降钙素原和C反应蛋白在鉴别老年人急性胆道感染中的价值
2019-02-18陈敏
陈敏


摘 要 目的:探討降钙素原(PCT)和C反应蛋白(CRP)鉴别老年人急性胆道感染的价值。方法:选择2015年1月至2018年3月就诊的老年急性胆道感染患者63例,按疾病不同分为急性胆管炎组31例和急性胆囊炎组32例,同时取同期慢性胆囊炎患者30例作为对照组。检测三组血清PCT、CRP浓度和白细胞计数,观察PCT、CRP检测在鉴别急性胆囊炎与急性胆管炎中的价值。结果:急性胆管炎组的PCT、CRP浓度分别为(17.646±2.146)ng/L和(128.755±12.964)mg/L,急性胆囊炎组分别为(12.727±3.041)ng/L和(116.231±6.615)mg/L,对照组分别为(0.108±0.027)ng/L和(10.16±1.279)mg/L,组间差异有统计学意义(P<0.05)。ROC曲线显示,CRP灵敏度为0.77,特异度为0.78;PCT灵敏度为0.87,特异度为0.84;PCT检测的灵敏度和特异度均优于CRP(P<0.05)。结论:检测血清PCT、CRP可以判别老年人急性胆道感染(疾病早期)的严重程度,而且PCT、CRP与老年人急性胆道感染严重程度呈正相关。
关键词 急性胆道感染;急性胆管炎;降钙素原;C反应蛋白
中图分类号:R657.4 文献标志码:A 文章编号:1006-1533(2019)02-0013-03
The value of procalcitonin and C-reactive protein in the differential diagnosis of acute biliary tract infection in the elderly
CHEN Min(Department of Clinical Laboratory of Community Health Service Center of Pengpuxincun of Jingan District, Shanghai 200435, China)
ABSTRACT Objective: To explore the value of procalcitonin(PCT) and C-reactive protein(CRP) in the differential diagnosis of acute biliary tract infection in the elderly. Methods: Sixty-three elderly patients with acute biliary tract infection at the clinic from January 2015 to March 2018 were selected and according to different diseases divided into an acute cholangitis group with 31 cases and an acute cholecystitis group with 32 ones. Meanwhile, 30 patients with chronic cholecystitis at the same time were taken as a control group. Serum levels of PCT, CRP concentration and white blood cell count were detected in the three groups to observe the value of PCT and CRP in the differential diagnosis between acute cholecystitis and acute cholangitis. Results: The PCT and CRP concentrations in the acute cholangitis group were (17.646±2.146) ng/L and (128.755±12.964) mg/ L, respectively, those in the acute cholecystitis group were (12.727±3.041) ng/L and (116.231±6.615) mg/L, respectively, those in the control group were (0.108±0.027) ng/L and (10.16±1.279) mg/L, respectively, and the difference between the groups was statistically significant(P<0.05). The ROC curve showed that the CRP sensitivity was 0.77 and the specificity was 0.78; PCT sensitivity was 0.87 and specificity was 0.84; the sensitivity and specificity of PCT detection were superior to CRP(P<0.05). Conclusion: Detection of serum PCT and CRP can determine the severity of acute biliary infection(early disease) in the elderly; moreover, PCT and CRP are positively correlated with the severity of acute biliary infection in the elderly.
KEY WORDS acute biliary infection; acute cholangitis; procalcitonin; C-reactive protein
急性胆管炎的发病机制是由于胆道系统部分或完全梗阻而引起的细菌感染[1-2],患者中70%可表现为右上腹痛、寒战高热、黄疸(Charcot三联征)[3-4],具有起病急,进展快及临床处理困难等特点,易发生感染性休克,甚至多器官功能衰竭,是良性胆道疾病死亡主要原因之一[5-6]。急性胆管炎与急性胆囊炎的急性期临床症状十分相似,老年人因其特殊的生理特征,导致临床上很难鉴别。因此,如何早期鉴别老年人急性胆管炎与急性胆囊炎、帮助临床医生掌握手术或内镜治疗时机、减少并发症以及病死率是目前的难题。本文通过测定急性胆道感染老年患者的血清降钙素原(proealcitonin,PCT)和C反应蛋白(C-reactive protein,CRP)浓度,探讨两者在鉴别老年人群急性胆管炎与急性胆囊炎的临床参考价值。
1 资料与方法
1.1 一般资料
选取2015年1月至2018年3月在上海市静安区彭浦新村街道社区卫生服务中心就诊的老年急性胆道感染患者63例,均经B超、上腹部CT或磁共振胰胆管造影(magnetic resonance cholangiopancreatography,MRCP)确诊。将患者分为急性胆管炎组和急性胆囊炎组。急性胆管炎组31例,其中男性14例,女性17例,年龄73~88岁,平均(81.2±4.2)岁;急性胆囊炎组32例,其中男性15例,女性17例,年龄69~89岁,平均(80.3±3.6)岁。选取同期慢性胆囊炎患者30例作为对照组,其中男性14例,女性16例,年龄69~90岁,平均(80.6±4.9)岁。排除肝硬化、急性病毒性肝炎、肝脓肿、慢性肝病、自身免疫性肝炎及同时伴有其他部位感染患者。
1.2 方法
所有患者就诊后,在使用抗生素药物治疗前在无菌条件下采集静脉血5 ml,置于血清分离管中,待血液凝固后用高速离心机离心,取血清进行PCT和CRP检测。另用EDTA抗凝管采集静脉血2 ml,充分混匀进行白细胞计数。PCT采用Roche Cobas E601型全自动电化学发光免疫分析仪(德国Roche Cobas公司)检测(>0.5 ng/L为阳性);CRP采用PA-900型特定蛋白分析仪(普门公司)测定(≥10 mg/L为阳性);白细胞计数采用XS-800i五分类血液分析仪(Sysmex公司)檢测,所有操作均严格按说明书进行。
1.3 统计学处理
2 结果
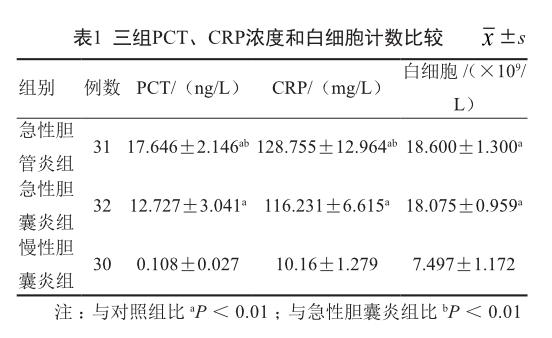
2.1 三组血清PCT、CRP浓度和白细胞计数
急性胆管炎组的PCT、CRP浓度明显高于急性胆囊炎组(P<0.05),但急性胆管炎组与急性胆囊炎组的白细胞计数差异无统计学意义(P>0.05)。急性胆管炎组和急性胆囊炎组的PCT、CRP浓度和白细胞计数较对照组明显升高(P<0.05)。见表1。
2.2 PCT和CRP检测的敏感度和特异度
从图1可见,PCT、CRP浓度和白细胞计数表现出最高的价值曲线下面积(AUC)为白细胞0.61(0.47~0.75),CRP 0.81(0.70~0.93),PCT 0.92(0.84~0.99)。与此同时,采用Youden指数法计算血清PCT和CRP的最佳诊断分界点分别为15.36和120.83,此时CRP灵敏度为0.77,特异度为0.78;PCT灵敏度为0.87,特异度为0.84。PCT检测的灵敏度和特异度均优于CRP(P<0.05)。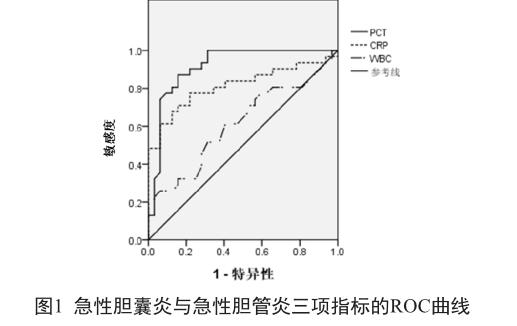
3 讨论
急性胆管炎因胆道梗阻引起胆管内细菌明显增多和胆管内压力迅速增高,致使细菌或内毒素回流至血液,最终导致胆道急性化脓性感染[7-9]。随着中国年龄结构的变化,老龄化趋势加重,从而老年人急性胆管炎的发病率也随之逐年上升。由于老年人生理功能下降,中枢神经系统和周围神经系统传递功能减退,对痛觉反应比较迟钝,大部分缺乏典型的临床症状和体征。然而,临床上老年人的急性胆管炎与急性胆囊炎的症状十分相似,容易造成漏诊、误诊,因此早期确诊以及有效解除胆道梗阻可以减少其并发症,从而有效地降低死亡率,改善预后[2,10]。
PCT属于无激素活性糖蛋白,可作为细菌感染的早期诊断标志物[11]。PCT作为新的炎症指标已普遍用于各类细菌感染性疾病的临床诊断与鉴别诊断。在没有全身细菌或真菌感染的情况下,PCT通常是由甲状腺C细胞产生的一种降钙素前体蛋白[12],几乎不释放到人体血液中,其浓度在健康人群血液中很低,甚至检测不到(<0.05 ng/ml)[11-13]。但在全身细菌感染情况下,全身各器官(肺、肾、肝、脂肪细胞和肌肉)大量合成并释放PCT,血清PCT水平急剧增加[11-17],而且体内血清PCT水平与机体感染的严重程度呈正相关[11,18]。美国传染病学会和危重病学会联合推荐PCT作为区别脓毒血症和非感染性全身炎症反应的辅助诊断标志物[19]。有研究表明PCT在病毒感染时表现为低水平[14]。
本研究表明,急性胆管炎组和急性胆囊炎组的PCT浓度明显高于对照组(P<0.01),与文献报道一致[2]。同时,急性胆管炎组PCT浓度明显高于急性胆囊炎组(P<0.01),表明PCT可以明显区分老年人急性胆管炎与急性胆囊炎,而且随着疾病进展,PCT浓度与疾病的感染严重程度呈一定相关性[1-2,22]。目前,越来越多的研究表明,PCT是具有敏感性、特异性的全身性细菌或真菌感染标志物,在疾病发生的早期阶段,其浓度升高速度快于其他生物标志物[11,15-17]。
CRP作为临床上一种较为敏感的炎症指标标志物,同时也是急性时相反应蛋白中重要的蛋白之一,健康人血清CRP浓度很低(正常值:0.068~8.2 mg/L),在感染、风湿性疾病、手术等炎性改变的不同病理状态下,其血清浓度大多会升高。有研究报道,CRP在细菌感染时会明显增高[20]。本研究数据表明,CRP在急性胆道感染时会明显增高[2,21],与疾病的感染严重程度呈正相关。然而,通过敏感度和特异度比较,PCT指标均优于CRP,说明血清PCT浓度检测是区分老年人急性胆囊炎与急性胆管炎较好的指标。
白细胞是人体免疫防御的重要组成部分,健康人血液中的正常数值为(3.5~9.5)×109/L。当病原微生物入侵机体时,其会向机体的炎症部位迁移、聚集,对病原体发挥吞噬、杀伤作用,尤其是当细菌侵入机体时,此时机体外周血白细胞数会明显升高。本研究证实,当机体有细菌感染时,白细胞总数会显著增高,但在临床上无法判别是急性胆囊炎还是急性胆管炎。
综上所述,测定血清PCT、CRP浓度可以判别老年人急性胆道感染(疾病早期)的严重程度,为进一步治疗争取宝贵时机。而且血清PCT、CRP浓度与老年人急性胆道感染严重程度呈正相关,对老年人急性胆管炎的病情评估及治疗具有指导意义。同时,PCT检测的敏感度和特异度均优于CRP,是判别老年人急性胆道感染严重程度的较好指标。由于本研究为单中心的回顾性研究,收集病例数较少,还有待于今后多中心临床研究进一步证实。
参考文献
[1] Umefune G, Kogure H, Hamada T, et a1. Procalcitonin is a useful biomarker to predict severe acute cholangitis a singlecenter prospective study[J]. J Gastroenterol, 2017, 52(6): 734-745.
[2] Sato M, Matsuyama R, Kadokura T, et a1. Severity and prognostic assessment of the endotoxin activity assay in biliary tract infection[J]. J Hepatobiliary Pancreat Sci, 2014, 21(2): 120-127.
[3] Gigot JF, Leese T, Dereme T, et a1. Acute cholangitis. Multivariate analysis of risk factors[J]. Ann Surg, 1989, 209(4): 435-438.
[4] OConnor HJ, Vickers CR, Buckels JA, et al. Role of endoscopic retrograde cholangiopancreatography after orthotopic liver transplantation[J]. Gut, 1991, 32(4): 419-423.
[5] 何三光. 中国外科专家经验文集[M]. 沈阳: 沈阳出版社, 1993: 600-602.
[6] Kiriyama S, Takada T, Strasberg SM, et al. New diagnostic criteria and severity assessment of acute cholangitis in revised Tokyo Guidelines[J]. J Hepatobiliary Pancreat Sci, 2012, 19(5): 548-556.
[7] Kimura Y, Takada T, Strasberg SM, et al. TG13 current terminology, etiology, and epidemiology of acute cholangitis and cholecystitis[J]. J Hepatobiliary Pancreat Sci, 2013,20(1): 8-23.
[8] Ahrendt S, Pitt H. The biliary tract[J]// Sabiston text book of surgery, 17th ed. Philadelphia: W. B. Saunders, 2004, 1625.
[9] Mosler P. Diagnosis and management of acute cholangitis[J]. Curr Gastroenterol Rep, 2011, 13(2): 166-172.
[10] 陳飞. 老年急症重症胆管炎最佳手术时机探讨和体会[J].中华肝胆外科杂志, 2012, 18(4): 264-265.
[11] Assicot M, Gendrel D, Carsin H, et al. High serum procalcitonin concentrations in patients with sepsis and infection[J]. Lancet, 1993, 341(8844): 515-518.
[12] Shinya S, Sasaki T, Yamashita Y, et al. Procalcitonin as a useful biomarker for determining the need to perform emergency biliary drainage in cases of acute cholangitis[J]. J Hepatobiliary Pancreat Sci, 2014, 21(10): 777-785.
[13] Maruna P, Nedelníková K, Gürlich R. Physiology and genetics of procalcitonin[J]. Physiol Res, 2000; 49 Suppl 1: S57-61.
[14] Christ-Crain M, Müller B. Procalcitonin in bacterial infections--hype, hope, more or less?[J]. Swiss Med Wkly, 2005, 135(31-32): 451-460.
[15] Becker KL, Nylen ES, White JC, et al. Clinical review 167:procalcitonin and the calcitonin gene family of peptides in inflammation, infection, and sepsis: a journey from calcitonin back to its precursors[J]. J Clin Endocrinol Metab, 2004, 89(4): 1512–1525.
[16] Becker KL, Snider R, Nylen ES. Procalcitonin assay in systemic inflammation, infection, and sepsis: clinical utility and limitations[J]. Crit Care Med, 2008, 36(3): 941–952.
[17] Jensen JU, Heslet L, Jensen TH, et al. Procalcitonin increase in early identification of critically ill patients at high risk of mortality[J]. Crit Care Med, 2006, 34(10): 2596–2602.
[18] de Azevedo JR, Torres OJ, Beraldi RA, et a1. Prognostic evaluation of severe sepsis and septic shock: procalcitonin clearance vs a sequential organ failure assessment[J]. J Crit Care, 2015, 30(1): 219.e9-12 .
[19] OGrady NP, Barie PS, Bartlett JG, et a1. Guidelines for evaluation of new fever in critically ill adult patients: 2008 update from the American College of Critical Care Medicine and the Infectious Diseases Society of America[J]. Crit Care Med, 2008, 36(4): 1330-1349.
[20] García Vázquez E, Martínez JA, Mensa J, et a1. C-reactive protein levels in community-acquired pneumonia[J]. Eur Respir J, 2003, 21(4):702-705.
[21] Lin J, Sun H, Li J, Zheng Y, et a1. Role of presepsin for the assessment of acute cholangitis severity[J]. Clin Lab, 2016, 62(4): 679-687.
