Radiofrequency and malignant biliary strictures: An update
2019-02-27FrancescoAuriemmaLucaDeLucaMarioBianchettiAlessandroRepiciBenedettoMangiavillano
Francesco Auriemma, Luca De Luca, Mario Bianchetti, Alessandro Repici, Benedetto Mangiavillano
Abstract Malignant biliary strictures are usually linked to different types of tumors,mainly cholangiocarcinoma, pancreatic and hepatocellular carcinomas. Palliative measures are usually adopted in patients with nonresectable or borderline resectable biliary disease. Stent placement is a well-known and established treatment in patients with unresectable malignancy. Intraductal radiofrequency ablation (RFA) represents a procedure that involves the use of a biliary catheter device, via an endoscopic approach. Indications for biliary RFA described in literature are: Palliative treatment of malignant biliary strictures, avoiding stent occlusion, ablating ingrowth of blocked metal stents, prolonging stent patency,ablating residual adenomatous tissue after endoscopic ampullectomy. In this mini-review we addressed focus on technical success defined as deployment of the RF catheter, virtually succeeded in all patients included in the studies. About efficacy, three main outcome measures have been contemplated: Biliary decompression and stent patency, survival. Existing studies suggest a beneficial effect on survival and stent patency with RFA, but current impression is limited because most of studies have been performed using a retrospective design, on diminutive and dissimilar cohorts of patients.
Key words: Radiofrequency; Ablation; Endoscopic retrograde colangiopancreatography;Malignant biliary strictures
INTRODUCTION
The aim of this mini-review is to assess the utility of radiofrequency ablation (RFA) in malignant biliary obstruction (MBO). Malignant biliary strictures represent a diagnostic and therapeutic open question for biliary endoscopist. MBO is usually linked to different types of tumors, mainly cholangiocarcinoma, as well as pancreatic and hepatocellular carcinomas. Traditionally palliative measures have been adopted in patients with nonresectable or borderline resectable biliary disease. Stent placement is a well-established and widely accepted treatment in patients with unresectable malignancy[1,2], with a lower rate of adverse events such as procedural complications and post-stenting occlusion than surgical decompression[3]. The use of metal stents decreases the need for re-intervention and the occurrence of cholangitis compared to plastic or polyethylene stents[4]. However, stent patency is difficult to preserve due to neoplastic in- and over-growth, epithelial hyperplasia, and sludge deposition[5].
Efforts have been ongoing to develop different palliatives interventions to prolong patency of metallic biliary stents. Some of the interventions which have been studied include photodynamic therapy (PDT), intraductal radiotherapy and RFA[6-8].
RFA is a well-recognized percutaneous approach that has widely been used in the management of hepatocellular carcinoma and metastatic hepatic malignancy, with demonstrated effectiveness[9].
Even within the bile duct, RFA can be performed by specific endo-biliary probes that enable increased precision in the delivery of thermal energy in the biliary tree resulting in decreased epithelial hyperplasia and tumor ingrowth. Several studies have confirmed the safety and feasibility of these procedures for clinical use with promising results reported for the palliative treatment of malignant biliary strictures,preventing stent occlusion, ablating ingrowth of blocked metal stents, prolonging stent patency, ablating residual adenomatous tissue after endoscopic ampullectomy[10].
TECHNICAL ASPECTS
RFA creates an electrical passage through the body of monopolar probes, between an electrode and a grounding pad placed on the patient. Additionally, it may be generated by two interstitial electrodes with bipolar catheters, by using an alternating current. Resistance heats the surrounding tissues burning up to elevated temperature(50°C-100°C) and causing protein denaturation followed by cell desiccation and coagulative necrosis. The most contiguous areas to the electrode undergo to the highest current and heat shock due to reduced electrical conductivity of tissues. On the other hand, the parts of the tumor most distant are only burnt and necrosis is not determined because thermal conduction is not sufficiently high[11,12].
Intraductal RFA represents a procedure that encompasses the use of a biliary catheter device, via an endoscopic approach. For biliary RF, two devices are designed to be used over a guide wire during endoscopic retrograde colangiopancreatography(ERCP): Habib™ EndoHBP and ELRA™.
The RFA catheter Habib EndoHPB (EMcision Ltd, London, UK; Boston Scientific,Marlborough, Massachusetts, USA) is a disposable device properly designed for endoluminal delivery of RFA into the biliary system. It is an 8 Fr RFA probe, with bipolar conduction features. It is well-suited for large working channel of duodenoscopes, mostly over 0.035-inch guidewires. The catheter has two ring electrodes, 8 mm distant from each other. It provides local coagulative necrosis over a 2.5 cm length, in circular and ellipsoidal way (Figure 1). The highest energy accumulation is achieved between the electrodes, placed below and above the target.VIO 200D or 300D generator (Erbe Elktromedizin, Tubingen, Germany) are usually used, delivering high-frequency bipolar current. Generator setting mostly lies on:Power between 7 W-10 W, effect set at 8 for a duration of 30 s-90 s.
ELRA™ (EndoLuminal Radiofrequency Ablation, Taewoong Medical, South Korea)probe has been recently introduced. It allows strict control of temperature at the interface tissue-electrode. This probe has two sizes (18- and 33-mm length), with a diameter of 7 Fr. It contains four bipolar electrodes which provide linear ablation.There is no need for ground pads. The generator is VIVA (Taewoong Medical, South Korea) mostly set to two minutes interval, maximum temperature of 80°C and a power of 10 watts (Figure 2). In animal studies this represents the ideal setting to reduce the charring process, allowing more prolongated current stream and more effective tissue ablation[13,14].
To perform biliary RFA, biliary tract is cannulated as a standard ERCP procedure.Then a cholangiography is performed to distinctly visualize the location of the stricture and to define its extent and width. Though not crucial, a sphincterotomy is generally completed. In addition to this, dilation of the stricture, mostly by mean of a balloon, could be performed before RFA procedure. The probe is then inserted over the guidewire across the stricture.
RF energy is applied for the desired period, according to different RFA probe manufacturer's indications. Before withdrawn the probe, a break period of about 60 s is necessary to prevent tissues from adhering to the electrodes. Usually multiple RF applications are completed during the same session. Generally it is preferred from the proximal verge of the target to the distal one, with tiny overlap in order to decrease the risk of complications, mainly perforation.
Once the probe has been removed, coagulated tissue debris are swiped by mean of balloon, and a plastic or metal stent is positioned to guarantee biliary drainage[15,16].
MALIGNANT BILIARY OBSTRUCTION
Over the last 8 years, more than 350 patients were reported in the literature to have been undergone endoscopic biliary RFA. Indications were mainly malignant strictures and occluded self-expanding metal stents (SEMS).
Nearly in all studies, malignant strictures accounted cholangiocarcinoma or pancreatic cancer, but also other malignant strictures have been considered, such gallbladder cancer, hepatic carcinoma and metastatic cancers as well.
In this mini-review we will focus on retrospective “largest” papers including more than 40 patients (including controls group) and all prospective and randomized controlled trial studies published on topic up to August 2018. Table 1 summarizes the main characteristics of the included studies (study design, population, intervention,RFA probe, outcomes, main findings)[17-25].
Technical success defined as deployment of the RF catheter was essentially succeeded in all patients. About efficacy, main outcome measures considered are:Biliary decompression and stent patency, survival. As for stent patency and biliary drainage different outcome measures have been considered: 30- or 90-d patency rate,median time patency. Moreover, in these studies different types of procedures have been grouped in the same series (RFA before stenting, RFA without stenting, RFA in occluded SEMS, combined endoscopic and/or percutaneous RFA), dissimilar stents have been used (metallic or plastic), different stenting replacement strategies have been adopted (on demanding, 3 mo scheduled ERCP). Despite this lack of homogeneity, the results of the included studies are quite similar, with 90-d patency ranging between 80%-86%, up to 69% ad 180-d[17,24]; median patency ranged between 170 d[19]and 200 d[25]. RFA + metallic stent placement outperformed RFA + plastic stent strategy, doubling median patency rate[19]. About survival, all but one study, in which similar results have been observed between RFA and PDT[21], showed very encouraging results in patients performing one or more RFA sessions. Overall survival ranged between 226 and 396 d[22,23,25], and RFA + stent outperformed stenting alone strategy in all study comparing them.
With regard to adverse events (AE), frequency ranged between 6.3% and 33.3%.Most of these concerns the bilio-pancreatic compartment: Acute pancreatitis,cholangitis, cholecystitis, and haemobilia. Only one study report two severe adverse events: One hepatic liver infarction and one hepatic coma[19].
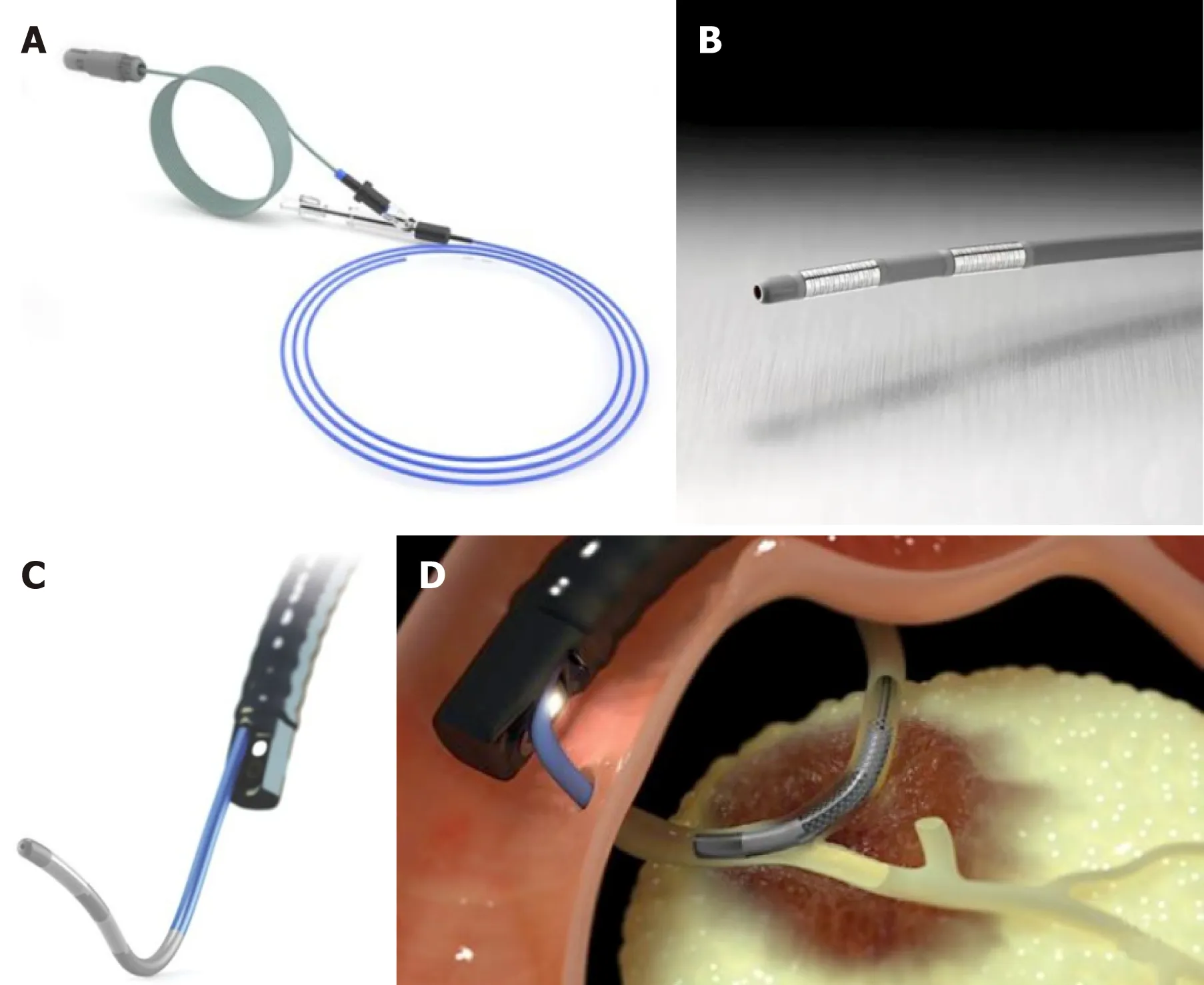
Figure 1 Habib™ EndoHPB Catheter. A, B: Radio Frequency ablation catheter; C, D: Duodenoscope and catheter in endoscopic retrograde colangiopancreatography simulation model. From:https://www.bostonscientific.com/content/gwc/en-US/products/rf-ablation/habib-endohpb-bipolar-radiofrequency-catheter.html.
OCCLUDED SEMS
Only two studies have specifically addressed biliary RFA in case of occluded metal stents. Kadayifci et al[26]matched endobiliary RFA to controls in which plastic stents were inserted across the stent. The study group included 25 patients treated with RFA using a Habib™ endoprobe inside the SEMS. The control group involved 25 patients treated only with placement of a plastic stent into an occluded SEMS. Biliary drainage was restored in all patients. Stent patency was evaluated at 90 d, reaching 56% and 24% in the RFA and control groups, respectively. In addition to this, stent patency was significantly longer in the RFA group compared to the control group (119.5 d vs 65.3 d, P = 0.03). 30-d mortality rate and 3- and 6-mo survival rates did not significantly differ between the RFA group and controls (P > 0.05).
The other study, recently published, is a feasibility prospective case series of 7 patients treated with novel temperature-controlled RFA probe ELRA™ (Taewoong,South Korea)[14]. Nine procedures were performed. Seventy percent of patients (5/7)required additional procedures and stent placement to guarantee optimal drainage.There were no procedure-related complications.
ENDOSCOPIC RADIOFREQUENCY ABLATION OFINTRADUCTAL RESIDUAL OF AMPULLARY ADENOMA
Ampullary adenomas are usually treated by endoscopic papillectomy. Nevertheless,ampullary adenomatous residuals spreading into the distal common bile duct or Wirsung represent a tricky condition.
Intraductal adenoma typically has been considered a contraindication to endoscopic management. Surgical treatment represents the gold standard in this condition. Conversely, a pancreaticoduodenectomy or a Whipple procedure are associated with high morbidity and mortality.
Firstly Valente et al[27]published a small series of three patients in which rescue endoscopic RFA for ampullary neoplasms with intraductal extension has been performed. They presented a long follow-up concluding that this approach may represent a safe alternative in patients refusing or not suitable for surgery. It could represent a long-term, palliative strategy in high risk patients.
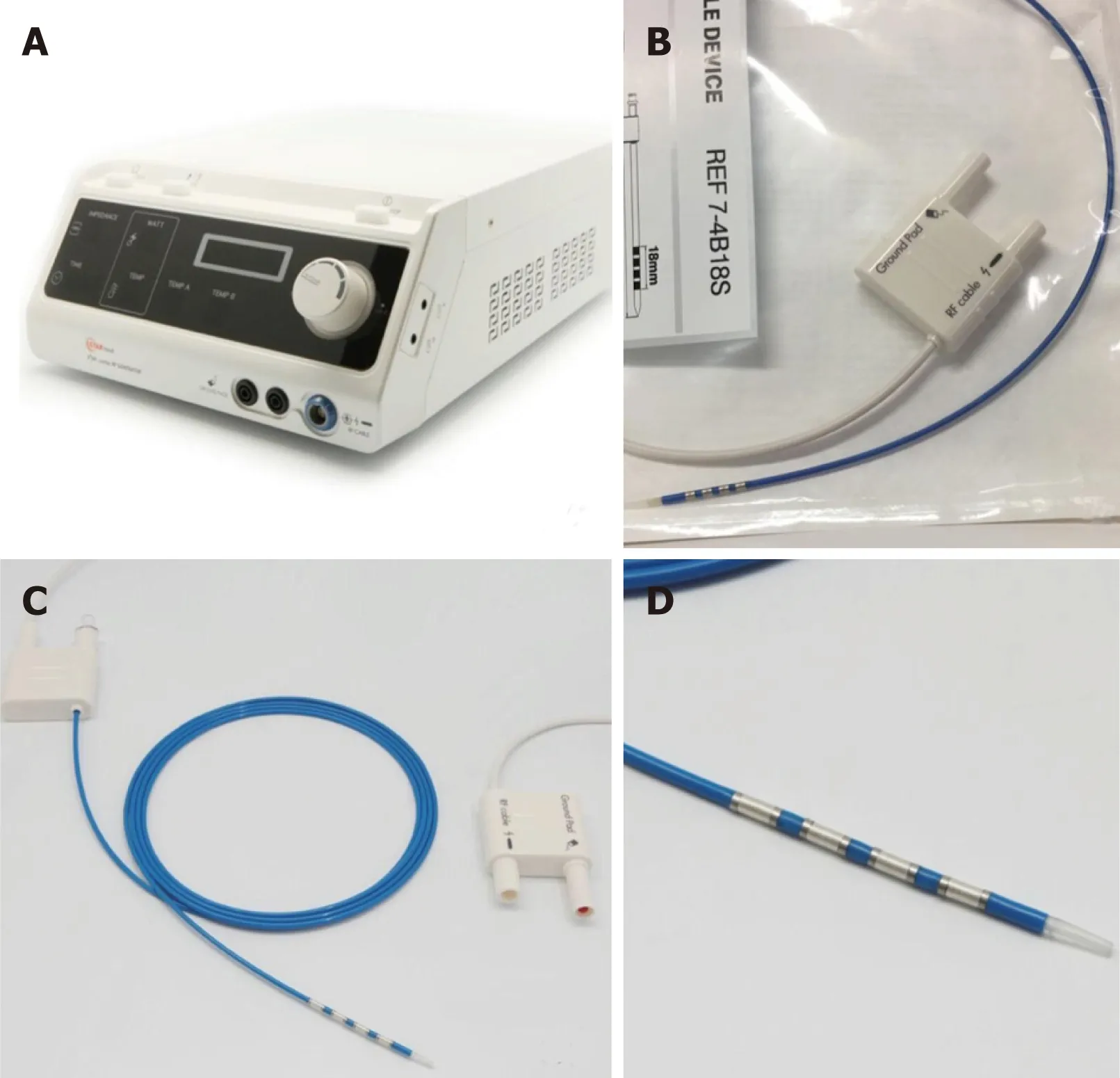
Figure 2 ELRA™ (EndoLuminal Radiofrequency Ablation, Taewoong Medical, South Korea). A: VIVA generator; B, C, D: ELRA™ catheter. Courtesy of Euromedical Srl.
A retrospective study evaluated the feasibility, safety, and efficacy in 14 patients with adenoma extension into the common bile duct and pancreatic duct. These patients underwent one RFA session (range, 1-5 sessions). At a median follow-up period of sixteen months after RFA, complete intraductal ablation was obtained in about 92% of patients. Adverse events occurred in 43% of cases, mainly represented by ductal strictures and a retro-duodenal abscess[28]. Suarez et al[29]published another small case series of 4 patients showing similar results, with 3 patients succeeding complete ablation of the intraductal adenoma and no adverse events noted during the short follow-up period.
Finally, Camus et al[30]published in 2018 the results of a prospective and open-label multicenter study including 20 patients with pathological confirmed endobiliary adenoma remnant undergoing intraductal RFA. Residual neoplasia was evident in 15% and 30% of patients at 6 mo and 12 mo, respectively, achieving seventy percent possibility of dysplasia eradication at 12 mo after a single session of RFA. At least one adverse event (no one severe) occurred in 40% patients during 12 mo follow-up.
Although small in number, in these studies RFA seems to be a reasonably safe and effective approach for the treatment of residual ampullary adenomas with endobiliary extension.
CONCLUSION
RFA is an additional treatment recently impemented to the advanced bilio-pancreatic endoscopy. In the field of unresectable neoplasia and MBO, in which treatment options are very restricted, great potential has been addressed to this procedure.Available studies suggest a beneficial effect on survival and stent patency with RFA,but current suggestion is limited because most of studies have been performed using a retrospective design, on diminutive and dissimilar cohorts of patients. As for complication, safety seems to be tolerable, though serious adverse events have been reported. Only few prospective studies and one randomized controlled trial are available and confirm and enhance these two main aspects: Increased survival and reduced rates of adverse events. Further efforts are needed to increase the degree of evidence and to comply with additional therapeutic indications such as occluded SEMS or adenomatous post-ampullectomy residuals.
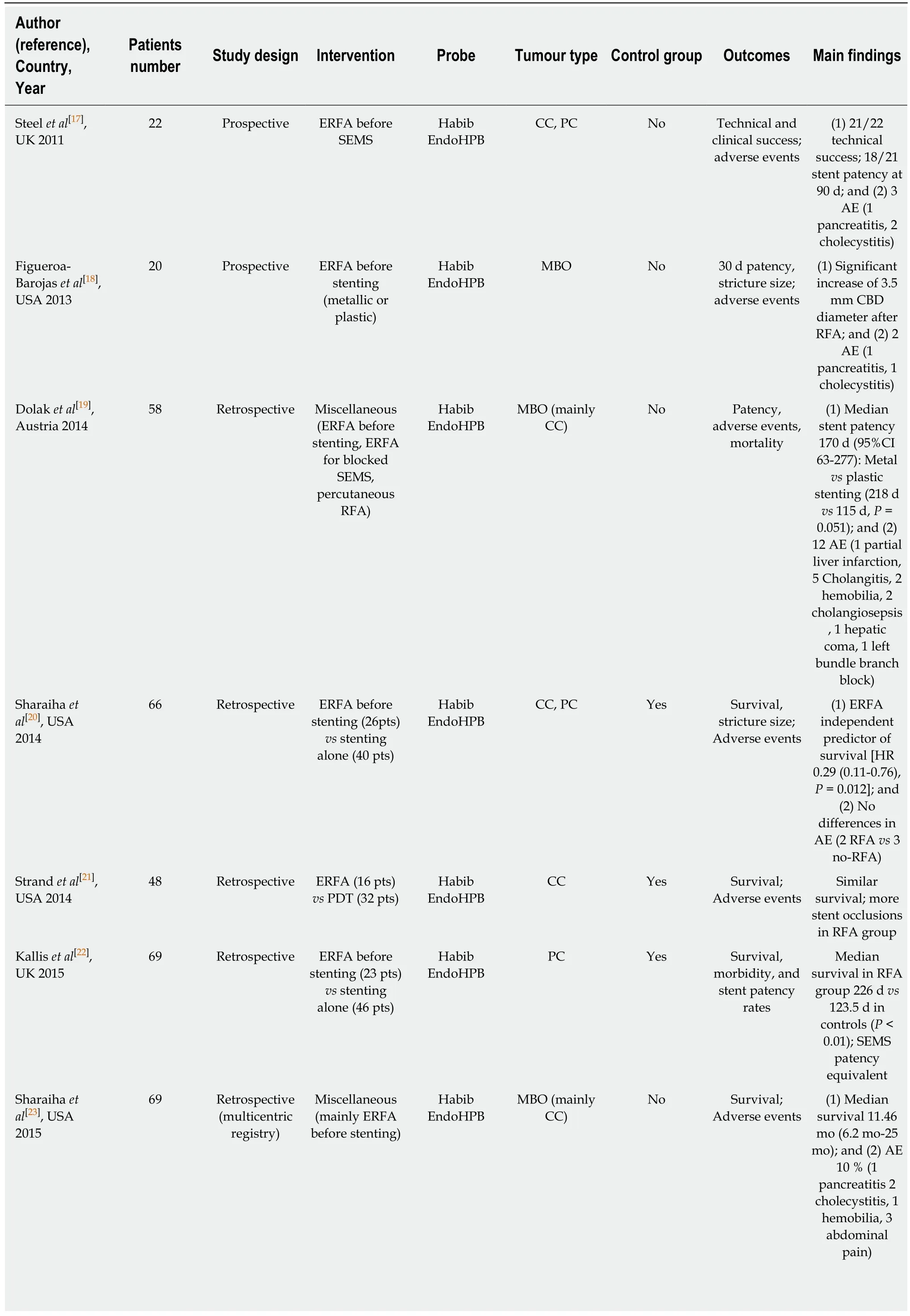
Table 1 Summary of the main characteristics of the included studies (study design, population, intervention, radiofrequency ablation probe, outcomes, main findings)
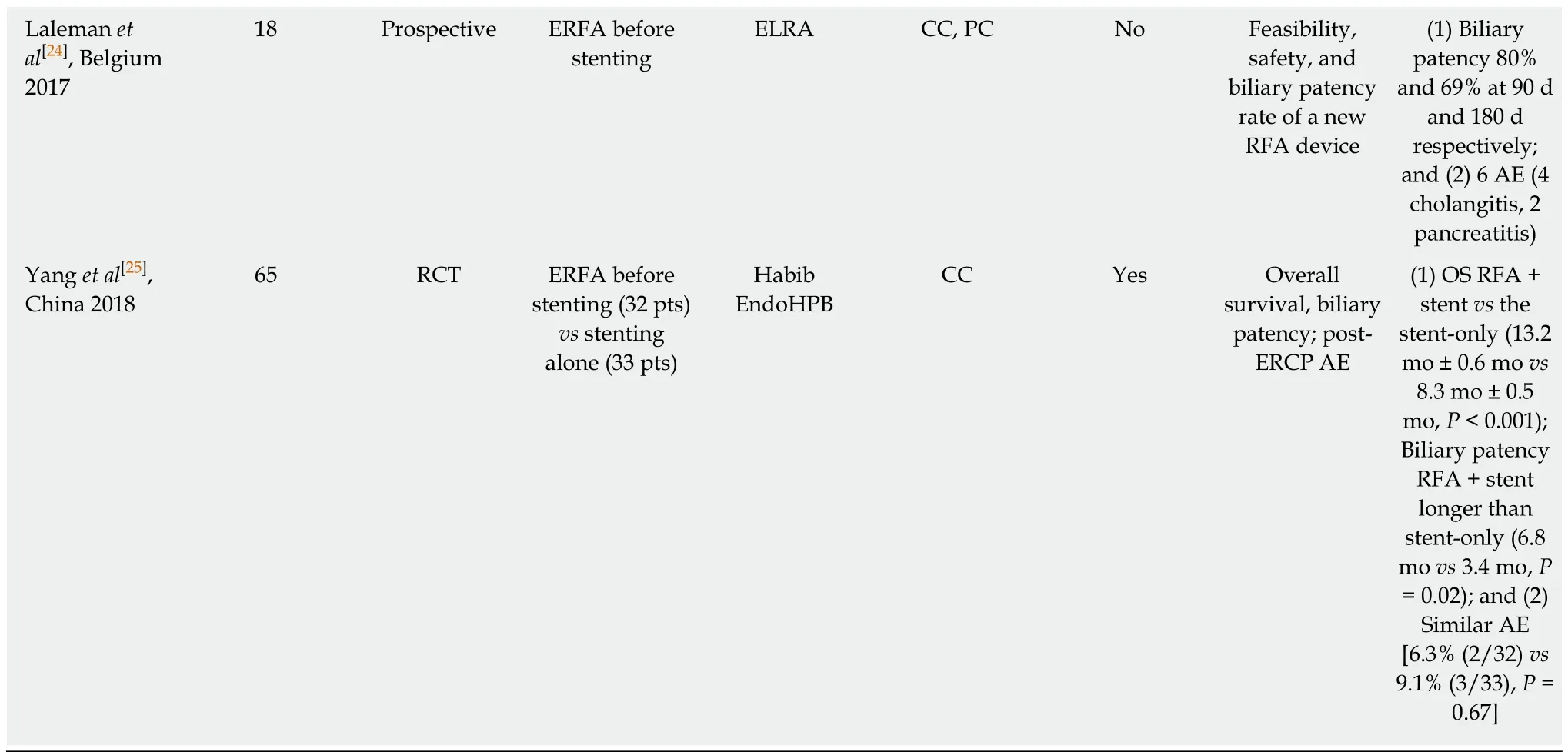
ERFA: Endoscopic radiofrequency ablation; CC: Cholangiocarcinoma; PC: Pancreatic cancer; MBO: Malignant biliary obstruction; SEMS: Self-expandable metal stents; AE: Adverse events; CBD: Common bile duct; HR: Hazard ratio; PDT: Photo dynamic therapy; OS: Overall survival.
杂志排行

World Journal of Gastrointestinal Endoscopy的其它文章
- Role of endoscopy in acute gastrointestinal bleeding in real clinical practice: An evidence-based review
- Role of endoscopy in the management of primary sclerosing cholangitis
- Endoscopic ultrasound-guided drainage of the biliary system:Techniques, indications and future perspectives
- Spectrum of gastrointestinal involvement in Stevens - Johnson syndrome
- No significant difference in clinically relevant findings between Pillcam® SB3 and Pillcam® SB2 capsules in a United States veteran population
- Age, socioeconomic features, and clinical factors predict receipt of endoscopic retrograde cholangiopancreatography in pancreatic cancer