No significant difference in clinically relevant findings between Pillcam® SB3 and Pillcam® SB2 capsules in a United States veteran population
2019-02-27TylerAasenDavidWilhoiteAynurRahmanKalpitDevaniMarkYoungJamesSwenson
Tyler D Aasen, David Wilhoite, Aynur Rahman, Kalpit Devani, Mark Young, James Swenson
Abstract BACKGROUND Capsule endoscopy (CE) allows for a non-invasive small bowel evaluation for a wide range of gastrointestinal (GI) symptoms and diseases. Capsule technology has been rapidly advancing over recent years, often improving image frequency and quality. The Pillcam® SB3 (SB3) capsule is one such technology that offers an adaptive frame rate advantage over the previous versions of the capsule the Pillcam® SB2 (SB2). Some have proposed that this improvement in capsule technology may lead to increased diagnostic yields; however, real world clinical data is currently lacking.AIM To evaluate the clinically relevant findings of SB3 and SB2 capsules in a population of United States veterans.METHODS A retrospective analysis of 260 consecutive CE studies was performed including 130 SB3 and 130 SB2 capsule studies. Recorded variables included: age, gender,type of capsule, body mass index, exam completion, inpatient status, opioid use,diabetes, quality of preparation, gastric transit time, small bowel transit time,indication, finding, and if the exam resulted in a change in clinical management.The primary outcome measured was the detection of clinically relevant findings between SB3 and SB2 capsules.RESULTS Mean age of the study population was 67.1 ± 10.4 years and 94.2% of patients were male. Of these 28.1% were on opioid users. The most common indications for capsule procedure were occult GI bleeding (74.6%) and overt GI bleeding(14.6%). Rates of incomplete exam were similar between SB3 and SB2 groups(16.9% vs 9.2%, P = 0.066). The overall rate of clinically relevant finding was 48.9% in our study. No significant difference was observed in SB3 vs SB2 capsules for clinically relevant findings (46.2% vs 51.5%, P = 0.385) or change in clinical management (40.8% vs 50.0%, P = 0.135).CONCLUSION Our study found no significant difference in clinically relevant findings between SB3 and SB2 capsules.
Key words: Capsule Endoscopy; Veterans; Retrospective studies; Capsules;Gastrointestinal diseases; SB3; SB2
INTRODUCTION
Capsule endoscopy (CE) offers a non-invasive form of small bowel evaluation for a variety of gastrointestinal (GI) symptoms and diseases[1,2]. Common indications for CE include the evaluation obscure GI bleeding, suspected or known Crohn's disease,surveillance of polyps or masses, and evaluation of suspect malabsorption syndromes[1,2]. Since the first wireless capsule was approved for use in 2001, multiple capsule enhancements and upgrades have been made in attempt to improve diagnostic accuracy and expand the clinical indications of CE[3,4].
Several commercial CE products are currently available and the preference of capsule often is determined by institutional policy and price; however, the Pillcam®SB3 (SB3) (Medtronic, Minneapolis, MN, United States) is currently one of the most widely used capsules[5]. Over time, advances in capsule technology have aimed to improve image capture quality, battery life, viewing angle, and rate of image capture[3-5]. In 2013, the SB3 capsule was introduced and it has largely replaced the previous version of the capsule Pillcam®SB2 (SB2) in clinical practice. The SB3 capsule offers an adaptive framerate technology which adjusts the image capture rate based on how fast the capsule is moving[6]. Additionally, in a clinical validation study,images from the SB3 capsule were rated superior to the SB2 capsule by physicians[7].Some have proposed that this improvement in capsule technology may lead to increased diagnostic yields; however, real world clinical data is currently lacking[8].Small studies evaluating diagnostic yields between SB3 and SB2 capsules have had mixed results, with some suggesting an improvement in diagnostic yield and others showing no benefit[9-11]. Additionally, limited data exists evaluating if capsule upgrades will alter clinical management. Data specific to the veteran population is particularly limited. This study aimed to evaluate the clinically relevant findings of SB3 and SB2 capsules in a population of United States veterans.
MATERIALS AND METHODS
Study population
This was a retrospective study conducted at the Mountain Home Veterans Affairs Medical Center after obtaining institutional review board approval. The study period included patients undergoing CE from January 2014 to January 2017. All patients undergoing CE during the study period were included. During the study period from January 2014 through December 2015, the SB2 capsule was being utilized at our institution while from December 2015 through January 2017 the SB3 capsule was being used. A total of 130 SB3 and 130 SB2 capsule studies were included. No studies were excluded. There was no financial support for this study.
Variables and outcomes
Charts were retrospectively accessed and pertinent demographic and study characteristics were recorded. Recorded patient demographics included age, gender,body mass index (BMI) and comorbidities such as history of diabetes and current opioid use. CE related variables such as indication, finding, exam completion,inpatient status, quality of preparation, gastric transit time (GTT), small bowel transit time (SBTT) were recorded. Incomplete CE examination was defined as the failure of the capsule to reach the cecum within the recording period of the study. Capsule retention was defined as evidence of capsule persistence within the body two weeks after capsule ingestions. Indications for the procedure were recorded as occult GI bleeding, overt GI bleeding, polyp or mass evaluation, inflammatory bowel disease,or other indication. Iron deficiency anemia and occult positive stool samples were included in the occult GI bleeding indication group. Clinically relevant capsule findings included the following categories: Evidence of inflammatory bowel disease,polyps/masses, and identification of a bleeding source. Findings of ulcerative disease,erosive disease, arteriovenous malformations, and gross blood in the lumen were considered positive for bleeding source identification. The primary outcome of the study was to evaluate clinically relevant findings in SB3 and SB2 capsule groups. The secondary outcome aimed to analyze if the capsule procedure resulted in a change in clinical management. A change in clinical management following the CE study was defined as those studies that lead to the ordering of an endoscopic procedure,ordering of a diagnostic study, or an addition or change of dose in the patient's medication regimen.
Capsule procedure
Standard preparation for CE at our institution included 2 liters of polyethylene glycol solution the evening before the procedure and 160 milligrams of simethicone one hour prior to capsule ingestion the morning of procedure. Patients were instructed to eat nothing by mouth starting midnight prior to procedure. After capsule ingestion patients could begin clear liquids two hours post ingestion and could eat a regular diet four hours after capsule ingestion. The capsule studies were read by gastroenterology fellows under the supervision of an experienced attending physician with expertise in CE. Studies were read using RAPID®Reader software. The preparation was considered to be inadequate if less than 50% of the small bowel was seen during the study.
Statistical analysis
Continuous variables were reported as means ± standard deviation. Categorical variables were reported as frequencies and their respective percentage. Unpaired ttest was used for normally distributed continuous variables and Mann-Whitney test for non-normally distributed continuous variables. For categorical variables, Pearson Chi Square was used or Fischer Exact Test when appropriate. Statistical significance was defined as two-tailed P value < 0.05. Statistical calculations were performed using GraphPad software under the guidance of a biostatistical expert.
RESULTS
Total of 260 patients undergoing consecutive CE studies were included during the study period. Of these, 130 patients utilized Pillcam®SB3 capsules and another 130 used Pillcam®SB2 capsules. Baseline characteristics of the patient population are as shown in Table 1. Overall mean age of the veterans included was 67.1 ± 10.4 years 94.2% of the patients were male. Mean BMI of the study population was 30.3 kg/m2,45.85% of patients were diabetic, and 28.1% were on opioid therapy. Incomplete capsule exams occurred in 13.1% of examinations, and inadequate preparation was seen in 12.7% of studies.
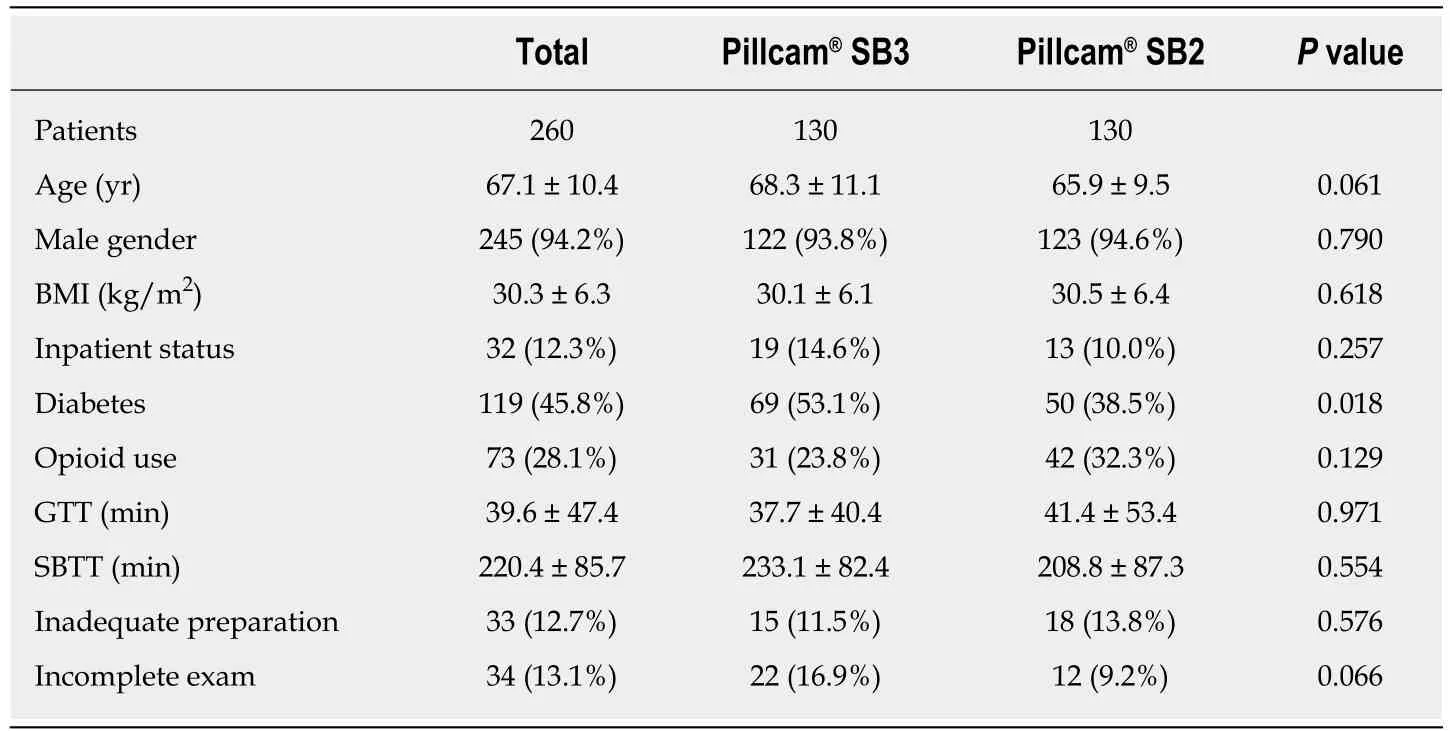
Table 1 Baseline demographics
No significant difference was observed in patient characteristics between SB3 and SB2 capsules for age, gender, BMI, opioid use, and inpatient status: Age (68.3 ± 11.1 vs 65.9 ± 9.5, P = 0.061), male gender (93.8% vs 94.6%, P = 0.790), BMI (30.1 ± 6.1 kg/m2vs 30.5 ± 6.4 kg/m2, P = 0.618), opioid use (23.8% vs 32.3%, P = 0.129), and inpatient status (14.6% vs 10% P = 0.257). A significant difference for diabetes as a comorbidity was seen between SB3 and SB2 groups (53.1% vs 38.5%, P = 0.018). There was also no significant difference in incomplete exam and inadequate preparation between SB3 and SB2 groups: Incomplete exam (16.9% vs 9.2% P = 0.066), inadequate preparation(11.5% vs 13.8%, P = 0.576). No capsule retentions were observed and no capsule malfunctions were seen within the cohort. Mean GTT was 39.6 ± 47.4 min and mean SBTT was 220.4 ± 85.7 min for the cohort. No significant difference in GTT or SBTT was observed between SB3 and SB2 capsule groups: GTT (37.7 ± 40.4 min vs 41.4 ±53.4 min, P = 0.971), SBTT (233.1 ± 82.4 min vs 208.8 ± 87.3 min, P = 0.554).
CE indications and findings are presented in Table 2. The most common indication for CE examination was occult GI bleeding (74.6%), followed by overt GI bleeding(14.6%), mass polyp evaluation (3.5%), inflammatory bowel disease (IBD) (2.7%), and other (4.6%). Other indications included diarrhea, celiac disease evaluation, and abdominal pain. Overall clinically relevant finding rate was 48.9% which included bleeding source identification (38.5%), mass/polyp (6.9%), and IBD (3.5%). No significant difference was observed in SB3 vs SB2 capsules for clinically relevant findings (46.2% vs 51.5%, P = 0.385). Additionally, 45.4% of CE studies resulted in a change in clinical management and no significant difference in changes in clinical management were seen between SB3 and SB2 capsule groups (40.8% vs 50.0%, P =0.135).
DISCUSSION
CE has now become a routine part of clinical practice for gastroenterologists and can be used as a non-invasive means to investigate a variety of GI symptoms[1,2]. Though many capsule enhancements have been made since CE was first introduced, there is limited data to suggest that recent improvements in capsule technology enhance diagnostic yield of the examinations. Our study demonstrated no significant difference in clinically relevant findings detected between SB3 and SB2 capsules. As a secondary outcome, we also found no significant difference for changes of clinical management between the two capsule groups. This study represents one of the largest studies to evaluate clinically relevant findings between SB3 and SB2 capsules, and to our knowledge is the largest that exclusively looks at a veteran population.
Over time, multiple enhancements in capsule technology have been made;however, a clear impact on improvements in capsule technology on key clinical endpoints has not clearly been demonstrated. Improving capsule viewing angle has been investigated, including one study that showed no significant difference in diagnostic yields between SB2 capsules and a 360° viewing capsules[12]. Alternatively,Rahman et al studied the effect of increasing capsule battery life on diagnostic yields of CE studies and found that the Pillcam®SB2-ex (SB2-ex), which increased battery life from eight hours to twelve hours, lead to higher study completion rates whencompared to SB2 capsules; however, no improvement in diagnostic yield was seen with the capsule upgrade and in fact the SB2 capsule outperformed the SB2-ex for diagnostic yields in this study[13]. Given these findings, some have suggested that improving battery life may not be the key to improving diagnostic yields[8].Alternatively, it was proposed that rapid transit times in the duodenum and jejunum may lead to missed lesions during CE; therefore, it was suggested that the adaptive frame rate of the SB3 capsule may enhance diagnostic yields[8]. The SB3 adaptive frame rate technology was designed to combat CE limitations during periods of rapid transit[6]. The SB3 capsules will perform a traditional image capture rate of two frames per second (FPS) during periods of slow transit, and image capture rates will automatically increase to six FPS during periods of rapid transit[6]. The SB3 capsule also offers superior image quality in comparison to the SB2 capsule and representative images from our cohort are presented in Figure 1[6].
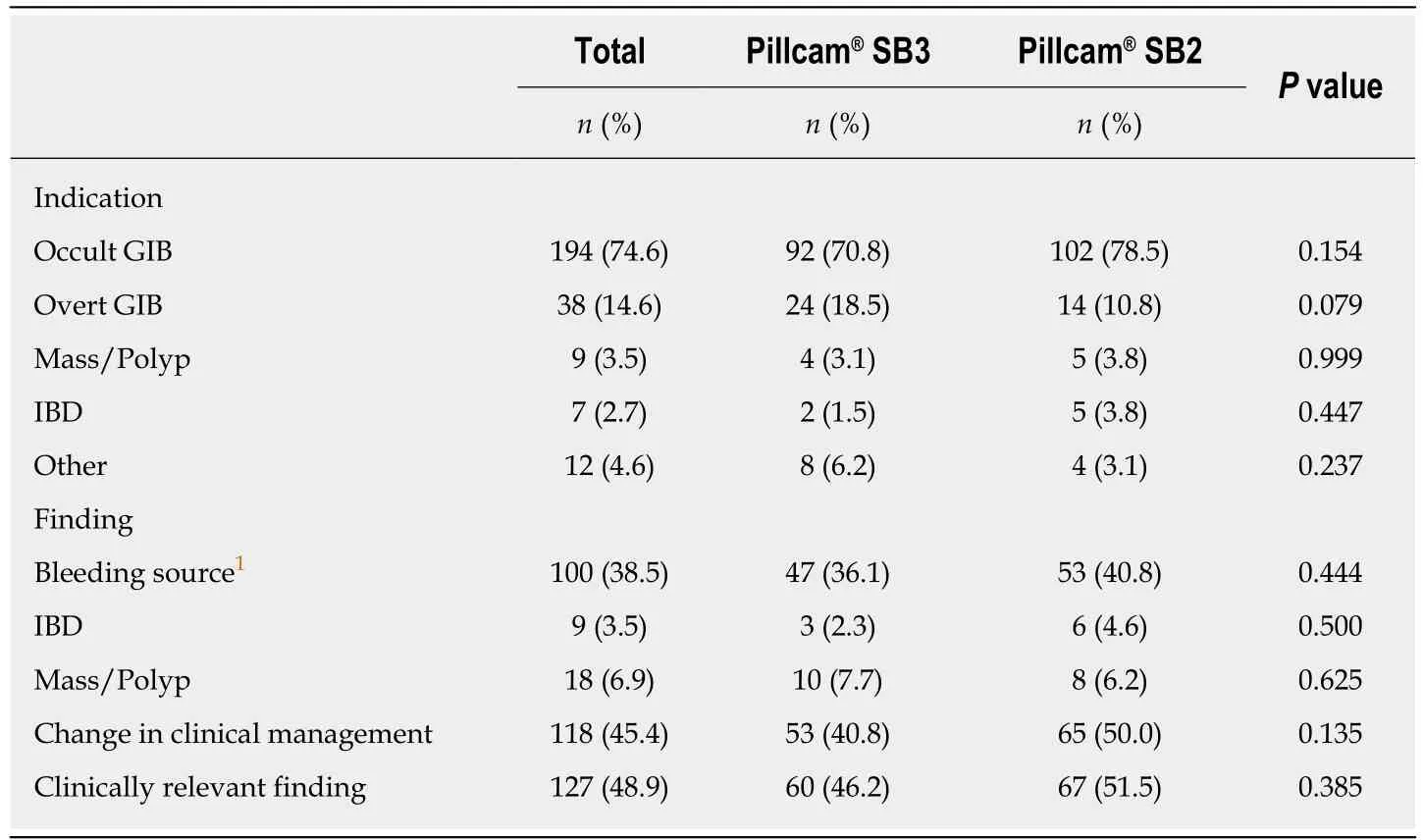
Table 2 Indications and findings of Pillcam® SB3 vs Pillcam® SB2 capsule studies
In theory, improving image quality and optimizing image capture rate may improve overall quality of CE examinations and improve its clinical usefulness. The SB3 capsule has been shown to provide improved image quality over the SB2 capsule and images were preferred by gastroenterologists in a feasibility study[7]. Whether this improvement in image quality along with the adaptive frame rate technology of the SB3 capsule results in improved diagnostic yields are more uncertain. Studies have previously aimed to evaluate if SB3 capsules lead to improved diagnostic yields in comparison to SB2 capsules, though most are retrospective in nature and come with significant limitations. Dunn et al[9]reported increased diagnostic yields of SB3 capsules in comparison to SB2 capsules; however, their study is limited by small sample size and is only published in abstract form. Monteiro et al[8]reported a possible increase in diagnostic yields in favor of SB3 capsules over SB2 capsules. Likewise, the study was limited to small retrospective cohort and major duodenal papilla detection rate was used as a surrogate indicator of diagnostic yield[8]. These data were further expanded upon by the same group and Xavier et al[10]subsequently published the largest retrospective series comparing diagnostic yields of SB3 and SB2 capsules and found no significant difference. More recently, Kunihara et al[14]reported that SB3 capsules improved the detection of small esophageal varices in comparison to SB2 capsules; however, overall rate of variceal detection was not significantly different between the two capsules. In our cohort, there was no significant difference of clinically relevant findings between SB3 and SB2 capsules. These results may also be supported by previous studies that failed to establish a significant effect on diagnostic yield by increasing the FPS from 2 FPS to 3 or 4 FPS[15,16].
CE continues to play a key role in clinical practice and CE studies often provide diagnostic information and impact clinical management. Prior investigations have suggested that diagnostic yields of CE may range from 39%-69% depending on procedure indications and definitions of pertinent findings[17-20]. The overall rate of clinically relevant finding in our study was 48.9% and no difference in clinically relevant findings was observed between SB3 and SB2 groups. CE has previously been shown to significantly impact clinical management of patients undergoing the investigation, with changes in clinical management reported ranging from 26%-67%[19-22]. Our study found that 45.4% of CE studies resulted in a change in clinical management, and there was no significant difference was observed between SB3 and SB2 groups. These findings may suggest that both capsules have a strong role in clinical practice.
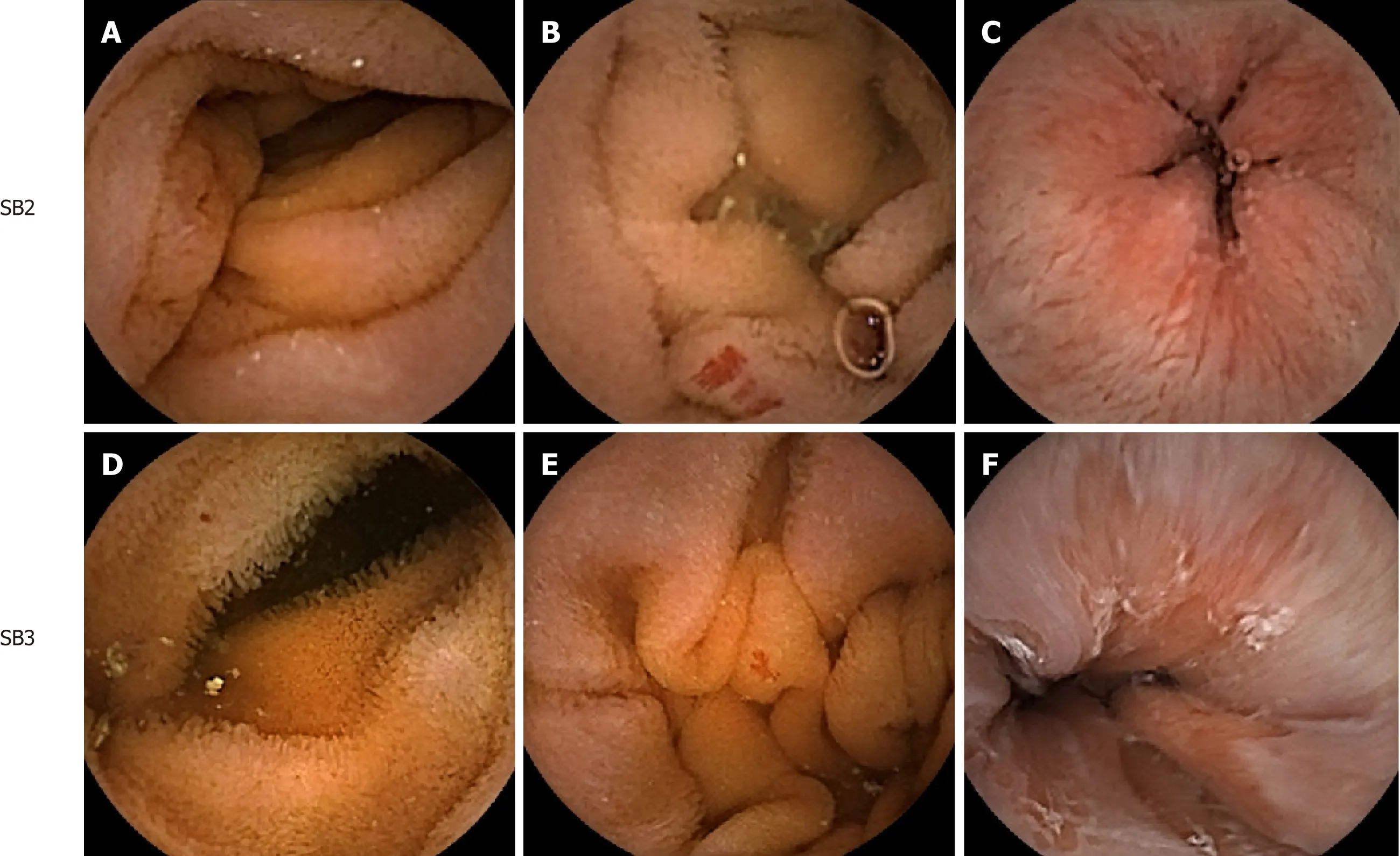
Figure 1 Image quality comparison between Pillcam® SB3 and Pillcam® SB2 capsules for selected clinical findings. A: Normal small intestinal lumen visualized with SB2 capsule; B: Vascular malformation visualized with SB2 capsule; C: Z-line visualized with SB2 capsule; D: Normal small intestinal lumen visualized with SB3 capsule; E: Vascular malformation visualized with SB3 capsule; F: Z-line visualized with SB3 capsule.
Our study, like others investigating this topic, is limited by the retrospective study design. Additionally, our study examined a unique population of United States veterans and may not be directly comparable to other studies investigating this area.The cohort in our study was almost entirely male (94.2%) which reflects the overall demographics of our institution. Data regarding the diagnostic yields of CE in the veteran population is extremely limited, though one study reported higher than average diagnostic yields in the veteran population[23]. The most common indication in our study was occult GI bleeding (74.6%), which represents a larger portion of studies for this indication than large CE cohorts have previously suggested[18,24]. This is likely explained by a below average use of CE for crohn's disease evaluation and management at our institution. Our study included consecutive endoscopy examinations before and after SB3 capsules became the standard capsule at our institution. Although no significant changes in how capsules were read at our institution were made during this time, it is difficult to control for variations and changes in practice patterns over time or any learning curves when the new capsule was implemented. Our CE studies were also read by trainees under the supervision of experienced providers which may introduce inter-observer variability; however, this method of reading may be reflective of real-world clinic practice. Group characteristics between SB3 and SB2 groups in our study were mostly similar,however the SB3 group had an overall higher age and great portion of patients with diabetes which previous studies have shown may potentially increase CE findings or lead to prolonged transit times[25-27]. Diabetes has been shown to be a risk factor for poor colon preparations, though the effects of diabetes on CE preparation are poorly characterized[28]. Likewise, our study included a large percentage of current opioid users at 28.1%; however opioid use has not clearly been shown to be associated with altered exam completion rates or diagnostic findings[29,30].
The failure of our study to show a significant improvement in clinically relevant findings between SB3 and SB2 capsules may potentially suggest that there is a plateau of diagnostic yield during CE studies. There is a possibility that the adaptive frame rate technology of the SB3 capsule may lead to the detection of non-clinically relevant findings, or that the improved image quality of this capsule may lead to better visualization of lesions that would have still been detected by previous capsule versions. If a diagnostic yield plateau was exist, then potential cost savings may be created by using the most affordable capsule option under most circumstances.However, it remains to be seen if better capsule technology may result in improved diagnostic yields within particular subgroups of study indications; therefore, studies evaluating SB3 vs SB2 capsules or other similar improvements in capsule technology for more specific procedural indications may better elucidate if capsule enhancements would improve clinically relevant findings within these groups. Additionally, future investigation to evaluate the effect of capsule enhancement on diagnostic yield will be warranted. The principle indications for CE procedures in our study were primarily overt and occult GI bleeding. Future direction of research may seek to explore only these indications, and a post hoc analysis including only these principle indications may be beneficial to confirm the results obtained by the same total group. Likewise,studies investigating findings for procedures with the specific indication of IBD,polyp or mass evaluation, or other indications may be required to further evaluate the effect of capsule upgrades within these groups.
In conclusion, our study found no significant difference in clinically relevant findings between SB3 and SB2 capsules. Additionally, no significant change in clinical management was observed. Further prospective randomized research is needed to determine if this capsule improvement enhances clinical findings or impacts clinical management.
ARTICLE HIGHLIGHTS
Research background
Capsule endoscopy (CE) is frequently used in clinical practice to evaluate a wide spectrum of gastrointestinal symptoms and diseases. Capsule technology has advanced over time; however,it remains unclear if upgrades in capsule technology enhance clinically relevant findings during the procedure.
Research motivation
The Pillcam®SB3 capsule is a commonly used capsule that provides superior image quality and an adaptive frame rate advantage over the previous versions of the capsule the Pillcam®SB2. It has been proposed that these improvements may result in improved diagnostic yields of the CE study.
Research objectives
To assess clinically relevant findings of SB3 and SB2 capsules in a population of United States veterans.
Research methods
A retrospective analysis of 260 consecutive CE studies was performed including 130 SB3 and 130 SB2 capsule studies. The primary outcome measured was the detection of clinically relevant findings between SB3 and SB2 capsules. Whether the capsule study resulted in a change in clinical management was evaluated as a secondary measure.
Research results
The overall rate of clinically relevant finding was 48.9% in our study. No significant difference was observed in SB3 vs SB2 capsules for clinically relevant findings (46.2% vs 51.5%, P = 0.385)or change in clinical management (40.8% vs 50.0%, P = 0.135).
Research conclusions
Our study found no significant difference in clinically relevant findings between SB3 and SB2 capsules.
Research perspectives
Improvements in capsule technology should be critically analyzed to determine their impact on clinical practice. Further prospective research is warranted to confirm the results of our study.
杂志排行

World Journal of Gastrointestinal Endoscopy的其它文章
- Safety and efficacy of over-the-scope clip-assisted full thickness resection of duodenal subepithelial tumors: A case report
- Role of pancreatoscopy in management of pancreatic disease: A systematic review
- Narrow band imaging evaluation of duodenal villi in patients with and without celiac disease: A prospective study
- Age, socioeconomic features, and clinical factors predict receipt of endoscopic retrograde cholangiopancreatography in pancreatic cancer
- Spectrum of gastrointestinal involvement in Stevens - Johnson syndrome
- Endoscopic ultrasound-guided drainage of the biliary system:Techniques, indications and future perspectives