河南省直公务员缺血性心血管病发病危险度评估
2017-09-08滕军燕魏艳萍苏丰鸣郭智萍陈利国河南省骨科医院河南郑州45008河南省人民医院保健办公室河南郑州45000郑州市紧急医疗救援中心河南郑州45008
滕军燕 魏艳萍 苏丰鸣 郭智萍 陈利国(.河南省骨科医院 河南 郑州 45008;.河南省人民医院 保健办公室 河南 郑州 45000;.郑州市紧急医疗救援中心 河南 郑州 45008)
·论 著·
河南省直公务员缺血性心血管病发病危险度评估
滕军燕1魏艳萍2苏丰鸣3郭智萍1陈利国1
(1.河南省骨科医院 河南 郑州 450018;2.河南省人民医院 保健办公室 河南 郑州 450003;3.郑州市紧急医疗救援中心 河南 郑州 450018)
目的 了解河南省直公务员心血管病危险因素现状,评估该群体10年缺血性心血管病(ischemic cardiovascular diseases, IVCD)发病危险度。方法 采用分层随机抽样方法,抽取2 211名35~59岁河南省直在职公务员体检报告,进行补充调查;对抽取人员进行心血管病危险因素现状调查分析,并使用“国人IVCD 10年发病危险度评估表”简易模型进行危险度评估。结果 在体质量指数(BMI)、血脂、血压、糖尿病、吸烟5个危险因素方面,不同性别、年龄组间差异均有统计学意义,且男性健康状况差于女性;血脂异常和糖尿病发生率随年龄增长而升高。两性ICVD绝对危险度平均值均随年龄增加而增加,各年龄组两性间差异有统计学意义(P<0.05);男性绝对危险度<10%的占94.1%,≥10%的占5.9%;女性绝对危险度<10%的占96.8%,≥10%的占3.2%;危险度分布在不同性别、年龄组间差异有统计学意义(P<0.05)。ICVD各主要危险因素在绝对危险度≥10%和<10%的两组间比较, 差异均有统计学意义(P<0.05)。结论 河南省直公务员ICVD发病危险度处于较高水平,建议在公务员队伍中开展有效的健康管理。ICVD评估方法适用于高危人群筛查,但在指标得分的权重上有待于进一步的权衡和完善。
公务员;心血管疾病;危险因素;危险评估
发展中国家心血管疾病的流行病学特点已逐渐与发达国家相近[1]。心血管疾病的发病率和死亡率在全球范围中占首位[2-3],也是我国死亡的首要原因,中国每年约300万人死于心血管疾病[4]。与其他国家不同的是,我国以缺血性心血管病(ischemic cardiovascular diseases,ICVD)为主,其与年龄、性别、血压、血清总胆固醇、体质量指数(BMI)、吸烟和糖尿病有显著关联,且高胆固醇血症和高血压对增加心血管病的死亡率有协同作用[5-13]。因此,危险因素有所偏重的不同群体其缺血性心血管病的发病危险有差异。
公务员是一个特殊群体,著名的白厅研究表明,冠心病与工作性质和阶层有关,公务员是冠心病的高发群体[14-16]。中国公务员也面临着逐渐严重的健康问题,工作压力大等情况影响着他们的健康状况[17-18]。有研究表明,中国公务员慢性疾病的发病率呈上升趋势,且发病率高于普通居民[19-20]。但是,针对公务员群体缺血性心血管病发病风险的评估却较少。本研究将对2 400名河南省直公务员进行心血管病危险因素现状调查及缺血性心血管疾病10年发病风险评估,以探讨影响公务员心血管健康的主要原因和可改善的方法。
1 对象与方法
1.1 研究对象 从2015年在河南省人民医院体检的65个省直单位中采用分层随机抽样的方法抽取35~59岁的2 400名公务员进行调查。排除已确诊冠心病、脑卒中的人员,有效调查2 211名,有效入选率92.13%。
1.2 调查方法 调查表标准统一,且对调查员进行培训。调查内容包括人口学数据信息(性别、年龄、单位),生活方式(吸烟和饮酒),病史(糖尿病、冠心病、脑卒中等)和体格检查(血压、BMI、血脂、空腹血糖等)。血脂和血糖实验室检查采用瑞士罗氏试剂(罗氏诊断公司,德国曼海姆, Sandhofer街116、68305)。
1.3 诊断标准 高脂血症:总胆固醇>5.17 mmol/L,甘油三酯>1.46 mmol/L和低密度脂蛋白>3.1 mmol/L[21]。高血压:在未使用降压药物的情况下,收缩压≥140 mm Hg和(或)舒张压≥90 mm Hg。糖尿病:有糖尿病症状,且空腹血糖≥7.0 mmol/L或非空腹血糖≥11.1 mmol/L[22]。无典型糖尿病症状,则至少2次空腹血糖≥7.0 mmol/L或非空腹血糖≥11.1 mmol/L[23]。BMI异常: BMI=体质量/身高2(kg/m2),BMI 24.0~27.9为超重,BMI≥28为肥胖[24]。吸烟:参考世界卫生组织推荐的吸烟标准,每天吸烟1支以上,连续1个月以上为吸烟[25]。
1.4 危险因素分组与危险度分级 采用“国人ICVD 10年发病危险评估方法”简易模型计算缺血性心血管病绝对危险度[26-27]。见图1、图2。
根据模型要求,设定6个变量并分组。①年龄:每5岁为1个年龄组,分为35~39岁、40~44岁、45~49岁、50~54岁、55~59岁,共5组;②收缩压:分为<120 mm Hg、120~129 mm Hg、130~139 mm Hg、140~159 mm Hg、160~179 mm Hg、≥180 mm Hg,共6组;③BMI:分为<24 kg/m2、24~27.9 kg/m2、≥28 kg/m2,共3组;④总胆固醇(mmol/L):分为<5.20 mmol/L和≥5.20 mmol/L两组;⑤吸烟:分为是、否两组;⑥糖尿病:分为是、否两组。
按照性别,计算所有研究对象6种危险分层的总得分,并计算出绝对危险(%):≤5为极低危,5.1~9.9为低危,10~19.9为中危,20~39.9为高危,以≥40为极高危,≥10即中危以上为异常。

图2 ICVD 10年发病危险度评估量表(女)
1.5 统计学分析 使用Epidata 3.02建立数据库,数据采用双核对方法录成,导入IBM SPSS 22.0统计软件中处理。其中河南省直公务员心血管危险因素分布情况和公务员ICVD 10年发病绝对危险度分布采用描述性统计方法,不同性别公务员心血管病危险因素暴露情况对比采用独立样本t检验,不同性别、年龄ICVD 10年发病绝对危险均值比较采用方差分析,绝对危险度<10%和≥10%两个人群心血管危险因素暴露率比较采用四格表χ2检验,采用单样本t检验。P<0.05表示差异有统计学意义。
2 结果
2.1 基本情况 35~59岁河南省直在职公务员共2 211名,男1 468名(66.40%),女743名(33.60%),平均(48.09±6.99)岁。不同性别公务员在年龄、BMI、抽烟、糖尿病、总胆固醇、收缩压方面的分布情况见表1。
2.2 心血管病危险因素暴露情况 受调公务员在超重和肥胖、高脂血症、高血压、糖尿病和吸烟等5个方面的暴露率分别为62.96%、76.07%、34.87%、8.10%和21.30%。男性公务员以上5个危险因素的暴露率均高于女性,差异有统计学意义(P<0.05)。见表2。不同年龄组以上5个危险因素的暴露率比较,差异有统计学意义(P<0.05)。血脂异常和糖尿病发生率有随年龄增长而升高的趋势。见表3。
2.3 ICVD 10年发病风险评估
2.3.1 不同性别、年龄10年ICVD发病绝对危险均值 男性10年ICVD发病绝对危险值为(3.88±5.19)%,女性为(1.68±3.00)%,差异有统计学意义(t=113.910,P=0.000)。两性公务员ICVD 10年发病绝对危险均值均随年龄增长而升高;男性公务员除35~39岁、40~44岁间差异无统计学意义外,其他两组间差异均有统计学意义(P<0.05);女性公务员50~54岁、55~59岁组与其他年龄组相比,差异均有统计学意义(P<0.01)。各年龄组,男性公务员绝对危险值均高于女性,差异有统计学意义(P<0.05)。见表4。
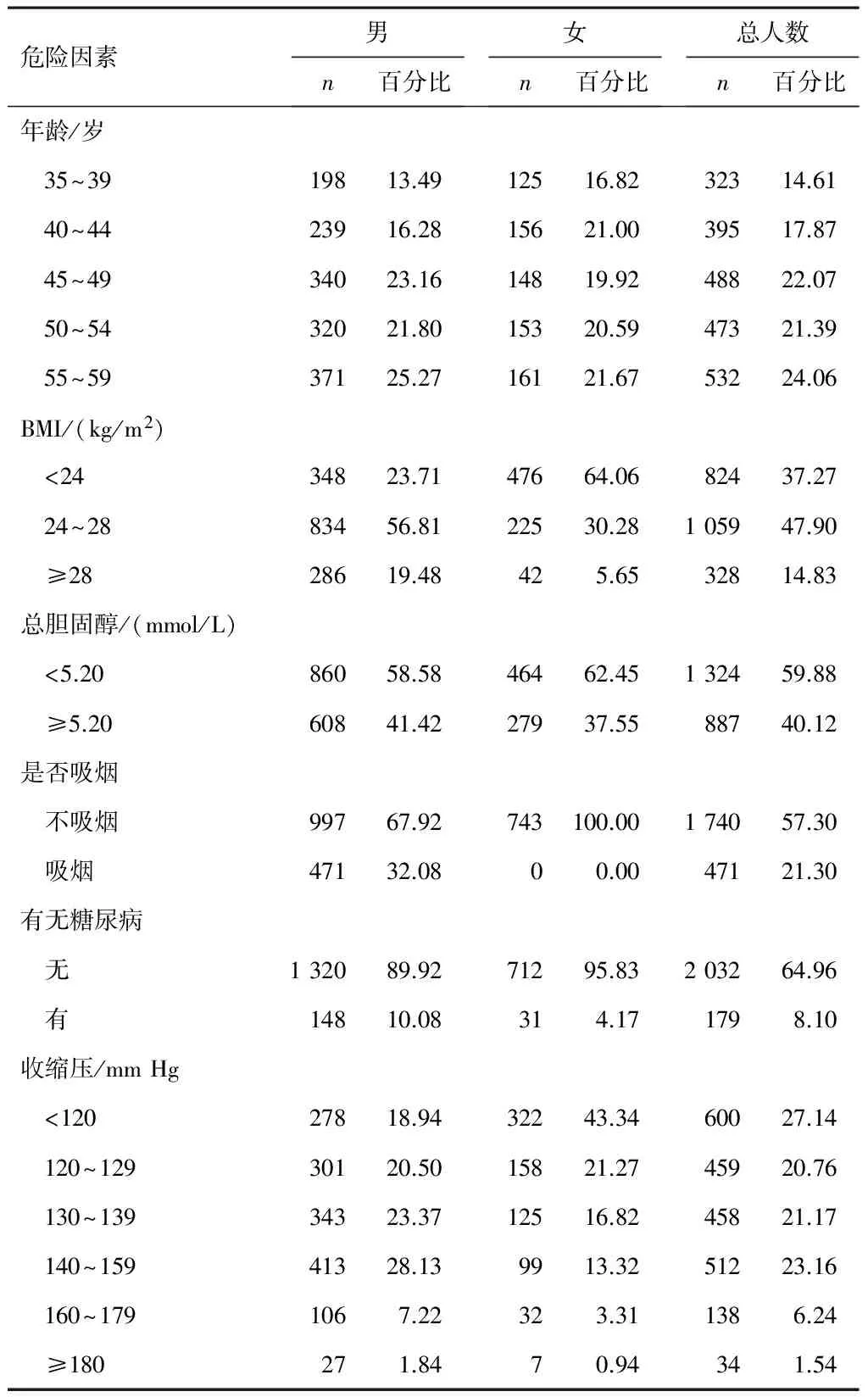
表1 河南省直公务员心血管危险因素分布情况(n,%)

表2 河南省直不同性别公务员心血管病危险因素暴露情况[n(%)]
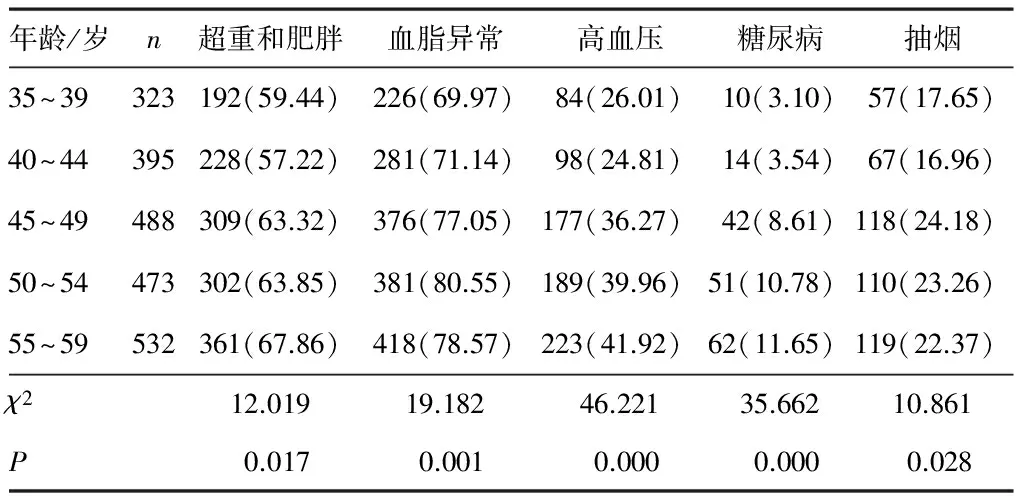
表3 河南省直不同年龄公务员心血管病危险因素暴露情况[n(%)]
表4 河南省直公务员不同性别、年龄ICVD 10年发病绝对危险值
注:与同性别其他组比较,aP<0.05;与同性别其他组比较,bP<0.01。
2.3.2 ICVD 10年发病绝对危险度分布 2 211名公务员绝对危险度由极低危到极高危的比重分别为82.27%、12.75%、3.17%、1.63% 和0.18%。其中,男性公务员中危以下的占94.1%(1 382名),中危及以上占5.9%(86名);女性公务员中危以下的占96.8%(719名),中危及以上占3.2%(24名);不同性别间差异有统计学意义(χ2=109.150,P=0.000)。各年龄组间差异有统计学意义(χ2=287.596,P=0.000)。见表5。
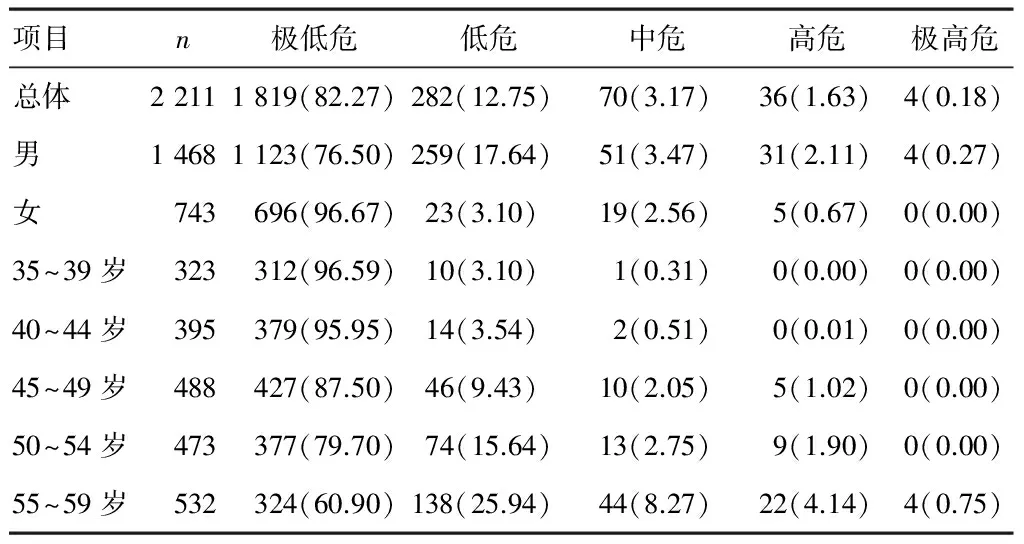
表5 河南省直公务员ICVD 10年发病绝对危险度分布[n(%)]
2.3.3 不同绝对危险度人群主要危险因素发生情况 ICVD 10年发病绝对危险度<10%和≥10%的人群在高收缩压、高总胆固醇、超重和肥胖、吸烟和糖尿病等方面的发生率比较,差异均有统计学意义(P<0.05)。见表6。

表6 不同危险度人群的心血管病危险因素暴露情况[n(%)]
2.3.4 不同性别绝对危险度评估 男性公务员35~39岁、40~44岁、45~49岁、50~54岁、55~59岁组ICVD 10年发病绝对危险较该年龄段一般人群和低危人群分别净增(0.53%、1.23%)、(0.46%、1.46%)、(1.40%、2.80%)、(1.64%、3.54%)、(3.64%、5.64%),分别是一般人群和低危人群的(1.53、5.10)、(1.33、4.65)、(1.74、6.60)、(1.63、6.06)、(1.84、6.64)倍。女性公务员各年龄组ICVD 10年发病绝对危险较一般人群和低危人群分别净增(0.04%、0.24%)、(0.12%、0.42%)、(0.37%、0.77%)、(1.29%、1.89%)、(2.61%、3.51%),分别是一般人群和低危人群的(1.13、3.40)、(1.30、5.20)、(1.62、4.85)、(2.43、7.30)、(2.86、8.02)倍。见表7。
3 讨论
本研究调查了河南省直公务员缺血性心血管疾病10年发病风险情况和心血管病危险因素暴露情况。结果表明,公务员缺血性心血管病危险因素暴露率和发病风险远高于普通居民。其中,男性公务员健康状况明显差于女性,其在超重和肥胖、高脂血脂、高血压、糖尿病上的检出率均高于女性,且有32.08%的男性公务员抽烟。其中,高血压和糖尿病的发生率和年龄相关,而超重、抽烟、高胆固醇和年龄没有相关性,因此,考虑缺血性心血管疾病的危险因素与生活方式相关。45岁后的女性公务员危险评分明显大于普通居民,这一结果提示,有必要对不同性别和年龄的公务员采取针对性的健康管理。在以前的研究中发现,收入和教育史与急性心肌梗死等心血管疾病呈负相关[22],公务员作为社会的中上等阶层,收入和教育程度较好,但是为何其ICVD风险较高?其中原因有必要进一步研究。
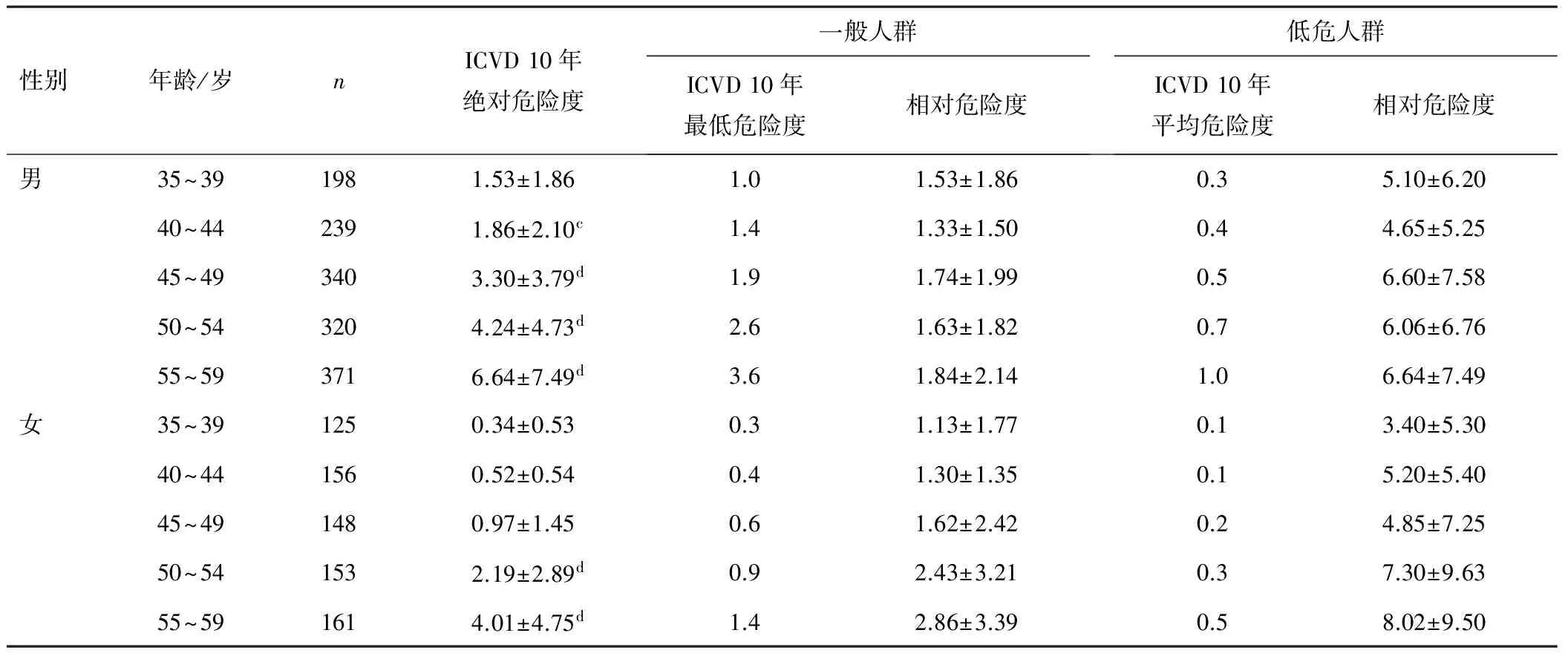
表7 河南省直不同性别、年龄公务员ICVD 10年绝对危险度评估(%)
注:与其他组比较,cP<0.05;与其他组比较,dP<0.01。
使用“国人缺血性心血管病10年发病危险度评估表”对不同性别公务员进行评估的结果显示,绝对危险度有随年龄增长而增长的趋势,男性在各个年龄组的绝对危险度平均值都高于女性,且差异有统计学意义。两性公务员各年龄组的平均绝对危险度均高于一般人群。这表明河南省公务员整体的缺血性心血管病发病危险度要高于同年龄段的普通居民,应该引起政府和卫生防控部门的足够重视。
在ICVD 10年发病绝对危险度≥10%的公务员人群中,高收缩压发生率为99.10%、超重和肥胖发生率为95.45%。有研究表明,高脂血症等其他心血管病危险因素与超重和肥胖之间有明确的流行病学关系[28-30],本研究中,血压和BMI对ICVD 10年发病风险中危以上人群影响更大,有研究表明,超重和肥胖能够显著增加人们患心血管病的风险;肥胖和高血压患者与正常人相比,患冠心病的风险增加2~3倍,猝死风险增加7倍;但是减肥却能够有效降低总胆固醇[28,31-32]。因此,降低该人群的发病风险应该着重从控制血压、控制体质量入手。有研究表明,吸烟属冠心病全球最强的危险预测因素[33],ICVD中除年龄的其他5个危险因素同时存在,可预测80%的急性冠脉综合征,而每天>1支烟即可增加40%的急性心肌梗死发生率[34],单纯持续吸烟即可预测36%的急性心肌梗死[35]。ICVD 10年发病绝对危险度<10%的人群中,仍有20.03%的人抽烟,在评估的模型中是否降低了吸烟的得分比重,该模型是否未包含反映受调个体心血管危险因素的重要影响因素,有待于进一步研究。
本研究对象为在职公务员,调查人群的ICVD 10年发病绝对危险度显著高于评估参考标准,因此,该评估办法可以应用于公务员这一群体。及时发现缺血性心血管病的高危个体,做到早期预防并进行科学的健康管理干预,能有效降低心脑血管疾病的发病率,对于保证政府人力资源的可持续发展具有深远意义。
综上所述,公务员存在ICVD的高发生风险,改善生活方式和个性化健康管理能够减少与发病相关的危险因素,从而减少心血管疾病的发病率和死亡率。这项研究也为进一步探索ICVD相关发病风险预测模型提供了基础。
[1] Celermajer D S,Chow C K,Marijon E,et al.Cardiovascular disease in the developing world: prevalences,patterns,and the potential of early disease detection[J].J Am Coll Cardiol,2012,60(14):1207-1216.
[2] Mathers C D,Loncar D.Projections of global mortality and burden of disease from 2002 to 2030[J].PLoS Med,2006,3(11):e442.
[3] Roger V L,Go A S,Lloyd-Jones D M,et al.Heart disease and stroke statistics--2012 update: a report from the American Heart Association[J].Circulation,2012,125(1):e2-e220.
[4] Cheng T O.Cardiovascular health,risks and diseases in contemporary China[J].Int J Cardiol,2012,154(2):233-242.
[5] Di Iorio B,Di Micco L,Torraca S,et al.Variability of blood pressure in dialysis patients: a new marker of cardiovascular risk[J].J Nephrol,2013,26(1):173-182.
[6] Hadaegh F,Mohebi R,Khalili D,et al.High normal blood pressure is an independent risk factor for cardiovascular disease among middle-aged but not in elderly populations: 9-year results of a population-based study[J].J Hum Hypertens,2013,27(1):18-23.
[7] Danaei G,Lawes C M,Vander Hoorn S,et al.Global and regional mortality from ischaemic heart disease and stroke attributable to higher-than-optimum blood glucose concentration: comparative risk assessment[J].Lancet,2006,368(9548):1651-1659.
[8] Chen J H,Pan W H,Hsu C C,et al.Impact of obesity and hypertriglyceridemia on gout development with or without hyperuricemia:a prospective study[J].Arthritis care Res,2013,65(1):133-140.
[9] Li M,Hou W,Zhang X,et al.Hyperuricemia and risk of stroke: a systematic review and meta-analysis of prospective studies[J].Atherosclerosis,2014,232(2):265-270.
[10]Lloyd-Jones D M,Goff D C, Stone N J.Guidelines for cardiovascular risk assessment and cholesterol treatment[J].Jama,2014,311(21):2235.
[11]Wen C P,David Cheng T Y,Tsai S P,et al.Are Asians at greater mortality risks for being overweight than Caucasians? Redefining obesity for Asians[J].Public Health Nutr,2009,12(4):497-506.
[12]Yang Y,Li J X,Chen J C,et al.Effect of elevated total cholesterol level and hypertension on the risk of fatal cardiovascular disease:a cohort study of Chinese steelworkers[J].Chin Med J,2011,124(22):3702-3706.
[13]Harvey P R,Holt A,Nicholas J,et al.Is an average of routine postdialysis blood pressure a good indicator of blood pressure control and cardiovascular risk?[J].J Nephrol,2013,26(1):94-100.
[14]Guimaraes J M,Werneck G L,Faerstein E,et al.Early socioeconomic position and self-rated health among civil servants in Brazil:a cross-sectional analysis from the Pro-Saude cohort study[J].BMJ open,2014,4(11):e005321.
[15]Ferrie J E,Martikainen P,Shipley M J,et al.Employment status and health after privatisation in white collar civil servants: prospective cohort study[J].BMJ,2001,322(7287):647-651.
[16]Ferrie J E,Shipley M J,Stansfeld S A,et al.Effects of chronic job insecurity and change in job security on self reported health,minor psychiatric morbidity,physiological measures,and health related behaviours in British civil servants:the Whitehall II study[J].J Epidemiol Community Health,2002,56(6):450-454.
[17]Brunner E J,Marmot M G,Nanchahal K,et al.Social inequality in coronary risk: central obesity and the metabolic syndrome.Evidence from the Whitehall II study[J].Diabetologia,1997,40(11):1341-1349.
[18]Tchicaya A,Braun M,Lorentz N,et al.Social inequality in awareness of cardiovascular risk factors in patients undergoing coronary angiography[J].Eur J Prev Cardiol,2013,20(5):872-879.
[19]Li Y H,Yang C,Pang J,et al.Study on lifestyle and self-rated health among 5 kinds of occupational populations in 6 provinces in China[J].Zhonghua yu fang yi xue za zhi,2012,46(3):214-219.[20]Zhu C L,Ou L,Geng Q,et al.Relationships of Mental Health Problems with Stress Among Civil Servants in Guangzhou,China[J].Community Ment Health J,2014,50(8):991-996.
[21]Stone N J,Robinson J G,Lichtenstein A H,et al.2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults:a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines[J].J Am Coll Cardiol,2014,63(25 Pt B):2889-2934.
[22]James P A,Oparil S,Carter B L,et al.2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8)[J].Jama,2014,311(5):507-520.
[23]Frei A,Chmiel C,Schläpfer H,et al.The Chronic CARe for diAbeTes study (CARAT): a cluster randomized controlled trial[J].Cardiovasc Diabetol,2010,15(9):23.
[24]Wu Y.Overweight and obesity in China[J].BMJ,2006,333(7564):362-363.
[25]McClave A K,McKnight-Eily L R,Davis S P,et al.Smoking characteristics of adults with selected lifetime mental illnesses: results from the 2007 National Health Interview Survey[J].Am J Public Health,2010,100(12):2464-2472.
[26]Zhou B L,Stamler J,Tao S,et al.Relation of occupational change to cardiovascular risk factor levels in rural Chinese men:the people’s republic of China-United States Collaborative Study on cardiovascular and cardiopulmonary epidemiology[J].Am J Public Health,2003,93(12):2049-2051.
[27]Wu Y.A study on evaluation of the risk of ischemic cardiovascular diseases in Chinese and the development of simplified tools for the evaluation[J].Chin J Cardiol,2002,31(12):893-901.
[28]Grundy S M.Atherosclerosis imaging for risk assessment and primary prevention of cardiovascular disease[J].Prog Cardiovascular Dis,2003,46(2):115-121.
[29]Klose G,Beil F U,Dieplinger H,et al.New AHA and ACC guidelines on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk:statement of the D·A·CH society for prevention of cardiovascular diseases,the Austrian atherosclerosis society and the working group on lipids and atherosclerosis (AGLA) of the Swiss society for cardiology[J].Internist,2014,55(5):601-606.
[30]Guo J,Wang Y,Chen T,et al.Influence of socioeconomic status on acute myocardial infarction in the Chinese population:the interheart China study[J].Chin Med J (Engl),2012,125(23):4214-4220.
[31]Xie S,Wang J,Li N,et al.Survey on overweight and obesity of preschool children in rural areas from ten provinces of China[J].Zhonghua liu xing bing xue za zhi,2014,35(4):425-428.
[32]Teramoto T,Sasaki J,Ishibashi S,et al.Cardiovascular disease risk factors other than dyslipidemia.Executive summary of the Japan Atherosclerosis Society (JAS) guidelines for the diagnosis and prevention of atherosclerotic cardiovascular diseases in Japan-2012 version[J].J Atheroscler Thromb,2013,20(10):733-742.
[33]Qin R,Chen T,Lou Q,et al.Excess risk of mortality and cardiovascular events associated with smoking among patients with diabetes: meta-analysis of observational prospective studies[J].Int J Cardiol,2013,167(2):342-350.
[34]Steele L,Lloyd A,Fotheringham J,et al.A retrospective cross-sectional study on the association between tobacco smoking and incidence of ST-segment elevation myocardial infarction and cardiovascular risk factors[J].Postgrad Med J,2015,91(1079):492-496.
[35]Yano Y,Hoshide S,Shimada K,et al.The impact of cigarette smoking on 24-hour blood pressure,inflammatory and hemostatic activity,and cardiovascular risk in Japanese hypertensive patients[J].J Clin Hypertens,2013,15(4):234-240.
Pathogenesis risk assessment of ischemic cardiovascular in Henan provincial civil servents
Teng Junyan1, Wei Yanping2, Su Fengming3, Guo Zhiping1, Chen Liguo1
(1.OrthopedicHospitalofHenanProvince,Zhengzhou450018,China; 2.HenanProvincePeople'sHospital,Zhengzhou450003,China; 3.EmergencyMedicalRescueCenterofZhengzhouCity,Zhengzhou450018,China)
Objective To understanding the cardiovascular disease risk factors in Henan provincial civil servant status, and assess the ischemic cardiovascular diseases (ICVD) risk of this group in decade. Methods The medical reports of 2 211 Henan provincial civil servants from 35 to 59 years old were extracted by stratified random sampling method and carried out the supplementary investigation. The current situation of the risk factors of cardiovascular disease in the target group was investigated and assess the risk under the assessment model of “Chinese ICVD risk assessment table in decade”. Results In the 5 risk factor of BMI, blood lipids, blood pressure, diabetes and smoking, there were significant differences between genders, age groups and worse health status found in male group. Dyslipidemia and diabetes incidence increases with age. Gender ICVD absolute average risk increases with age, and there was significant differences between the male and female of all age groups (P<0.05). Male absolute risk less than 10% accounted for 94.1%, greater or equal to 10% occupied 5.9%. Female absolute risk less than 10% accounted for 96.8%, greater than or equal to 10% occupied 3.2%. Risk distribution between different genders, age groups was statistically significant difference(P<0.05). The comparison of the principal risk factor between the two group of ICVD absolute risk greater than or equal to 10% and less than 10%, there was statistically significant differences(P<0.05). Conclusion ICVD risk of Henan provincial civil servants is at a high level. It is recommended that effective health management in the civil service. ICVD assessment method is suitable for screening for high risk population, but which need further developed and weighed on the index score.
civil servant; cardiovascular diseases; risk factors; risk assessment
河南省科技厅科技攻关项目(152102310142);河南省医学科技攻关项目(201403171);河南省哲学社会科学规划项目(2015BSH023);河南省科技厅软科学项目(122400450432)。
魏艳萍, E-mail:wei-yp1234@163.com。
R 54
10.3969/j.issn.1004-437X.2017.16.001
2017-03-16)
