses are made intraoperatively, unless the biliary tract is involved, which consequently causes jaundice, cholangitis, or pancreatitis [13] . Most studies report that the fistu- las are revealed incidentally by other radiologic studies to inves- tigate biliary conditions, pancreatic diseases, or intestinal obstruc- tions [5] . Intestinal obstructions are easily detected by CT, which is also useful to exclude neoplastic lesions located at the hepatic hilum or into the liver. Pneumobilia may be evident by CT, being highly suggestive of a biliary-enteric fistula [12 , 14] . The patients who presented with signs and symptoms of intestinal obstruction underwent CT scans, showing gallstone ileus in all cases ( n = 5), with pneumobilia present in four of them.
MRCP has superior diagnostic accuracy in about 50% of cases, thereby providing better information about the structure and con- tents of the biliary tree [15] . The diagnostic accuracy of ERCP for a biliary fistula varies from 55% to 90%, but this modality also of- fers the advantage of a therapeutic role [12 , 16 , 17] . In this series, to achieve a preoperative diagnosis, MRCP was not applied in any of our patients, but ERCP was used for two patients, which detected a CDF in one patient who underwent sphincterotomy and place- ment of a biliary stent. The stent was removed at 2 months post- cholecystectomy. For the other patient, a stone was extracted from the CBD, and sphincterotomy was effectively achieved, although no fistula was observed.
There are two possible explanations for the nature of a CEF. The first theory is based on the erosion of stones through the injured wall of the gallbladder into the duodenum, colon, or stom- ach, causing a gallstone ileus ( Fig. 2 ) [10 , 18] . Furthermore, since the gallbladder is decompressed, and if no stone remains, the pa- tient may become asymptomatic. If the patient is exceedingly ill due to electrolyte imbalance, sepsis, or other disorders caused by the intestinal obstruction due to a gallstone ileus, under no cir- cumstances should the fistula be repaired or closed because of the increased risk of additional contamination from further dissection in the area of the gallbladder. We only repaired the fistulas of two of the five patients with gallstone ileus because the gallbladder was not firmly adhered to the duodenum and unruラed dissection was feasible. For the other three patients, the inflammatory pro- cess caused significant derangement of the anatomy of Calot’s tri- angle, so we opted to leave the fistulas untreated.
The second theory of the formation of this type of fistula in- volves acute inflammation with obstruction of the cystic duct, causing the gallbladder to stretch and swell, sometimes rubbing the gastrointestinal tract and forming adhesions between two or- gans with subsequent gangrenous changes with eventual erosion, thereby establishing a lasting anomalous communication [5] .
The standard treatment when encountering a CEF is cholecys- tectomy, and repair of the fistulous opening, either by a laparo- scopic, or an open approach, depending on the experience of the surgeon and the condition of the patient [2] . Whenever difficult dissection or significant bleeding is encountered in a laparoscopic method, intestinal suturing might be challenging along with an in- creased risk of injury to the biliary tree, in which cases, conver- sion to open surgery might be necessary [4] . The conversion rate from the laparoscopic approach in the current study was 80% due to trouble visualizing the anatomy of the gallbladder area in most cases and because of significant hemorrhage from Calot ´s triangle in one case, which occurred during dissection of the inflamed tis- sue around the gallbladder and duodenal area, but there was no damage to any significant vascular structure.
A defect on the duodenum can be closed with sutures [4] or a Graham patch [19] , while leaving a T-tube during duodenostomy after previous repair attempts had failed [20] . We suggest the use of the first two techniques to restore the duodenal anatomy since there was no leakage with either of these methods in this series.
On the patients where the colon was involved, we performed on two of them, partial cholecystectomies, and on one a completed counterpart. On two patients we performed primary closure of the transverse colon, and on another, a colostomy was achieved with colonic reconnection auspiciously implemented 20 weeks later. We encountered a 49-year-old female patient with a gallstone ileus on the sigmoid colon along with a CCF, opting for conservative management, achieving only an enterolithotomy, with positive out- comes. This unusual site of impaction of the stone is exceptionally infrequent, occurring only in around 5% of all patients with gall- stone ileus [3] .
In this series, one patient developed jaundice and abdominal pain on POD 2. He presented with a stone within the CBD, as observed during MRCP. On POD 3, the stone (diameter, 4 mm) was extracted under ERCP guidance, and sphincterotomy was per- formed. Another patient developed paralytic ileus treated medi- cally without complications. The only death was an 86-year-old fe- male patient who presented with gallstone ileus, severe abdominal distension, and acute renal failure. Laparotomy with enterolitho- tomy was performed, but the patient succumbed to kidney failure on POD 20. Hence, the mortality rate in this study was 6.7%, which was lower than the rate of 25% in a series of 12 patients reported by Duzgun et al. [5] and lower than that in another study of 15%-22% among patients with a CEF [9] .

Fig. 2. Diagram exposing the process of a cholecystoduodenal fistula creation. A : Adherence formation and inflammatory tissue surrounding the gallbladder in touch with the duodenum; B : Erosion of the gallbladder’s wall into the duodenum, creating an anomalous communication.
In conclusion, CEF is an infrequent finding during cholecystec- tomy, implying a surgical challenge for the surgeon. When the US demonstrates a shrunken gallbladder with a thick wall of a patient with a long history of cholecystolithiasis, a supplemental image study is recommended (CT, MRCP, or ERCP) in order to rule out any other biliary disease. During surgery, if the gallbladder area is fixed by extensive inflammatory tissue and is stringently attached to the gastrointestinal tract, the surgeon should be highly suspi- cious of the presence of a CEF. There is no consensus on the best treatment for this condition, as the outcome is dependent on the surgeon’s expertise and the condition of the patient. A CEF is not always accompanied by gallstone ileus. For such cases, the primary purpose is to repair the intestinal obstruction, while avoiding the gallbladder area, unless there is definite proof of gallstones in the biliary tree.
Acknowledgments
Research group of Bioengineering and Regenerative Medicine from Tecnologico de Monterrey.
CRediT authorship contribution statement
Mauricio Gonzalez-Urquijo:Conceptualization, Data curation, Writing - original draft.Mario Rodarte-Shade:Data curation, Formal analysis, Investigation, Methodology.Gerardo Lozano- Balderas:Project administration, Software, Supervision.Gerardo Gil-Galindo:Validation, Writing - review & editing.
Funding
None.
Ethical approval
This study was approved by the Ethics Committee of Tecno- logico de Monterrey, Escuela de Medicina y Ciencias de la Salud. The study protocol was approved by the Institutional Review Board of our Institution (approval No. 031).
Competing interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the sub- ject of this article.
杂志排行
Hepatobiliary & Pancreatic Diseases International的其它文章
- Impact of EBV infection and immune function assay for lymphoproliferative disorder in pediatric patients after liver transplantation: A single-center experience
- Hepatobiliary&Pancreatic Diseases International
- Intraoperative management and early post-operative outcomes of patients with coronary artery disease who underwent orthotopic liver transplantation
- Acute onset of autoimmune hepatitis in children and adolescents
- Liver stiffness as a predictor of hepatocellular carcinoma behavior in patients with hepatitis C related liver cirrhosis ✩
- Treatment and prognosis of hepatic epithelioid hemangioendothelioma based on SEER data analysis from 1973 to 2014