声脉冲辐射力成像与实时剪切波弹性成像诊断肝纤维化程度的价值研究
2017-11-01陈雪梅江小英卢咏梅夏良华
陈雪梅,江小英,卢咏梅,夏良华
·全科医生技能发展·
声脉冲辐射力成像与实时剪切波弹性成像诊断肝纤维化程度的价值研究
陈雪梅1*,江小英2,卢咏梅1,夏良华3
目的探讨声脉冲辐射力成像(ARFI)、实时剪切波弹性成像(SWE)诊断肝纤维化程度的价值,以期为临床工作提供参考。方法选择2015年1月—2016年5月于上海市东方医院吉安医院就诊的符合纳入标准的慢性肝病患者149例为研究对象。收集患者一般资料,分别采用ARFI、SWE检测患者的肝实质硬度(LS)。根据ARFI、SWE检查结果,将患者分别分为ARFI检测到LS组、ARFI未检测到LS组和SWE检测到LS组、SWE未检测到LS组。收集并比较ARFI检测到LS组与ARFI未检测到LS组、SWE检测到LS组与SWE未检测到LS组患者性别、年龄、BMI、丙氨酸氨基转移酶(ALT)水平。采用多因素Logistic回归分析计算ARFI、SWE联合的多因素Logistic回归方程;以超声引导下肝脏穿刺活检结果为金标准,分别绘制ARFI、SWE及其联合诊断慢性肝病患者肝纤维化程度(≥S2、≥S3、S4期)的受试者工作特征曲线(ROC曲线),计算ROC曲线下面积(AUC)、灵敏度、特异度。结果ARFI检测到LS率高于SWE(P<0.05)。ARFI检测到LS组与ARFI未检测到LS组患者性别、年龄、BMI、ALT水平比较,差异均无统计学意义(P>0.05)。SWE检测到LS组与SWE未检测到LS组患者性别、年龄、ALT水平比较,差异均无统计学意义(P>0.05);SWE检测到LS组患者BMI低于SWE未检测到LS组(P<0.05)。ARFI、SWE及其联合诊断慢性肝病患者肝纤维化≥S2期的AUC分别为0.936〔95%CI(0.895,0.978)〕、0.837〔95%CI(0.754,0.919)〕、0.972〔95%CI(0.949,0.995)〕,临界值分别为1.32 m/s、17.14 kPa、-9.228,灵敏度分别为87.8%、80.0%、91.1%,特异度分别为97.3%、83.8%、91.9%。ARFI、SWE及其联合诊断慢性肝病患者肝纤维化≥S3期的AUC分别为0.915〔95%CI(0.859,0.970)〕、0.867〔95%CI(0.796,0.938)〕、0.910〔95%CI(0.851,0.968)〕,临界值分别为1.45 m/s、25.36 kPa、7.114,灵敏度分别为90.9%、85.5%、90.9%,特异度分别为88.9%、87.5%、91.7%。ARFI、SWE及其联合诊断慢性肝病患者肝纤维化S4期的AUC分别为0.860〔95%CI(0.746,0.974)〕、0.948〔95%CI(0.902,0.993)〕、0.975〔95%CI(0.949,1.000)〕,临界值分别为1.52 m/s、38.54 kPa、1.878,灵敏度分别为88.0%、96.0%、96.0%,特异度分别为92.2%、93.1%、91.2%。ARFI单独诊断慢性肝病患者肝纤维化≥S2、≥S3期的AUC大于SWE,诊断慢性肝病患者肝纤维化S4期的AUC小于SWE(P<0.05)。ARFI单独诊断慢性肝病患者肝纤维化≥S2、S4期的AUC小于ARFI、SWE联合(P<0.05);ARFI单独诊断慢性肝病患者肝纤维化≥S3期的AUC与ARFI、SWE联合比较,差异无统计学意义(P>0.05)。SWE单独诊断慢性肝病患者肝纤维化≥S2、≥S3、S4期的AUC小于ARFI、SWE联合(P<0.05)。结论ARFI、SWE联合诊断肝纤维化程度的价值较单独ARFI、SWE好。
肝硬化;肝纤维化;超声检查;诊断;超声辐射脉冲成像;实时剪切波弹性成像
陈雪梅,江小英,卢咏梅,等.声脉冲辐射力成像与实时剪切波弹性成像诊断肝纤维化程度的价值研究[J].中国全科医学,2017,20(30):3796-3802.[www.chinagp.net]
CHEN X M,JIANG X Y,LU Y M,et al.Value of acoustic radiation force impulse imaging versus real-time shear wave elastography in the diagnosis of hepatic fibrosis[J].Chinese General Practice,2017,20(30):3796-3802.
由于各种病因导致的慢性肝病会持续反复引起肝实质发生炎症、变性坏死等病理改变,导致肝脏纤维结缔组织增生从而发生肝纤维化[1]。而各种慢性肝炎的早期并无特异性症状和体征,许多患者在出现明显症状后再就诊时常已进展为肝硬化甚至肝衰竭等。由于肝纤维化本身是可逆的,如果能早期诊断并采取合理的干预措施,可以延缓甚至阻断其进展。而即使是到了肝硬化阶段,如果能及早检查发现,也可以有效避免失代偿性肝硬化引起的腹腔积液、消化道大出血等不良后果[2]。因此,采取能有效检出肝纤维化的方法对患者进行检查,随访其肝脏病变情况具有重要的临床意义。
目前诊断肝纤维化或肝硬化的金标准是肝脏组织活检,但其具有创伤性,且不宜重复取样。因此,寻找准确、无创伤、可重复的检查方法,对于动态观察患者肝脏病变情况极其重要。近年来,出现了声脉冲辐射力成像(ARFI)、实时剪切波弹性成像(SWE)等可用于检测肝纤维化和肝硬化的超声技术,且其具有无创、可重复、操作简便等优点[3]。ARFI和SWE在临床上均有较多的应用,但其诊断肝纤维化的效能是否存在差异尚不清楚。因此,本研究对比分析了ARFI、SWE及其联合诊断肝纤维化的价值,以期为临床工作提供参考。
1 对象与方法
1.1 纳入与排除标准 纳入标准:(1)超声引导下肝脏穿刺活检确诊,并依据病毒性肝炎防治方案[4]对肝纤维化程度进行分期:S0期,无纤维化;S1期,汇管区纤维化扩大,局限窦周及小叶内纤维化;S2期,汇管区周围纤维化,纤维间隔形成,小叶结构保留;S3期,纤维间隔伴小叶结构紊乱,无肝硬化;S4期,早期肝硬化。其中≥S2期为轻-重度肝纤维化,≥S3期为重度肝纤维化,S4期为早期肝硬化。(2)穿刺前接受肝脏ARFI、SWE检查。排除标准:肝脏恶性肿瘤者。
1.2 研究对象 选择2015年1月—2016年5月于上海市东方医院吉安医院就诊的符合纳入标准的慢性肝病患者149例为研究对象。本研究通过了上海市东方医院吉安医院伦理委员会审批,患者均了解研究意义并签署知情同意书。
1.3 研究方法
1.3.1 一般资料收集 收集患者一般资料,包括性别、年龄、BMI、丙氨酸氨基转移酶(ALT)水平、疾病类型、肝纤维化分期。
1.3.2 ARFI检查 采用ACOUSON S3000彩色超声诊断仪(西门子股份公司)对患者进行肝脏ARFI检查,6C l凸阵探头,频率为1.0~6.0 MHz,由同一名超声医师操作。患者取仰卧位或左侧卧位,将探头置于肝脏右前叶处,弹性取样框与肝脏表面垂直,置于距探头表面约4 cm的肝脏实质区域内,并避开周围管道结构。检查时嘱患者屏住呼吸,发动高强度低频的脉冲波,接收并记录其横向剪切波速度(Vs)(见图1),单位m/s。Vs越大,表明肝脏硬度越大。每例患者重复检查10次,取平均值记为肝实质硬度(LS)。
1.3.3 SWE检查 采用AixPlorer型实时剪切波弹性成像超声诊断仪(法国 Supersonic Imagine公司)对患者进行肝脏SWE检查,SC6-1凸探头,频率为1~6 MHz,由同一名超声医师操作。患者取平卧位,右上肢上抬,先将探头置于患者的右锁骨中线4~5肋间做二维超声检测,选择肝右叶进行检测,切换到弹性成像模式后,将取样框置于肝包膜下1~5 cm的肝实质内,并避开周围管道结构。嘱患者吸气并屏住呼吸3~5 s进行成像,选取直径为2 cm左右的感兴趣区域测量弹性值,单位为kPa(见图2)。弹性值为杨氏模量值,该值越大表明肝脏硬度越大。每例患者重复测量5次,取平均值记为LS。
1.4 分组及观察指标 根据ARFI、SWE检查结果,将患者分别分为ARFI检测到LS组、ARFI未检测到LS组和SWE检测到LS组、SWE未检测到LS组。收集并比较ARFI检测到LS组与ARFI未检测到LS组、SWE检测到LS组与SWE未检测到LS组患者性别、年龄、BMI、ALT水平。

本研究价值:
肝纤维化具有可逆性,早期诊断及干预可以延缓进展。肝组织活检具有创伤性、不宜重复取样等缺点。而声脉冲辐射力成像(ARFI)、实时剪切波弹性成像(SWE)具有无创、可重复、操作简便等优点。本研究对比分析了ARFI、SWE及其联合诊断肝纤维化程度(≥S2、≥S3、S4期)的价值,结果显示,对于早期肝纤维化患者优先使用ARFI,对于肝纤维化S4期的患者则优先使用SWE,而单独ARFI或SWE诊断结果不明确或对诊断结果有所怀疑时,或者不了解患者肝纤维化程度时,两者联合诊断可以提高诊断正确率。
2 结果
2.1 一般资料 149例患者中,男84例,女65例;年龄21~74岁,平均年龄(53.4±12.9)岁;BMI(27.0±5.8)kg/m2;ALT(58.8±20.3)U/L;疾病类型:慢性乙型肝炎103例,慢性丙型肝炎20例,药物损伤性肝炎13例,原发性胆汁性肝硬化10例,酒精性肝炎3例;肝纤维化分期:S0期11例,S1期40例,S2期40例,S3期33例,S4期25例;ARFI检测到LS 140例(94.0%),SWE检测到LS 127例(85.2%)。ARFI检测到LS率高于SWE,差异有统计学意义(χ2=4.111,P=0.043)。
2.2 ARFI检测到LS组与ARFI未检测到LS组患者性别、年龄、BMI、ALT水平比较 ARFI检测到LS组与ARFI未检测到LS组患者性别、年龄、BMI、ALT水平比较,差异均无统计学意义(P>0.05,见表1)。
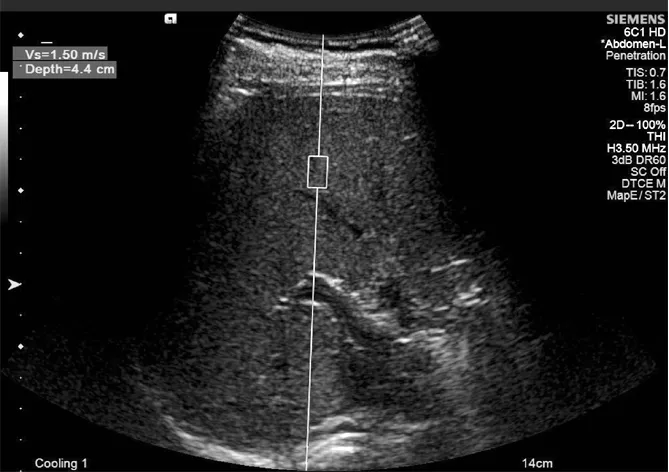
图1 肝脏ARFI检查

图2 肝脏SWE检查
表1 ARFI检测到LS组与ARFI未检测到LS组患者性别、年龄、BMI、ALT水平比较
Table1 Sex distribution,age distribution,BMI and ALT levels in group with ARFI-identified LS and group without ARFI-identified LS
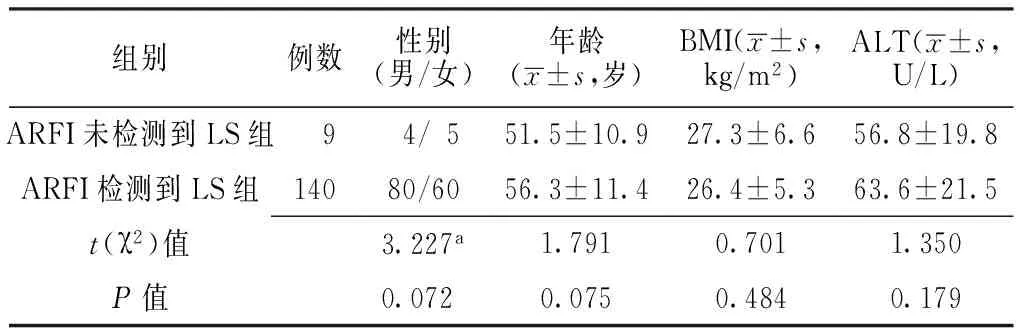
组别例数性别(男/女)年龄(x±s,岁)BMI(x±s,kg/m2)ALT(x±s,U/L)ARFI未检测到LS组 9 4/5 51.5±10.927.3±6.656.8±19.8ARFI检测到LS组14080/6056.3±11.426.4±5.363.6±21.5t(χ2)值3.227a1.7910.7011.350P值0.0720.0750.4840.179
注:a为χ2值;ARFI=声脉冲辐射力成像,LS=肝实质硬度,ALT=丙氨酸氨基转移酶
2.3 SWE检测到LS组与SWE未检测到LS组患者性别、年龄、BMI、ALT水平比较 SWE检测到LS组与SWE未检测到LS组患者性别、年龄、ALT水平比较,差异均无统计学意义(P>0.05);SWE检测到LS组患者BMI低于SWE未检测到LS组,差异有统计学意义(P<0.05,见表2)。
表2 SWE检测到LS组与SWE未检测到LS组患者性别、年龄、BMI、ALT水平比较
Table2 Sex distribution,age distribution,BMI and ALT levels in group with SWE-identified LS and group without SWE-identified LS

组别例数性别(男/女)年龄(x±s,岁)BMI(x±s,kg/m2)ALT(x±s,U/L)SWE未检测到LS组 22 14/855.8±12.430.3±6.061.8±21.0SWE检测到LS组12770/5752.1±10.824.2±6.756.7±19.4t(χ2)值1.497a1.4515.9221.622P值0.2210.149<0.0010.106
注:a为χ2值;SWE=实时剪切波弹性成像
2.4 ARFI、SWE及其联合诊断慢性肝病患者肝纤维化程度的价值 ARFI和SWE均可检测到LS 127例,其肝纤维化分期为:S0期6例,S1期31例,S2期35例,S3期30例,S4期25例。
2.4.1 ARFI、SWE及其联合诊断慢性肝病患者肝纤维化≥S2期的价值 以肝纤维化是否≥S2期为因变量(赋值:是=1,否=0),ARFI、SWE检查结果为自变量(连续型变量),进行多因素Logistic回归分析,结果显示,y=-27.069+8.530×ARFI检查结果+0.384×SWE检查结果。ARFI、SWE及其联合诊断慢性肝病患者肝纤维化≥S2期的AUC分别为0.936〔95%CI(0.895,0.978)〕、0.837〔95%CI(0.754,0.919)〕、0.972〔95%CI(0.949,0.995)〕(见图3),临界值分别为1.32 m/s、17.14 kPa、-9.228,灵敏度分别为87.8%、80.0%、91.1%,特异度分别为97.3%、83.8%、91.9%。ARFI单独诊断慢性肝病患者肝纤维化≥S2期的AUC大于SWE,差异有统计学意义(χ2=4.870,P=0.015);ARFI单独诊断慢性肝病患者肝纤维化≥S2期的AUC小于ARFI、SWE联合,差异有统计学意义(χ2=5.023,P=0.011);SWE单独诊断慢性肝病患者肝纤维化≥S2期的AUC小于ARFI、SWE联合,差异有统计学意义(χ2=10.550,P=0.001)。

注:ARFI=声脉冲辐射力成像,SWE=实时剪切波弹性成像
图3 ARFI、SWE及其联合诊断慢性肝病患者肝纤维化≥S2期的ROC曲线
Figure3 ROC curves of ARFI,SWE and ARFI combined with SWE for the diagnosis of liver fibrosis in stages 2-4 in patients with chronic liver disease
2.4.2 ARFI、SWE及其联合诊断慢性肝病患者肝纤维化≥S3期的价值 以肝纤维化是否≥S3期为因变量(赋值:是=1,否=0),ARFI、SWE检查结果为自变量(连续型变量),进行多因素Logistic回归分析,结果显示,y=-28.529+17.900×ARFI检查结果+0.382×SWE检查结果。ARFI、SWE及其联合诊断慢性肝病患者肝纤维化≥S3期的AUC分别为0.915〔95%CI(0.859,0.970)〕、0.867〔95%CI(0.796,0.938)〕、0.910〔95%CI(0.851,0.968)〕(见图4),临界值分别为1.45 m/s、25.36 kPa、7.114,灵敏度分别为90.9%、85.5%、90.9%,特异度分别为88.9%、87.5%、91.7%。ARFI单独诊断慢性肝病患者肝纤维化≥S3期的AUC大于SWE,差异有统计学意义(χ2=8.671,P=0.004);ARFI单独诊断慢性肝病患者肝纤维化≥S3期的AUC与ARFI、SWE联合比较,差异无统计学意义(χ2=2.193,P=0.072);SWE单独诊断慢性肝病患者肝纤维化≥S3期的AUC小于ARFI、SWE联合,差异有统计学意义(χ2=7.837,P=0.006)。
2.4.3 ARFI、SWE及其联合诊断慢性肝病患者肝纤维化S4期的价值 以肝纤维化是否为S4期为因变量(赋值:是=1,否=0),ARFI、SWE检查结果为自变量(连续型变量),进行多因素Logistic回归分析,结果显示,y=-16.903+9.567×ARFI检查结果+0.110×SWE检查结果。ARFI、SWE及其联合诊断慢性肝病患者肝纤维化S4期的AUC分别为0.860〔95%CI(0.746,0.974)〕、0.948〔95%CI(0.902,0.993)〕、0.975〔95%CI(0.949,1.000)〕(见图5),临界值分别为1.52 m/s、38.54 kPa、1.878,灵敏度分别为88.0%、96.0%、96.0%,特异度分别为92.2%、93.1%、91.2%。ARFI单独诊断慢性肝病患者肝纤维化S4期的AUC小于SWE,差异有统计学意义(χ2=4.462,P=0.022);ARFI单独诊断慢性肝病患者肝纤维化S4期的AUC小于ARFI、SWE联合,差异有统计学意义(χ2=8.736,P=0.003);SWE单独诊断慢性肝病患者肝纤维化S4期的AUC小于ARFI、SWE联合,差异有统计学意义(χ2=7.243,P=0.008)。

图4 ARFI、SWE及其联合诊断慢性肝病患者肝纤维化≥S3期的ROC曲线
Figure4 ROC curves of ARFI,SWE and ARFI combined with SWE for the diagnosis of liver fibrosis in stages 3-4 in patients with chronic liver disease

图5 ARFI、SWE及其联合诊断慢性肝病患者肝纤维化S4期的ROC曲线
Figure5 ROC curves of ARFI,SWE and ARFI combined with SWE for the diagnosis of liver fibrosis in stage 4 in patients with chronic liver disease
3 讨论
肝纤维化是机体对于慢性肝损伤产生的一种修复反应,可进展为失代偿期肝硬化、肝癌等严重影响患者生命安全的疾病[1,5]。而肝纤维化如能在早期确诊,并进行合理的治疗,可以有效延缓甚至逆转进程。目前诊断肝纤维化的金标准是肝组织穿刺活检,但其具有创伤性,且存在穿刺引发癌细胞种植转移等风险以及并发症,不宜重复检测,难以动态观察患者肝纤维化进展[2,6-8]。超声作为一种操作简便、经济、可重复进行的无创检查,是肝脏观察中应用最多的影像学方法。但肝脏早期出现纤维化时,其组织的声界面特征抗阻差或声强散射系数变化并不显著,因此常规的超声检查诊断肝纤维化的灵敏度和特异度不高[9-10]。然而,弹性成像技术克服了常规超声检查的局限性,在肝纤维化早期即可检测出肝脏弹性模量即肝脏硬度变化[11-12]。
本研究结果显示,ARFI检测到LS率高于SWE,说明单纯ARFI在整体检测LS方面可能较单纯SWE效果好。SWE检测到LS组患者BMI低于SWE未检测到LS组,说明BMI可能会影响SWE检测LS,可能是由于BMI较大的患者腹壁脂肪层较厚,影响测量[13]。ARFI、SWE单独诊断慢性肝病患者肝纤维化≥S2期的AUC分别为0.936、0.837,临界值分别为1.32 m/s、17.14 kPa,灵敏度分别为87.8%、80.0%,特异度分别为97.3%、83.8%;ARFI、SWE单独诊断慢性肝病患者肝纤维化≥S3期的AUC分别为0.915、0.867,临界值分别为1.45 m/s、25.36 kPa,灵敏度分别为90.9%、85.5%,特异度分别为88.9%、87.5%;ARFI、SWE单独诊断慢性肝病患者肝纤维化S4期的AUC分别为0.860、0.948,临界值分别为1.52 m/s、38.54 kPa,灵敏度分别为88.0%、96.0%,特异度分别为92.2%、93.1%;可见ARFI和SWE两种技术对肝纤维化均有较好的诊断效能。ARFI单独诊断慢性肝病患者肝纤维化≥S2期、≥S3期的AUC大于SWE,说明与SWE比较,ARFI在慢性肝病早期检测肝纤维化中有良好的价值。ARFI单独诊断慢性肝病患者肝纤维化S4期的AUC小于SWE,说明SWE在慢性肝病时间较长、重度肝纤维化或早期肝硬化患者中有较好的诊断价值,这与FERRAIOLI等[14]的研究结果一致。
ARFI、SWE单独诊断慢性肝病患者肝纤维化≥S2期、S4期的AUC小于ARFI、SWE联合;ARFI单独诊断慢性肝病患者肝纤维化≥S3期的AUC与ARFI、SWE联合无差异;SWE单独诊断慢性肝病患者肝纤维化≥S3期的AUC小于ARFI、SWE联合。ARFI通过向所测组织区域发射推进脉冲,使局部形变并产生横向剪切波,系统可采集该剪切波信号并计算出Vs,从而诊断组织的弹性模量[15];而SWE通过超高速成像系统采集组织内产生的剪切波,并根据相关公式计算出弹性模量值(杨氏模量值),即所测组织的硬度绝对值[16]。两种技术的检测原理有所差异,两者联合可以弥补不足,提高诊断效能。因此,在临床工作中,对于单用ARFI或SWE诊断肝纤维化结果不明确或对结果有所怀疑时,可以选择两者联合,以提高对肝纤维化诊断的正确率。而当考虑经济因素等情况不能同时进行两项检查时,对肝纤维化早期患者可以优先使用ARFI,对于肝纤维化S4期患者则优先使用SWE。
然而,本研究纳入患者仅限于同一医院就诊患者,可能具有地域局限性,可以进一步研究多地域患者,扩大各期、各种原因所致肝纤维化疾病的患者例数,获得更具有说服力的研究结果,以指导临床应用。
综上所述,ARFI、SWE联合诊断肝纤维化程度的价值较单独ARFI、SWE好。因此,ARFI和SWE联用是准确、可重复、无创的动态监测肝纤维进展的一个良好方法。
作者贡献:陈雪梅、江小英、卢咏梅进行文章的构思与设计,论文修订,统计学处理;陈雪梅、江小英、夏良华进行研究的实施与可行性分析,数据的收集与整理,结果分析与解释,文章的质量控制及审校;陈雪梅撰写论文,对文章整体负责,监督管理。
本文无利益冲突。
[1]李楚天,何青莲,罗碧怡,等.慢性肝炎患者肝脏炎症程度与肝纤维化的关系[J].广东医学,2014,35(17):2713-2714.DOI:10.3969/j.issn.1001-9448.2014.17.026.
LI C T,HE Q L,LUO B Y,et al.Relationship between liver inflammation and liver fibrosis in patients with chronic hepatitis[J].Guangdong Medical Journal,2014,35(17):2713-2714.DOI:10.3969/j.issn.1001-9448.2014.17.026.
[2]滕晓英,周新刚,孙磊,等.细化慢性肝炎肝纤维化分期标准在药物疗效评定中的应用[J].中华肝脏病杂志,2013,21(4):271-274.DOI:10.3760/cma.j.issn.1007-3418.2013.04.008.
TENG X Y,ZHOU X G,SUN L,et al.Application of a refined fibrosis staging system to evaluate therapeutic efficacy in chronic viral hepatitis[J].Chinese Journal of Hepatology,2013,21(4):271-274.DOI:10.3760/cma.j.issn.1007-3418.2013.04.008.
[3]匡莉,陈萍,郭鹏,等.超声弹性成像技术在慢性乙型肝炎患者肝纤维化分级中的应用[J].山东医药,2013,53(36):88-90.DOI:10.3969/j.issn.1002-266X.2013.36.034.
KUANG L,CHEN P,GUO P,et al.Application of ultrasonic elastography in grading of hepatic fibrosis in patients with chronic hepatitis B[J].Shandong Medical Journal,2013,53(36):88-90.DOI:10.3969/j.issn.1002-266X.2013.36.034.
[4]中华医学会传染病与寄生虫病学分会,中华医学会肝病学分会.病毒性肝炎防治方案[J].中华内科杂志,2001,40(1):62-68.
Infectious Diseases and Parasitology Society of Chinese Medical Association,Hepatology Association of Chinese Medical Association.Program for prevention and treatment of viral hepatitis[J].Chinese Journal of Internal Medicine,2001,40(1):62-68.
[5]ADLER M,LAROCCA L,TROVATO F M,et al.Evaluating the risk of hepatocellular carcinoma in patients with prominently elevated liver stiffness measurements by FibroScan:a multicentre study[J].HPB(Oxford),2016,18(8):678-683.DOI:org/10.1016/j.hpb.2016.05.005.
[6]KIANI A,BRUN V,LAINÉ F,et al.Acoustic radiation force impulse imaging for assessing liver fibrosis in alcoholic liver disease[J].World J Gastroenterol,2016,22(20):4926-4935.DOI:10.3748/wjg.v22.i20.4926.
[7]SHI Y,XIA F,LI Q J,et al.Magnetic resonance elastography for the evaluation of liver fibrosis in chronic hepatitis B and C by using both gradient-recalled echo and spin-echo echo planar imaging:a prospective study[J].Am J Gastroenterol,2016,111(6):823-833.DOI:10.1038/ajg.2016.56.
[8]陈敏,张大鹍,刘阳,等.声辐射力脉冲成像技术评价慢性乙型肝炎肝纤维化程度的临床研究[J].中华超声影像学杂志,2015(4):311-315.DOI:10.3760/cmaj.i.ssn1.004-44772.0150.40.12.
CHEN M,ZHANG D K,LIU Y,et al.Diagnostic value of acoustic radiation force impulse imaging for evaluating the degree of liver fibrosis in chronic hepatitis B[J].Chinese Journal of Ultrasonography,2015(4):311-315.DOI:10.3760/cmaj.i.ssn1.004-44772.0150.40.12.
[9]何肖敏,黄坚.肝纤维化血清学标志物研究新进展[J].中华肝脏病杂志,2015,23(11):874-877.DOI:10.3760/cma.j.issn.1007-3418.2015.11.016.
HE X M,HUANG J.Recent advances in serum biomarkers for liver fibrosis[J].Chinese Journal of Hepatology,2015,23(11):874-877.DOI:10.3760/cma.j.issn.1007-3418.2015.11.016.
[10]TADA T,KUMADA T,TOYODA H,et al.Utility of real-time shear wave elastography for assessing liver fibrosis in patients with chronic hepatitis C infection without cirrhosis:comparison of liver fibrosis indices[J].Hepatol Res,2015,45(10):E122-129.DOI:10.1111/hepr.12476.
[11]贾继东.肝纤维化无创诊断技术的机会与挑战[J].中华肝脏病杂志,2014,22(9):641-642.DOI:10.3760/cma.j.issn.1007-3418.2014.09.001.
JIA J D.Non-invasive diagnostic tests for liver fibrosis:opportunities and challenges[J].Chinese Journal of Hepatology,2014,22(9):641-642.DOI:10.3760/cma.j.issn.1007-3418.2014.09.001.
[12]VERLINDEN W,BOURGEOIS S,GIGASE P,et al.Liver fibrosis evaluation using real-time shear wave elastography in hepatitis C-monoinfected and human immunodeficiency virus/hepatitis C-coinfected patients[J].J Ultrasound Med,2016,35(6):1299-1308.DOI:10.7863/ultra.15.08066.
[13]FERRAIOLI G,PAREKH P,LEVITOV A B,et al.Shear wave elastography for evaluation of liver fibrosis[J].J Ultrasound Med,2014,33(2):197-203.DOI:10.7863/ultra.33.2.197.
[14]FERRAIOLI G,TINELLI C,DAL BELLO B,et al.Accuracy of real-time shear wave elastography for assessing liver fibrosis in chronic hepatitis C:a pilot study[J].Hepatology,2012,56(6):2125-2133.DOI:10.1002/hep.25936.
[15]张大鹍,陈敏,刘阳,等.声辐射力脉冲成像与APRI指数评价慢性丙型肝炎肝纤维化的临床价值[J].中华超声影像学杂志,2013,22(1):30-33.DOI:10.3760/cma.j.issn.1004-4477.2013.01.008.
ZHANG D K,CHEN M,LIU Y,et al.Clinical value of acoustic radiation force impulse imaging and APRI for quantitative evaluating the degree of liver fibrosis in chronic hepatitis C patients[J].Chinese Journal of Ultrasonography,2013,22(1):30-33.DOI:10.3760/cma.j.issn.1004-4477.2013.01.008.
[16]王利慧,徐芸,孙璐璐,等.实时剪切波弹性成像诊断自身免疫性肝病的肝纤维化程度[J].中华内科杂志,2013,52(7):601-603.DOI:10.3760/cma.j.issn.0578-1426.2013.07.019.
WANG L H,XU Y,SUN L L,et al.Real time shear wave elastography for the diagnosis of hepatic fibrosis in autoimmune liver disease[J].Chinese Journal of Internal Medicine,2013,52(7):601-603.DOI:10.3760/cma.j.issn.0578-1426.2013.07.019.
ValueofAcousticRadiationForceImpulseImagingversusReal-timeShearWaveElastographyintheDiagnosisofHepaticFibrosis
CHENXue-mei1*,JIANGXiao-ying2,LUYong-mei1,XIALiang-hua3
1.DepartmentofFunctionExamination,Ji′anHospital,ShanghaiEastHospital,Ji′an331000,China2.DepartmentofInternalMedicine,XinganHospitalofTraditionalChineseMedicine,Xingan331300,China3.DepartmentofUltrasound,TongjiUniversityAffiliatedShanghaiEastHospital,Shanghai200120,China
*Correspondingauthor:CHENXue-mei,Associatechiefphysician;E-mail:cxm13766250380@sina.com
ObjectiveTo explore the value of acoustic radiation force impulse imaging(ARFI),versus real-time shear wave elastography(SWE) in the diagnosis of hepatic fibrosis,with a view to providing a reference for clinical work.MethodsWe enrolled 149 eligible cases diagnosed as chronic liver disease who
treatment in Ji′an Hospital,Shanghai East Hospital from January 2015 to May 2016.The patients′ baseline data were collected,and the liver stiffness(LS) was measured by SWE and ARFI,respectively.According to the results of ARFI,they were divided into group with ARFI-identified LS,and group without ARFI-identified LS.Based on the findings of SWE,they were assigned to group with SWE-identified LS,and group without SWE-identified LS.Comparisons were made between the ARFI-identified groups as well as between the SWE-identified groups in terms of sex distribution,age distribution,BMI and ALT levels.Logistic regression analysis was used to calculate the Logistic regression equation of ARFI and SWE.Ultrasound-guided liver biopsy results were set as the gold standard for assessing the diagnostic value of ARFI,SWE,and ARFI combined with SWE.The receiver operating characteristic(ROC) curve of ARFI,SWE and their combined diagnosis of hepatic fibrosis(stages 2-4,stages 3-4,stage 4) in patients with chronic liver disease were drawn.The area under the ROC curve(AUC),sensitivity and specificity for the diagnosis of hepatic fibrosis was assessed with ROC analysis.ResultsThe rate of LS identified by ARFI was higher than that by SWE(P<0.05).Sex distribution,age distribution,BMI and ALT levels did not differ significantly between group with ARFI-identified LS and group without ARFI-identified LS(P>0.05).Both of group with SWE-identified LS and group without SWE-identified LS were found with similar sex distribution,age distribution,and ALT levels(P>0.05).Patients in group with SWE-identified LS were observed to have lower BMI compared with those in the group without SWE-identified LS(P<0.05).For the diagnosis of hepatic fibrosis in stages 2-4 in chronic liver disease,the AUC of ARFI,SWE and ARFI combined with SWE were 0.936〔95%CI(0.895,0.978)〕,0.837〔95%CI(0.754,0.919)〕,0.972〔95%CI(0.949,0.995)〕,respectively,the cut-off value of them were 1.32 m/s,17.14 kPa,-9.228,respectively,the sensitivity of them were 87.8%,80.0%,91.1%,respectively,and the specificity of them were 97.3%,83.8%,91.9%,respectively.For the diagnosis of hepatic fibrosis in stages 3-4 in chronic liver disease,the AUC of ARFI,SWE and ARFI combined with SWE were 0.915〔95%CI(0.859,0.970)〕,0.867〔95%CI(0.796,0.938)〕,0.910〔95%CI(0.851,0.968)〕,respectively,the cut-off value of them were 1.45 m/s,25.36 kPa,7.114,respectively,the sensitivity of them were 90.9%,85.5%,90.9%,respectively,and the specificity of them were 88.9%,87.5%,91.7%,respectively.For the diagnosis of hepatic fibrosis in stage 4 in chronic liver disease,the AUC of ARFI,SWE and ARFI combined with SWE were 0.860〔95%CI(0.746,0.974)〕,0.948〔95%CI(0.902,0.993)〕,0.975〔95%CI(0.949,1.000)〕,respectively,the cut-off value of them were 1.52 m/s,38.54 kPa,1.878,respectively,the sensitivity of them were 88.0%,96.0%,96.0%,respectively,and the specificity of them were 92.2%,93.1%,91.2%,respectively.In terms of identifying hepatic fibrosis in stages 2-4 or stages 3-4 in chronic liver disease,ARFI had larger AUC than SWE(P<0.05),but for identifying hepatic fibrosis in stage 4,its AUC was smaller than that of SWE(P<0.05).As for identifying hepatic fibrosis in stages 2-4 or stage 4 in chronic liver disease,ARFI had smaller AUC than ARFI combined with SWE(P<0.05),but for identifying hepatic fibrosis in stages 3-4,its AUC was similar to that of ARFI combined with SWE(P>0.05).As regards identifying hepatic fibrosis in stages 2-4,stages 3-4 or stage 4,the AUC of SWE was smaller than that of ARFI combined with SWE(P<0.05).ConclusionThe value of ARFI combined with SWE in diagnosing hepatic fibrosis is better than that of ARFI or SWE alone.
Liver cirrhosis;Liver fibrosis;Ultrasonography;Diagnosis;Acoustic radiation force impulse imaging;Real-time shear wave elastography
R 575.2
A
10.3969/j.issn.1007-9572.2017.00.089
2017-03-25;
2017-08-31)
(本文编辑:崔丽红)
上海市浦东新区卫生局卫生科技项目(PW2012A-24)
1.331000 江西省吉安市,上海市东方医院吉安医院功能科 2.331300 江西省新干县中医院内科 3.200120 上海市,同济大学附属上海东方医院超声科
*通信作者:陈雪梅,副主任医师;E-mail:cxm13766250380@sina.com
