对比分析回肠袢式造口术与结肠造口术治疗老年梗阻性乙状结肠癌和高位直肠癌的临床效果
2017-10-25单汉国黄笛鸣王春云
单汉国 黄笛鸣 王春云

[摘要] 目的 分析回腸袢式造口术与结肠造口术治疗老年梗阻性乙状结肠癌和高位直肠癌的临床效果。 方法 将2014年1月~2017年1月收治的80例老年梗阻性乙状结肠癌和高位直肠癌患者作为研究对象,根据随机数字表将患者分为两组,每组40例。结肠造口组采用结肠造口术治疗,回肠袢式造口组采用回肠袢式造口术治疗。比较两组梗阻性乙状结肠癌和高位直肠癌治疗效果,第一次排气时间、手术时间,干预前后患者生存质量水平、T淋巴细胞亚群指标,并发症发生率。 结果 回肠袢式造口组梗阻性乙状结肠癌和高位直肠癌治疗总有效率为77.50%,高于结肠造口组的50.00%(P<0.05);回肠袢式造口组第一次排气时间、手术时间分别为(23.51±1.41)h、(54.51±12.61)min,短于结肠造口组的(34.40±2.77)h、(77.40±23.57)min,差异有统计学意义(P<0.05);干预前两组生存质量水平、T淋巴细胞亚群指标相近(P>0.05);干预后回肠袢式造口组生存质量水平、T淋巴细胞亚群指标优于结肠造口组(P<0.05)。回肠袢式造口组并发症发生率为7.50%,低于结肠造口组的20.00%(P<0.05)。 结论 回肠袢式造口术治疗老年梗阻性乙状结肠癌和高位直肠癌的临床效果优于结肠造口术治疗,可改善预后,对细胞免疫功能影响不大,可缩短手术和排气时间,减少并发症发生率,促进患者生存质量的提升,值得推广。
[关键词] 回肠袢式造口术;结肠造口术;老年梗阻性乙状结肠癌;高位直肠癌
[中图分类号] R735.3 [文献标识码] B [文章编号] 1673-9701(2017)23-0042-03
[Abstract] Objective To analyze the clinical effect of ileal loop colostomy and colostomy in the treatment of obstructive sigmoid colon carcinoma and high rectal cancer. Methods A total of 80 patients with senile obstructive sigmoid colon carcinoma and high rectal cancer from January 2014 to January 2017 were enrolled in this study. They were grouped according to the random number table, with 40 patients in each group. Colostomy group was given colostomy treatment, ileal loop-type colostomy group was treated with ileum loop colostomy treatment. The therapeutic effects, the first exhaust time, the operation time of obstructive sigmoid colon cancer and high rectal cancer between the two groups were compared. The quality of life of patients before and after the intervention, the T lymphocyte subpopulation index and the incidence of complications between the two groups were compared. Results The treatment effect of obstructive sigmoid colon carcinoma and high rectal cancer was 77.50%, higher than that in colostomy group(50.00%) (P<0.05). The first exhaust time and the operation time was(23.51±1.41) h, (54.51±12.61) min respectively, shorter than that of colostomy group[(34.40±2.77) h, (77.40±23.57) min](P<0.05). The quality of life and the T lymphocyte subsets were similar in the two groups before intervention(P>0.05). The level of the quality of life and T-lymphocyte subsets in the ileal loop colostomy group were superior to that of colostomy group after intervention(P<0.05). The incidence of complication was 7.50% in the ileal colostomy group, lower than 20.00% in the colostomy group(P<0.05). Conclusion The clinical effect of ileal loop colostomy in the treatment of obstructive sigmoid colon cancer and high rectal cancer is superior to that of colostomy. And the ileal loop colostomy can improve the prognosis and has little effect on cellular immune function, which can shorten the operation and exhaust time, and can reduce the occurrence of complications. It promotes the quality of life of patients to enhance and is worth promoting.endprint
[Key words] Ileal loop colostomy; Colostomy; Senile obstructive sigmoid colon carcinoma; High rectal cancer
老年梗阻性乙状结肠癌和高位直肠癌发病率高,是常见消化道恶性肿瘤,多数患者就诊时处于晚期,加上慢性疾病多,预后较差[1-2]。目前老年梗阻性乙状结肠癌和高位直肠癌多采用手术方法治疗,但手术术式较多,需选择安全性高、疗效好的术式。回肠袢式造口术与结肠造口术是老年梗阻性乙状结肠癌和高位直肠癌常见术式,为了对比两者的效果,本研究将将2014年1月~2017年1月80例老年梗阻性乙状结肠癌和高位直肠癌患者作为研究对象并根据随机数字表分组,每组40例,探讨回肠袢式造口术与结肠造口术治疗老年梗阻性乙状结肠癌和高位直肠癌的临床效果,现报道如下。
1 资料与方法
1.1 一般资料
选择2014年1月~2017年1月收治的80例老年梗阻性乙状结肠癌和高位直肠癌患者作为研究对象并根据随机数字表分为两组,每组40例。回肠袢式造口组男23例,女17例;年龄61~84岁,平均(69.66±2.92)岁。结肠造口组男24例,女16例;年龄62~84岁,平均(69.91±2.66)岁。两组一般资料差异无统计学意义(P>0.05),具有可比性。
1.2 方法
结肠造口组采用结肠造口术治疗。通过高位直肠癌以及梗阻性乙状结肠癌根治术切除肿瘤后将直肠或远端结肠关闭,在左下腹近侧结肠部位进行单腔造口手术,术后3个月进行Ⅱ期手术将造口闭合。
回肠袢式造口组采用回肠袢式造口术治疗。通过高位直肠癌以及梗阻性乙状结肠癌根治术切除肿瘤,给予全肠灌洗,吻合降结肠直肠端,在距离回盲肠部20 cm左右作回肠袢式造口术,术后3个月进行Ⅱ期手术将造口闭合。
所有患者术后给予抗感染、补充水电解质、禁食、胃肠减压、营养支持等处理,在肠功能恢复正常后给予流质饮食[3-4]。
1.3观察指标
比较两组梗阻性乙状结肠癌和高位直肠癌治疗效果;第一次排气时间、手术时间;干预前后患者生存质量水平(根据SF-36量表进行评估,包括8个维度36个问题,总分100分,分数越高代表生存质量越高)[5]、T淋巴细胞亚群指标。
根据实体瘤疗效标准进行分级,分为完全缓解、部分缓解、稳定、进展四个级别,其中总有效率为完全缓解、部分缓解的百分比之和[6]。
1.4 统计学方法
采用SPSS12.0统计学软件处理数据,计量资料、计数资料的比较分别采用t检验、χ2检验,P<0.05表示差异有统计学意义。
2 结果
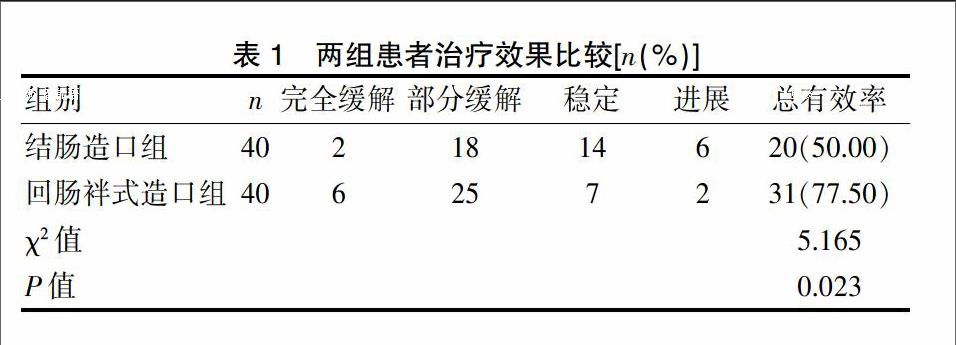
2.1 两组患者治疗效果比较
回肠袢式造口组梗阻性乙状结肠癌和高位直肠癌治疗总有效率为77.50%,高于结肠造口组的50.00%,差异有统计学意义(P<0.05)。见表1。
2.2两组患者干预前后生存质量水平、T淋巴细胞亚群指标比较
干预前两组生存质量水平、T淋巴细胞亚群指标相近(P>0.05);干预后回肠袢式造口组生存质量水平、T淋巴细胞亚群指标优于结肠造口组(P<0.05)。见表2。
2.3两组患者第一次排氣时间、手术时间比较
回肠袢式造口组第一次排气时间、手术时间分别为(23.51±1.41)h、(54.51±12.61) min,短于结肠造口组的(34.40±2.77)h、(77.40±23.57)min,差异有统计学意义(P<0.05),见表3。
2.4两组并发症发生率比较
回肠袢式造口组并发症发生率(7.50%)低于结肠造口组(20.00%),P<0.05。见表4。
3 讨论
回肠袢式造口术和结肠造口手术均是老年梗阻性乙状结肠癌和高位直肠癌的有效术式,但关于何种术式更安全有效目前仍存在争议[7-10]。但相对于结肠造口手术而言,回肠袢式造口术手术操作简便且创伤小,还纳简单,并发症少,术后康复快,可降低脓毒症和造口脱垂发生风险,对机体免疫功能影响小,可更好地改善患者生活质量[11-15]。
本研究中,结肠造口组采用结肠造口术治疗,回肠袢式造口组回肠袢式造口术治疗。结果显示,回肠袢式造口组梗阻性乙状结肠癌和高位直肠癌治疗总有效率为77.50%,高于结肠造口组的50.00%(P<0.05),说明回肠袢式造口术治疗老年梗阻性乙状结肠癌和高位直肠癌的临床效果优于结肠造口术治疗,这可能和回肠袢式造口术可减少造口脱垂和脓毒症等优势相关。
回肠袢式造口组第一次排气时间、手术时间分别为(23.51±1.41)h、(54.51±12.61)min,短于结肠造口组的(34.40±2.77)h、(77.40±23.57)min,差异有统计学意义(P<0.05),说明回肠袢式造口术操作更为简单,可缩短手术时间,减少对胃肠道功能的影响,加速术后胃肠道功能恢复。
干预前两组生存质量水平、T淋巴细胞亚群指标相近(P>0.05);干预后回肠袢式造口组生存质量水平、T淋巴细胞亚群指标优于结肠造口组(P<0.05),说明回肠袢式造口术可有效提升机体免疫力,促进患者生活质量的提高,而这和术后并发症少,恢复快等相关。
回肠袢式造口组并发症发生率为7.50%,低于结肠造口组的20.00%(P<0.05),说明回肠袢式造口术具有更高的安全性和微创性,可减少不良事件的发生。
陈建新、乔建国[14]的研究中按照手术方式的不同分为实验组46例和对照组40例,实验组患者采用回肠袢式造口术,对照组患者采用结肠造口术,结果显示,实验组患者的手术时间以及术后的排气时间、禁食时间、住院时间均明显低于对照组患者(P<0.05),且低血钾症的发生率也显著低于对照组患者(P<0.05),也说明回肠袢式造口术治疗老年梗阻性乙状结肠癌和高位直肠癌患者的临床效果更加显著,具有更高的安全性,和我们的研究结果相似。王兴国等[15]的研究也证实了回肠袢式造口术治疗老年梗阻性乙状结肠癌和高位直肠癌的临床效果优于结肠造口术。endprint
综上所述,回肠袢式造口术治疗老年梗阻性乙状结肠癌和高位直肠癌的临床效果优于结肠造口术治疗,可改善预后,对细胞免疫功能影响不大,可缩短手术和排气时间,减少并发症发生,促进患者生存质量提升,值得推广。
[参考文献]
[1] Serrurier K,Liu J,Breckler F,et al.A multicenter evaluation of the role of mechanical bowel preparation in pediatric colostomy takedown[J].Journal of Pediatric Surgery:Official Journal of the Surgical Section of the American Academy of Pediatric,the British Association of Paediatric Surgeons,the American Pediatric Surgical Association,and the Canadian Association of Paediatric Surgeons,2012,47(1):190-193.
[2] 金灵莉,周春芳,吕飞,等.结肠造口和回肠袢式造口术对老年梗阻性乙状结肠癌的疗效对比[J].实用癌症杂志,2016,31(10):1672-1674.
[3] Oda O,Davies D,Colapinto K,et al.Loop versus divided colostomy for the management of anorectal malformations[J].Journal of Pediatric Surgery:Official Journal of the Surgical Section of the American Academy of Pediatric,the British Association of Paediatric Surgeons,the American Pediatric Surgical Association,and the Canadian Association of Paediatric Surgeons,2014,49(1):87-90.
[4] 刘传渊,刘红权,肖荷芳,等.两种肠造口术对老年梗阻性乙状结肠癌和高位直肠癌的治疗效果探讨[J].当代医学,2016,22(34):18-19.
[5] 周皎琳,邱辉忠,林国乐,等.结直肠吻合的预防性造口术——袢式横结肠造口与袢式回肠造口的比较[J].中国现代手术学杂志,2011,15(1):65-68.
[6] VanDenHondel D,Sloots C,Meeussen C,et al.To split or not to split:Colostomy complications for anorectal malformations or hirschsprung disease:A single center experience and a systematic review of the literature[J].European journal of pediatric surgery=Zeitschrift fur Kinderchirurgie,2014,24(1):61-69.
[7] 张志泉,孙立征,刘学武,等.回肠袢式造口术与结肠造口术对老年结直肠癌中的疗效及安全性对比[J].实用癌症杂志,2016,31(5):798-800.
[8] 彭永红,喻学桥,周卫平,等.回肠袢式造口术和结肠造口术对老年左侧结直肠癌患者的临床疗效比较[J].中华普外科手术学杂志(电子版),2016,10(2):127-129.
[9] Jang HW,Kim YN,Nam CM,et al.Factors affecting colonoscope insertion time in patients with or without a colostomy after left-sided colorectal resection[J]. Digestive Diseases and Sciences,2012,57(12):3219-3225.
[10] 白景舒,辛革,王楠,等.两种术式治疗结肠癌患者的临床疗效及血清胃泌素、肝细胞生长因子变化水平比较[J].医学综述,2016,22(2):377-380.
[11] 曹超.结肠造口术与回肠袢式造口术治疗老年梗阻性乙状结肠癌及高位直肠癌[J].世界临床医学,2016,10(3):47,50.
[12] Zhang JE,Wong FKY,You LM,et al.Effects of enterostomal nurse telephone follow-up on postoperative adjustment of discharged colostomy patients[J].Cancer nursing,2013,36(6):419-428.
[13] 王龙安.两种肠造口术治疗老年梗阻性乙状结腸癌和高位直肠癌60例的临床观察[J].中国实用医药,2015, 10(31):54-55.
[14] 陈建新,乔建国.两种肠造口术对老年梗阻性乙状结肠癌和高位直肠癌的疗效比较[J].实用癌症杂志,2015, 30(8):1197-1199.
[15] 王兴国,李冠雄,杨中民,等.回肠袢式造口术和结肠造口术治疗老年梗阻性乙状结肠癌和高位直肠癌的临床对比观察[J].临床和实验医学杂志,2016,15(15):1525-1529.
(收稿日期:2017-06-16)endprint
