Age, socioeconomic features, and clinical factors predict receipt of endoscopic retrograde cholangiopancreatography in pancreatic cancer
2019-02-27SheilaRustgiSunilAminMichelleKimSatishNagulaNikhilKumtaChristopherDiMaioPaoloBoffettaAimeeLucas
Sheila D Rustgi, Sunil P Amin, Michelle K Kim, Satish Nagula, Nikhil A Kumta, Christopher J DiMaio,Paolo Boffetta, Aimee L Lucas
Abstract BACKGROUND Endoscopic retrograde cholangiopancreatography (ERCP) is the recommended technique for biliary decompression in pancreatic cancer. Previous studies have suggested racial, socioeconomic and geographic differences in diagnosis,treatment and outcomes of pancreatic cancer patients.AIM To examine geographic, racial, socioeconomic and clinical factors associated with utilization of ERCP.METHODS Surveillance, Epidemiology and End Results and linked Medicare claims data were used to identify pancreatic cancer patients between 2000-2011. Claims data were used to identify patients who had ERCP and other treatments. The primary outcome was receipt of ERCP. Chi-squared analyses were used to compare demographic information. Trends in use of ERCP over time were assessed using Cochran Armitage test. Adjusted odds ratios (aORs) and 95% confidence intervals (CIs) for receipt ERCP were calculated using logistic regression,controlling for other characteristics.RESULTS Among 32510 pancreatic cancer patients, 14704 (45.2%) underwent ERCP.Patients who had cancer located in the head of the pancreas (aOR 3.27, 95%CI:2.99-3.57), had jaundice (aOR 7.59, 95%CI: 7.06-8.17), cholangitis (aOR 4.22,95%CI: 3.71-4.81) or pruritus (aOR 1.42, 95%CI: 1.22-1.66) and lived in lower education zip codes (aOR 1.14, 95%CI: 1.04-1.24) were more likely to receive ERCP. In contrast, patients who were older (aOR 0.88, 95%CI: 0.83, 0.94), not married (aOR 0.92, 95%CI: 0.86, 0.98), and lived in a non-metropolitan area (aOR 0.89, 95%CI: 0.82, 0.98) were less likely to receive ERCP. Compared to white patients, non-white/non-black patients (aOR 0.83, 95%CI: 0.70-0.97) were less likely to receive ERCP. Patients diagnosed later in the study period were less likely to receive ERCP (aOR 2004-2007 0.85, 95%CI: 0.78-0.92; aOR 2008-2011 0.76,95%CI: 0.70-0.83). After stratifying by indications for ERCP including jaundice,racial differences persisted (aOR black patients 0.80, 95%CI: 0.67-0.95,nonwhite/nonblack patients 0.73, 95%CI: 0.58-0.91). Among patients with jaundice, those who underwent surgery were less likely to undergo ERCP (aOR 0.60, 95%CI: 0.52, 0.69).CONCLUSION ERCP utilization in pancreatic cancer varies based on patient age, marital status,and factors related to where the patient lives. Further studies are needed to guide appropriate biliary intervention for these patients.
Key words: Pancreatic cancer; Endoscopic retrograde cholangiopancreatography;Socioeconomic disparities; Racial disparities; Jaundice; Outcomes research
INTRODUCTION
Pancreatic cancer is the fourth most common cause of cancer death in the United States[1]. Endoscopic retrograde cholangiopancreatography (ERCP), especially prior to widespread use of endoscopic ultrasound (EUS), served both diagnostic and therapeutic roles in the evaluation and management of pancreatic cancer[2,3]. ERCP is recommended to relieve biliary obstruction in pancreatic cancer[3,4].
Although pancreatic cancer outcomes are poor for the general population, several studies have shown that racial and sociodemographic factors impact use of treatment and overall survival[5-12]. A recent retrospective study of the Surveillance,Epidemiology and End Results (SEER)-Medicare population found that sociodemographic factors were associated with receipt of pancreatic cancer-directed surgery, but that only geographic location was independently associated with survival[13]. Other studies suggest black patients fare worse than white patients in both utilization of pancreatic cancer treatment modalities and survival[7,10-12].
Since previous studies have demonstrated racial, socioeconomic, geographic and clinical disparities in pancreatic cancer-directed surgery, chemotherapy and radiation,we hypothesized similar variations may be seen in the use of ERCP. The aim of this study is to evaluate racial, socioeconomic, geographic and clinical factors associated with use of ERCP among patients with pancreatic cancer. A secondary outcome was receipt of ERCP in the setting of jaundice, cholangitis or pruritus.
MATERIALS AND METHODS
Patient selection and treatment
The SEER database of the National Cancer Institute is a national registry of patients diagnosed with cancer that collects data on cancer incidence and survival[14]. This database is linked with the patient's Medicare claims from time of Medicare eligibility until death. The claims were used to identify patients' clinical and procedural data.Patients in this study population are aged 65 and older because this is the age of enrollment in Medicare coverage in the United States. Patients with secondary insurance were excluded so that all claims were captured in this dataset. Patients with primary pancreatic cancer diagnosed between 2000 and 2011 were identified; those patients with more than one primary cancer were excluded to eliminate the effect of other cancers on morbidity and mortality[15].
Sociodemographic information was obtained from both the SEER and Medicarelinked databases. Comorbid conditions were controlled for using the Deyo adaption of the Charlson co-morbidity index[16-18]. Both inpatient and outpatient hospital claims(Medicare Provider Analysis and Review, Outpatient Standard Analytical File) as well as diagnoses on claims submitted by individual physicians (Carrier file) were included[18,19].
Education and income information was obtained from census data. Patients' zip codes were cross-referenced with census data to obtain median incomes for the zip code. Similarly, zip codes and census data were used to identify the proportion of residents in the zip code who had not completed high school, graduated from high school, attained some college and graduated from college. Patient level income and education data are not available.
ERCP, surgery, chemotherapy, radiation, jaundice, pruritus and cholangitis were identified from claims data using International Classification of Disease, 9thEdition and Healthcare Common Procedure Coding System codes (Table 1)[20-23]. SEERMedicare claims have been shown to accurately capture patients who have been treated with chemotherapy[23]. SEER historic stage was used for patient stage because American Joint Committee on Cancer stage was only available from 2004 to 2011.Patients of all stages were included in this analysis because all of these patients are evaluated for and receive these procedures.
Statistical analysis
Categorical variables were compared using chi-squared analyses to test for associations between patients' racial, socioeconomic, geographic and clinical characteristics and use ERCP. Statistical significance was noted as P value < 0.05.Trends in use of ERCP over time were assessed using Cochran Armitage test.Adjusted odds ratios and 95% confidence intervals (CIs) for receipt ERCP were calculated using logistic regression, controlling for other characteristics, including age,race, marital status, education, income, metropolitan area, region of the United States,symptoms and conditions, Charlson comorbidity scores, cancer site, stage and use of other therapies including surgery, chemotherapy and radiation. All statistical analyses were performed using SAS 9.3 and 9.4 (Cary, NC). The study was approved by both the local Institutional Review Board and the National Cancer Institute.
RESULTS
Between 2000 and 2011, a total of 32510 patients were diagnosed with pancreatic cancer and met inclusion criteria (Figure 1 and Table 2). Among these patients, 14704(45.2%) underwent ERCP. Patients who underwent ERCP were more often younger(46.9% vs 43.9%, P < 0.01), married (46.3% vs 44.2%, P < 0.01), and white (45.8% white vs 42.3% of black patients vs 42.7% of non-white/non-black patients, P < 0.01) (Table 2). ERCP was used less often later in the study period (Table 3, Cochran-Armitage trend P < 0.01). More patients in the Northeast underwent ERCP (46.5%) compared to Southeast (45.4%), Midwest (43.3%) or West Coast (45.1%), P < 0.01 (Table 2). More patients with jaundice (78.1%), cholangitis (87.4%) and pruritus (70.8%) underwent ERCP than those without these symptoms, P for all < 0.01. Patients who underwent other cancer directed therapies including chemotherapy, radiation and surgery also received ERCP more often.
To better assess the differences in receipt of ERCP, logistic regression was used to evaluate the impact of race, sociodemographic and clinical factors (Table 4). Patientswho were older (aOR 0.88, 95%CI: 0.82-0.95), not married (aOR 0.90, 95%CI: 0.85-0.97),or lived in a non-metropolitan area (aOR 0.87, 95%CI: 0.79-0.97) were less likely to receive ERCP. Compared to white patients, non-white/non-black patients (aOR 0.83,95%CI: 0.70-0.97) were less likely to receive ERCP.
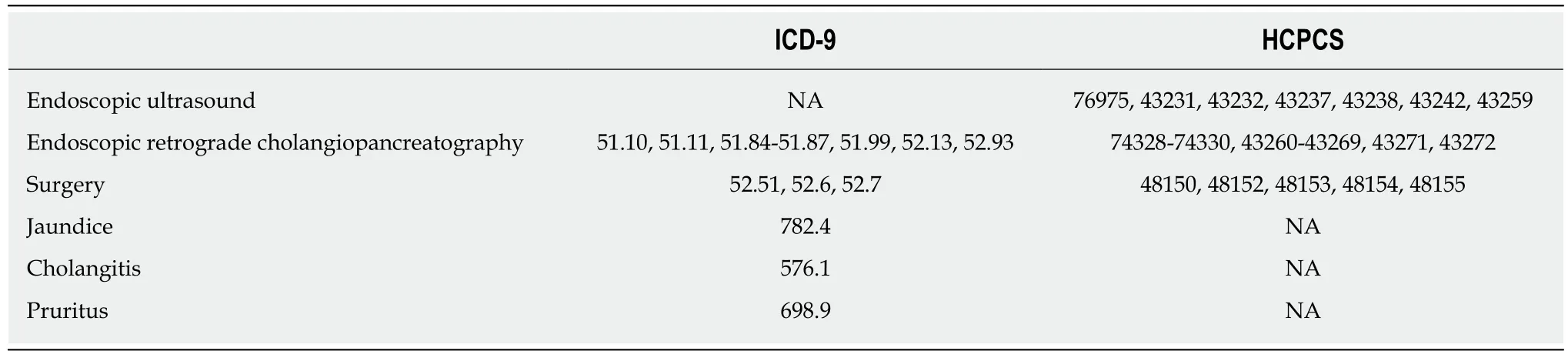
Table 1 International Classification of Disease, 9th Edition and Healthcare Common Procedure Coding System codes for claims data
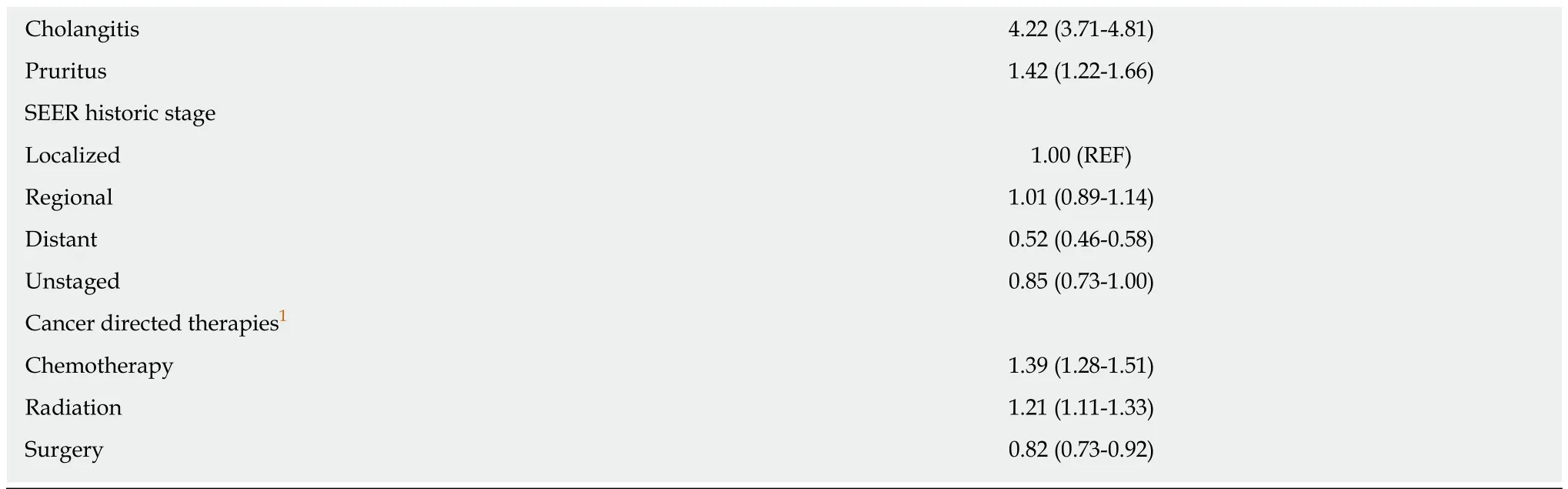
Clinical factors including cancer site, stage of cancer and use of other therapies were also associated with receipt of ERCP. Patients with cancer originating in the head of the pancreas had greater odds of receiving ERCP (aOR 3.27, 95%CI: 2.99-3.57)(Table 4). Compared to those with localized disease, patients with distant disease were less likely to receive ERCP (OR 0.52, 95%CI: 0.46-0.58). Finally, those who received chemotherapy (aOR for 1.39, 95%CI: 1.28-1.51) and radiation (aOR 1.21,95%CI: 1.11-1.33) had increased odds of receiving ERCP. Those who underwent surgery were less likely to receive ERCP (aOR 0.82, 95%CI: 0.73-0.92). Charlson score did not impact receipt of ERCP.
ERCP may not always be indicated in pancreatic cancer, and receipt of biliary decompression may not always suggest appropriate management. To address this, we performed a stratified analysis for receipt of ERCP in the setting of jaundice,cholangitis and pruritus (Table 5). After stratifying by indications for ERCP, racial differences became apparent. Compared to white patients, black patients (aOR 0.80,95%CI: 0.67-0.95) and non-white/non-black (aOR 0.73, 95%CI: 0.58-0.91) were less likely to undergo ERCP in the presence of jaundice (Table 5). Among patients with jaundice, patients who underwent surgery were less likely to undergo ERCP (aOR 0.60, 95%CI: 0.52-0.69).
The use of ERCP decreased over time: 4955 (47.7%) of patients received ERCP in 2000-2003, 4949 (44.5%) in 2004-2007, and 4800 (43.7%) in 2008-2011 (P-value for trend< 0.05, Table 3). Compared to those diagnosed early in the study, patients diagnosed in 2008-2011 were less likely to undergo ERCP (aOR 0.90, 95%CI: 0.83-0.97) (Table 4).
DISCUSSION
To our knowledge, this is the first study to evaluate race, income, education,geographic location and other clinical and sociodemographic characteristics in receipt ERCP in pancreatic cancer. While not curative, endoscopic procedures aid with diagnosis and staging, alleviate morbidity and facilitate other curative treatments including surgery and chemotherapy[3]. Given the dismal prognosis associated with pancreatic cancer, it is important to ensure that all patients have access to procedures that can aid in diagnosis, staging and management to reduce disparities in outcomes.
While other analyses have focused on racial disparities in PC, our study is unique in its ability to capture other sociodemographic data, such as income and education[5-10,13,24,25]. When controlling for these factors, we found no differences in overall receipt of ERCP for black patients. In our analyses stratified by ERCP indications, black patients received ERCP less often for jaundice, but not cholangitis or pruritus. In contrast, non-white/non-black patients received ERCP less often for the indications of jaundice and cholangitis, but not pruritus. Given the relatively small number of patients with pruritus (n = 146 for black patients and n = 120 for nonblack/non-white patients), it is possible the sample is not sufficient to detect differences in use of ERCP for pruritic patients. Further studies are warranted to investigate these racial discrepancies.
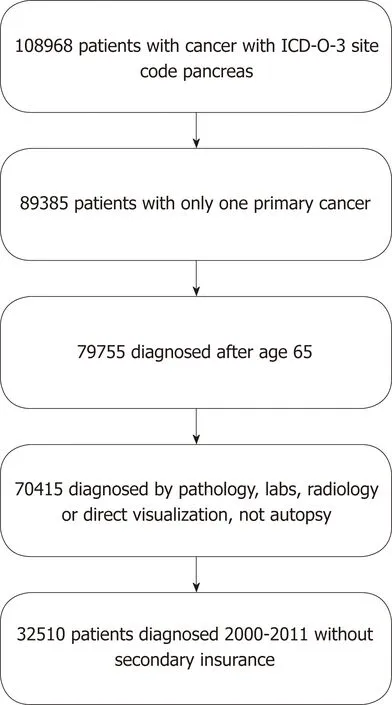
Figure 1 Patient selection.
Interestingly, patient age, marital status, and factors related to where the patient lives, including metropolitan area, were also associated with receipt of ERCP in pancreatic cancer. The relationship between surgical resection and sociodemographic factors including younger age and being married has previously been shown; our findings suggest the same is true for ERCP[13]. Differences in utilization may be explained by access to experts available to perform these procedures and regional practice differences. It should be noted that geographic differences shown in this study may not be representative of all regions in the country, since the SEER registry includes a selected 19 urban and rural regions throughout the United States. The Charlson score was not associated with use of ERCP, suggesting patient comorbidities do not deter endoscopists from pursuing these procedures.
The use of ERCP in pancreatic cancer patients fell during this time period. This may reflect two trends: One is the use of EUS for diagnosis and staging generally supplanted ERCP during this time[3]. The second may have been a large randomized controlled trial that suggested that ERCP performed prior to surgical resection increased postoperative complications and surgical morbidity[26]. Both trends may have had an effect of decreasing the use of ERCP in pancreatic cancer.
Patients with advanced stage disease received ERCP less often than those without metastatic disease. These findings may be expected in patients pursuing palliative options or who chose to forego further diagnostic work up and treatment. In contrast,patients with regional disease were more likely to pursue ERCP, which may be consistent with a plan of care to pursue cure with other cancer directed therapies[27].Multivariable analysis also showed that those who received chemotherapy and radiation were more likely to receive ERCP. ERCP can facilitate these treatments through biliary decompression and normalization of bilirubin. In contrast patients who underwent surgery were less likely to receive ERCP. During this time period,studies suggested that preoperative ERCP may increase postoperative complications,which may have impacted practice patterns[21,26].
There are several limitations to this study. There is variation in use of ERCP for malignant obstruction which may be guided by physician preference or protocols at different centers, which could not be measured through this database[28]. The use of ERCP in pancreatic cancer patients with resectable disease is controversial[29].Additionally, receipt of ERCP in pancreatic cancer may not accurately reflect access to expert care or appropriate clinical care. To address this, we performed additional analyses stratified by clinical indications (jaundice, cholangitis and pruritus) for ERCP. Racial, socioeconomic and geographic disparities identified here point to the need for future studies on how best to use ERCP in the management of PC as well as how to ensure that all patients have access to high quality care.
This is an analysis of a retrospective claims database and therefore patients are not randomized. However, our goal with this study was to examine how care is delivered in the real world. As with any claims database the information are limited toprocedures and diagnoses as submitted by physicians. Previous studies suggest the accuracy of procedure coding (e.g., for endoscopy and surgery) is high[30-32]. However,important clinical information that impacts recommendations for surgery and procedures, including smoking status and laboratory values (e.g., bilirubin level,carcinoembryonic antigen, cancer antigen 19-9), is not available.
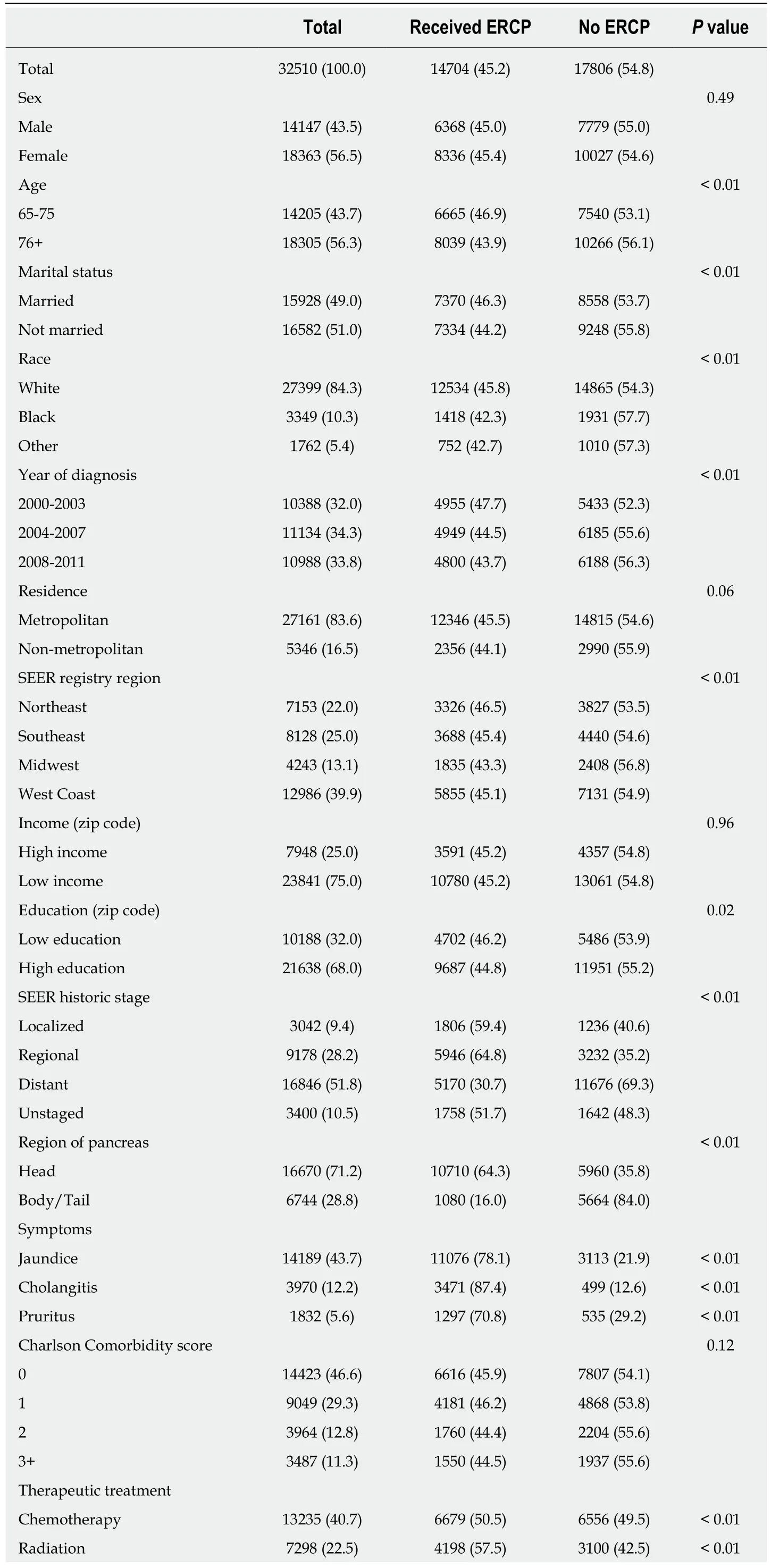
Table 2 Characteristics of patients with pancreatic cancer by receipt of endoscopic retrograde cholangiopancreatography n (%)

Some lines do not sum to 100% due to rounding or missing data. Other race: Neither white nor black race.Not married includes single, divorced and widowed. Metropolitan area defined as counties in metropolitan areas with population of 250000 or more; urban area defined as counties with populations of 2500 or more,both adjacent to metropolitan areas and not adjacent to metropolitan areas; rural defined as counties either completely rural or with populations < 2500. High income defined as > 75th percentile of income, or $74147.Low income defined as < 75th percentile or $74147. High education defined as living in a zip code where >50% of the population has completed some college or more. Low education is defined as living in a zip code where > 50% of the population has no college education. ERCP: Endoscopic retrograde cholangiopancreatography; SEER: Surveillance, Epidemiology and End Results.
Despite these limitations, this is the first study of a large population dataset that describes racial, sociodemographic and geographic disparities in use of ERCP for patients with pancreatic cancer. Since appropriate staging and prompt referral for surgery is crucial for potential of cure for these patients, it is possible that differences in the use of endoscopic procedures may partially explain previously described racial disparities in survival as well. ERCP utilization in pancreatic cancer varies based on patient age, marital status, and factors related to where the patient lives. Further studies are needed to guide appropriate biliary intervention for these patients.

Table 3 Use of endoscopic retrograde cholangiopancreatography over time using Cochran Armitage trend n (%)
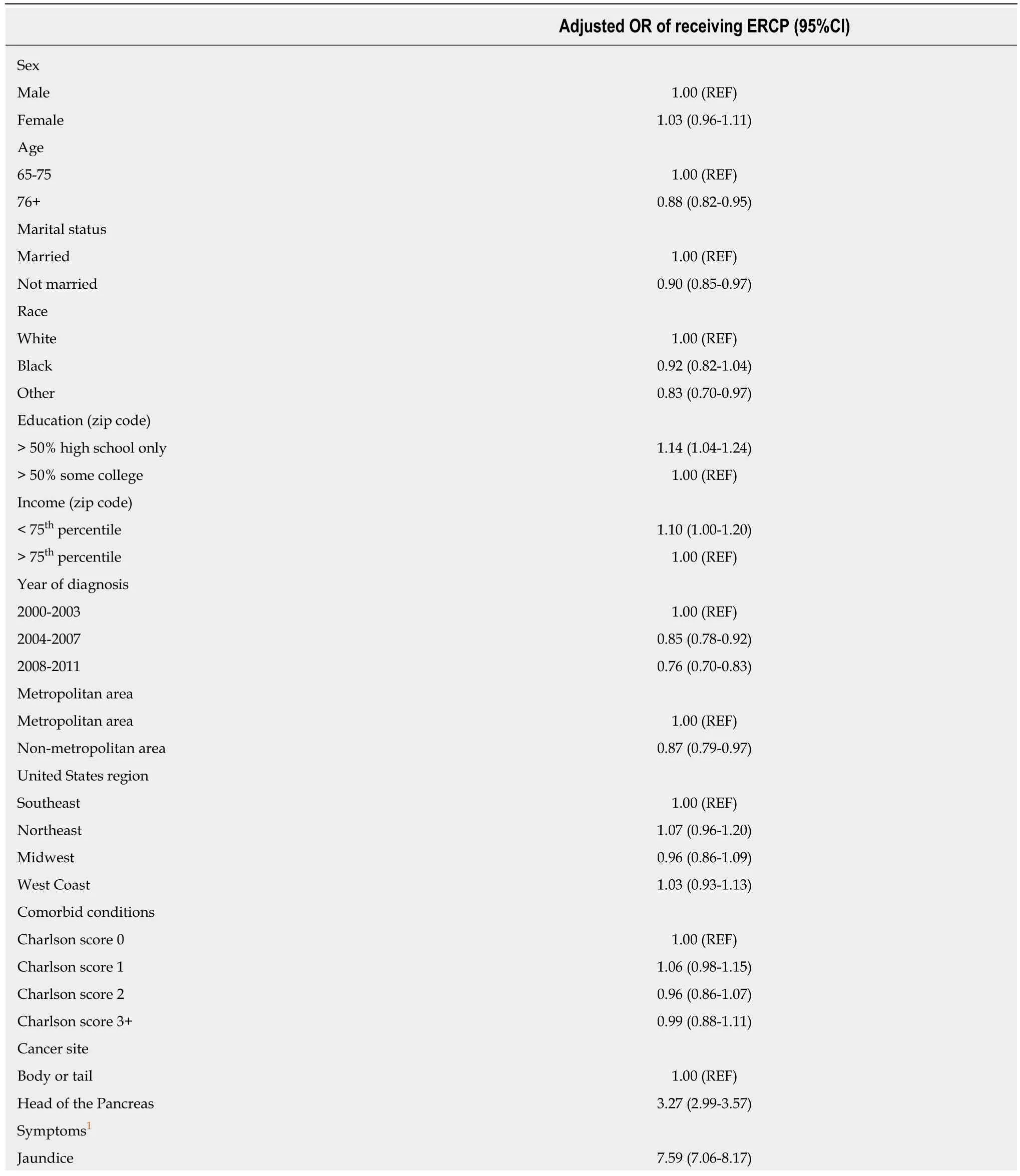
Table 4 Multivariable analysis of use of endoscopic retrograde cholangiopancreatography
1Referent category is not having those symptoms, conditions or treatments. Other race is neither white nor black race. Not married includes single,divorced and widowed. Metropolitan area defined as counties in metropolitan areas with population of 250000 or more. High income defined as > 75th percentile of income, or $74147. Low income defined as < 75th percentile or $74147. High education defined as living in a zip code where > 50% of the population has completed some college or more. Low education is defined as living in a zip code where > 50% of the population has no college education.OR: Odds ratio; CI: Confidence interval; Endoscopic retrograde cholangiopancreatography.
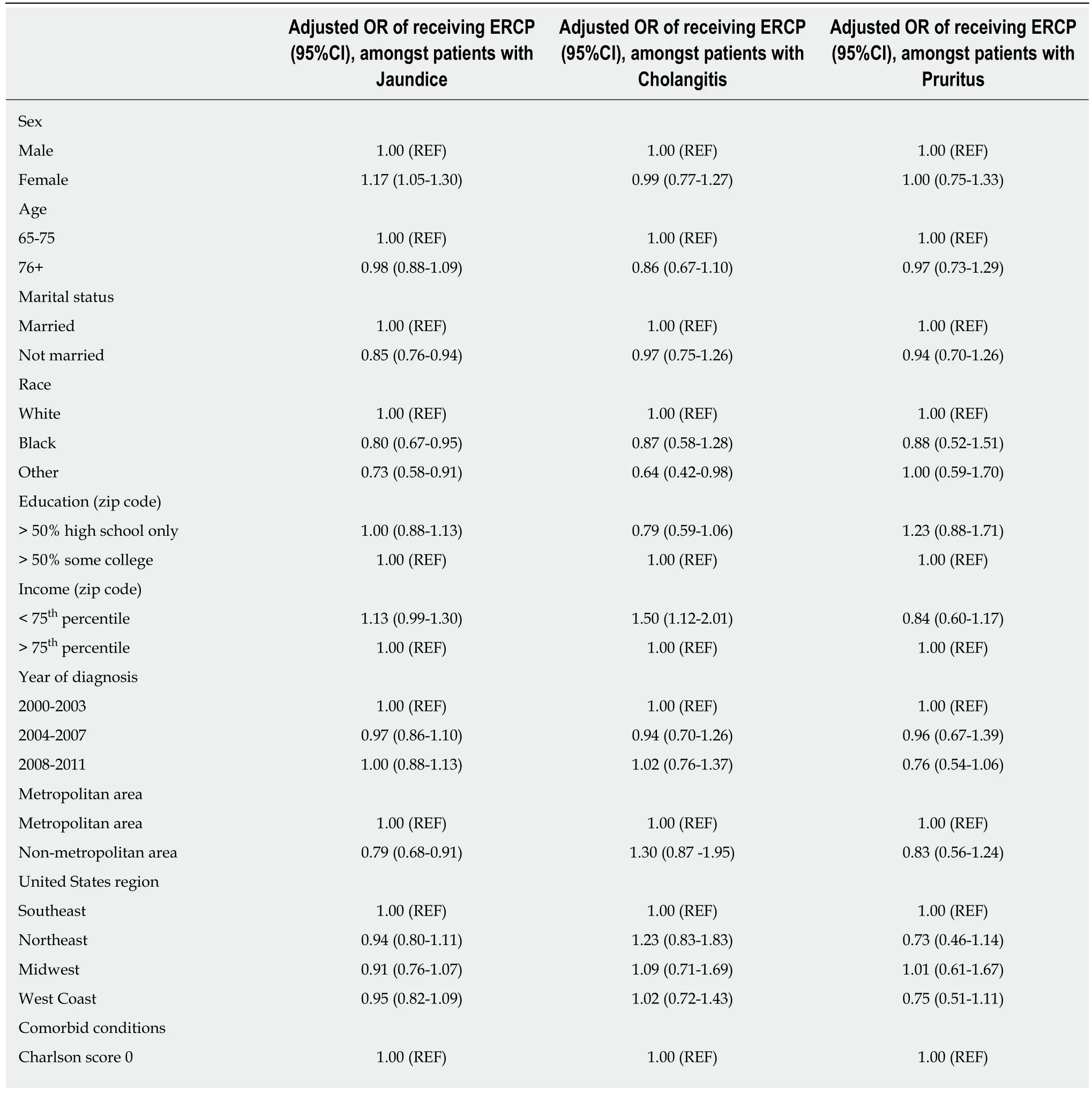
Table 5 Analysis stratified by symptoms/conditions
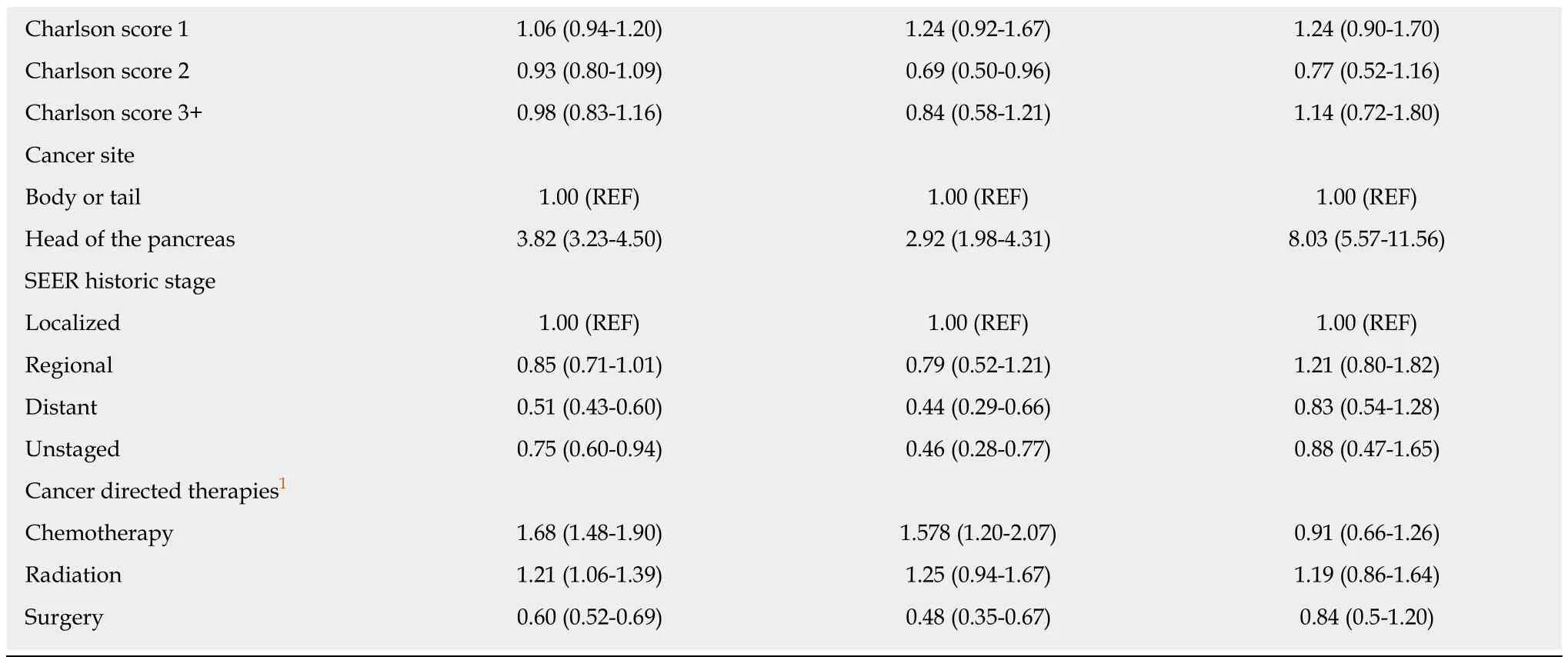
1Referent category is not undergoing these treatments. OR: Odds ratio; CI: Confidence interval; Endoscopic retrograde cholangiopancreatography.
ARTICLE HIGHLIGHTS
Research background
Endoscopic retrograde cholangiopancreatography (ERCP) is an important therapeutic procedure in the management of pancreatic cancer; before endoscopic ultrasound use was widespread, it also served an important diagnostic role. Variations in its use by patient and sociodemographic factors have not previously been described.
Research motivation
Variability in diagnosis, management and survival of pancreatic cancer by patient factors such as race are well described. However, national trends and variations in use of endoscopic procedures such as ERCP for pancreatic cancer have not previously been described. We hypothesized that there would be variations that may partially explain some of the disparities in outcomes.
Research objectives
We sought to describe variations in receipt of ERCP by patient factors including sociodemographic status, regional location in the country, clinical factors such as stage and comorbidities, and receipt of cancer directed therapies.
Research methods
This is a retrospective cohort study of Medicare claims data. Logistic regression was used to identify patient characteristics associated with the use of ERCP.
Research results
Fourteen thousand seven hundred and four patients diagnosed with pancreatic cancer underwent ERCP between 2000 and 2011. After multivariable analysis, we found multiple factors were associated with receipt of ERCP, including marital status, age, race, living in a nonmetropolitan area, year of diagnosis. Even amongst patients with an indication for ERCP(jaundice, cholangitis, pruritus) there were racial differences in use of ERCP. Whether or not these differences contribute to differences in outcomes is a future area of study.
Research conclusions
These findings suggest that use of ERCP in this country varies with non-clinical factors, such as patient race and marital status. This is similar to previous studies which suggest that there are disparities in stage at diagnosis, use of surgery and chemotherapy by sociodemographic factors.It is unclear what impact, if any, this may have on important patient outcomes such as survival.
Research perspectives
Further studies are needed to identify whether use of endoscopy in pancreatic cancer impacts outcomes, such as survival, and to guide appropriate use of biliary interventions in patients with pancreatic cancer.
杂志排行

World Journal of Gastrointestinal Endoscopy的其它文章
- Role of endoscopy in acute gastrointestinal bleeding in real clinical practice: An evidence-based review
- Role of endoscopy in the management of primary sclerosing cholangitis
- Radiofrequency and malignant biliary strictures: An update
- Endoscopic ultrasound-guided drainage of the biliary system:Techniques, indications and future perspectives
- Spectrum of gastrointestinal involvement in Stevens - Johnson syndrome
- No significant difference in clinically relevant findings between Pillcam® SB3 and Pillcam® SB2 capsules in a United States veteran population