髋关节直接前入路切口远端延长相关应用解剖学研究
2017-05-15李斌蔡宁宇史旭超潘天龙潘骏
李斌 蔡宁宇 史旭超 潘天龙 潘骏
髋关节直接前入路切口远端延长相关应用解剖学研究
李斌 蔡宁宇 史旭超 潘天龙 潘骏
目的 为髋关节直接前入路远端延长及其易损伤结构提供解剖学依据。方法 参照手术入路层次对10个成年尸体下肢标本相关结构和重要的神经血管进行解剖观测。 结果 股外侧皮神经外侧支与切口线的距离在X1、X2、X3线平面上分别为(0.61±0.39)、(-0.65±0.39)、(-0.10±0.32)cm,股外侧皮神经内侧支与切口线的距离在X1、X2、X3线平面上分别为(1.53±0.52)、(0.67±0.56)、(1.28±0.56)cm。旋股外侧动脉各分支(升支、横支、降支)与切口线的交点与髂前上棘(ASIS)的距离分别为(7.77± 0.79)、(11.01±1.48)、(14.91±1.48)cm,旋股外侧动脉各分支(升支、横支、降支)与切口线的交点与X1线平面的距离分别为(0.48± 0.58)、(4.99±1.18)、(7.35±1.07)cm。股神经股外侧肌支分支(最上支、最下支)入肌点与ASIS的距离分别为(11.26±0.96)、(15.09±1.74)cm,股神经股外侧肌支分支(最上支、最下支)入肌点与X1线的距离分别为(4.70±2.09)、(7.71±1.45)cm。 结论转子间线的远端是许多神经分支的入点,髋关节直接前入路切口的远端延长不应超过大转子平面以下1.1cm。
髋关节 直接前入路 远端延长 应用解剖学
髋关节直接前入路改良于Smith-Peterson入路及Heuter入路,其实是一种改良的单切口Smith-Peterson入路,它利用阔筋膜张肌、股直肌及缝匠肌之间的肌间隙直达髋关节,是一种真正从肌间隙进入的微创入路,具有对肌肉保护较好、不易损伤运动神经、假体位置好、术后脱位率低、康复快等优势[1-7]。然而有文献报道采用这种入路手术时可发生股骨骨折、内植物植入失败、肌肉损伤等术中并发症[8-14],预防这些并发症需要延长手术入路的远端。该入路近端延长至阔筋膜张肌和臀中小肌在骨盆上的附着点,它属于Smith-Peterson入路一部分,远端延长会损伤神经血管束。本研究的目的是通过尸体解剖,观测髋关节前入路远端延长时的血管神经分布,为临床手术及术中处理有关结构提供解剖学资料。
1 材料和方法
1.1 标本 成年尸体(男4具,女2具)下肢标本10个(4个成对的和2个不成对的),均由温州医科大学解剖教研室提供,标本血管均已用红色染料灌注。
1.2 方法 标本取仰卧位,分别触及髂前上棘(ASIS)和耻骨结节并予以标记。为了扩大视野,切口从髂嵴顶端开始,沿着髂骨边缘直至ASIS,继而沿着腓骨头方向向下延长,切口长度大约25cm。移除皮肤和皮下组织,分离出股外侧皮神经的内侧支和外侧支,观察这些神经分支走形规律。在腹股沟韧带水平解剖出股神经、股动静脉。髋关节前入路沿着阔筋膜张肌前缘延长,并且保持与股直肌外侧缘平行。平行于缝匠肌和股直肌边缘,仔细解剖出支配股外侧肌、股中间肌、股直肌、缝匠肌的股神经分支和旋股外侧动脉分支。从股外侧肌上移除阔筋膜张肌。记录下每条神经的入肌点,测量它们与大转子、ASIS的距离。观察股神经分支在股外侧肌、股中间肌内的走形。
1.3 统计学处理 采用SPSS 23.0统计软件,计量资料以表示。
2 结果
2.1 股外侧皮神经 股外侧皮神经主干从腰大肌外侧缘发自腰丛,沿髂腰肌表面下行,在ASIS内侧深筋膜深面分为股外侧皮神经前支和后支,经腹股沟韧带深面进入大腿,由阔筋膜深面穿入阔筋膜局部分为两层所围成的筋膜鞘中,股外侧皮神经前支分出的内侧支、外侧支以及股外侧皮神经后支分别走在各自的深筋膜鞘中,其间神经周围伴随着丰富的脂肪组织,它们的行径与髋关节手术前切口几乎平行或重合(图1)。股外侧皮神经前支各分支至各标志的距离见表1。

图1 股外侧皮神经与切口线的关系(虚线:切口线;X 1线:经过大转子顶端的平行线;X 2线:经过小转子基底部的平行线;X 3线:在X 1线与X 2线之间)

表1 1 0个下肢股外侧皮神经前支分支至各标志的距离(c m)
2.2 旋股外侧动脉 旋股外侧动脉分支与切口线的交叉点与ASIS、X1线距离见表2。在X1与X2两线之间,所有尸体下肢标本的旋股外侧动脉分为升支、横支、降支(图2)。升支经常上升至股骨颈中部上方,横支经常在X1、X2两线之间,降支在X2线下方(图3)。近端股外侧肌和股中间肌的血供来源于旋股外侧动脉横支或升支。

表2 1 0个下肢旋股外侧动脉分支与各标志的距离(c m)

图2 大转子平面至小转子平面之间的血管神经分布(a:右髋前区;b:同一右髋正位X线片;X 1线:经过大转子顶端的平行线;X 2线:经过小转子基底部的平行线)
2.3 股神经 股神经分支进入肌腹的入肌点与ASIS、X1线距离见表3,股神经分支的入肌点与切口线的关系见图4。近端支配股外侧肌神经分支X1线的距离为1.1~7.4(4.70±2.09)cm。
旋股外侧动脉分支与股神经的肌肉分支进入股外侧肌与股中间肌的肌纤维中形成一张神经血管网。笔者发现股外侧肌肌腹分成近内侧部与远外侧部。这2个肌腹与股中间肌的外侧部都受同一股神经外侧分支支配。股外侧肌外侧部的主要神经分支与旋股外侧动静脉伴行(图5)。另外的神经分支是来自股神经的近端分支。

图3 切口线与旋股外侧动脉的关系

表3 1 0个下肢股神经股外侧肌支入肌点至各标志的距离(c m)

图4 股神经与切口线的关系
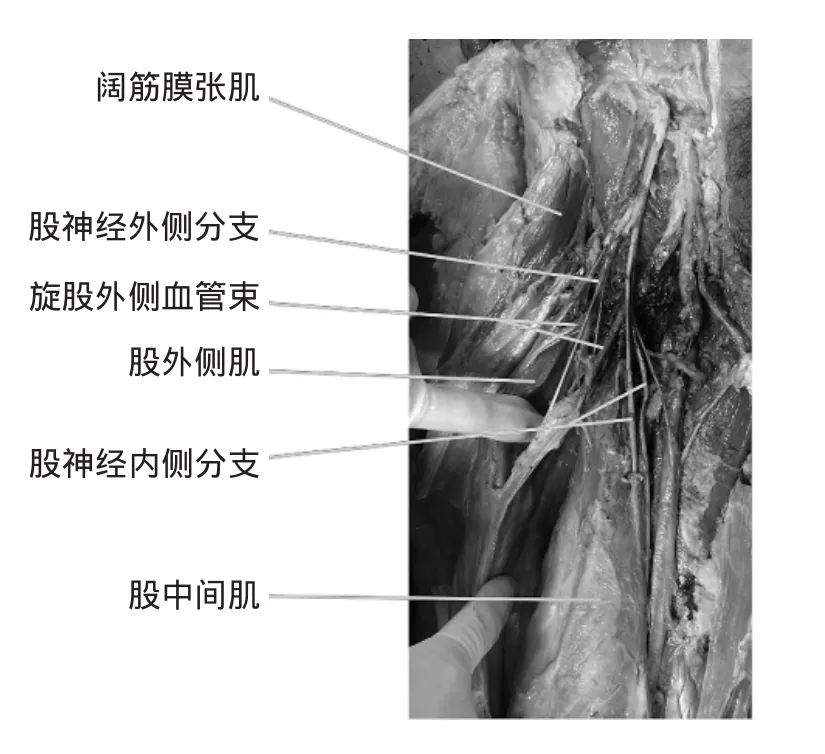
图5 图中可见股神经外侧分支分别进入股外侧肌与股中间肌外侧部,股神经分支与旋股外侧血管束伴行。股神经内侧分支进入股中间肌内侧部
股中间肌外侧部与股外侧肌接受相同的神经分支(即股神经外侧分支)支配。股中间肌内侧部接受股神经内侧分支支配。这些神经分支支配股中间肌的深层,这块肌肉的远端是膝关节肌。股神经分支呈拱形样支配股直肌和缝匠肌,这些分支更加表浅,距离股骨前方更远。股外侧肌和股中间肌的肌肉部分往往在股骨粗线的背侧汇合。在肌肉深面,神经分支分散开来,有些延伸进入附近的肌肉。更远一点的,末梢分支向外侧延伸进入股中间肌,并且进入股外侧肌背侧支配它。神经分支在肌肉内的走形存在一种特殊的形式,主要神经分支在远端以一种螺旋围绕着股骨干的形式在股中间肌肉层间延伸,并且它们最后在背侧分为终末分支。
3 讨论
髋关节直接前入路是真正的神经平面间入路,并且已经被多位学者成功使用。然而,有报道说该入路会增加一些并发症的风险,如术中转子骨折、股骨骨折、股骨穿孔。发生这些并发症后则需要行入路的远端延长,髋关节翻修手术同样也需要入路的远端延长[15-17]。笔者描述过直接前入路的远端延长,它通过切开股直肌和股外侧肌之间的肌肉间隙,进一步暴露股骨端。目前研究显示[18],施行该入路的远端延长,切口两侧的神经血管束会受到直接损伤,进而影响股外侧肌和股中间肌外侧部的功能。并且,当外科医生操作至股骨的时候,肌肉深部的神经血管束会因术中肌肉的移动受到间接牵拉而损伤。
Patil等[19]研究了股外侧肌的神经支配模式,并且他们的发现与之前的研究结果一致。沿着股骨中外侧线切开股外侧肌会使肌肉的后一半失神经支配。在大部分情况下,在同一平面切开股中间肌会导致整块股中间肌失神经支配。股外侧肌是股四头肌当中最大的一块肌肉,所以从理论上来说,股外侧肌和股中间肌损伤会直接导致股四头肌力量的减少。然而,Kennon等[20]报道,在使用直接前入路行翻修手术时,包括股骨干的翻修甚至整个股骨假体的置换,该入路可以向近端和远端延长。这可能与支配股中间肌的神经分支也支配股外侧肌的远侧部分,并且向股骨远端延伸不会影响股外侧肌远侧部分神经支配有关。但在某些患者股外侧肌和股中间肌外侧部部分功能的损伤可以被其他部分股四头肌代偿。
目前的研究结果强调股骨转子间线以远的区域是非常重要的[21]。该切口首先碰到的就是股外侧皮神经。股外侧皮神经外侧支在大转子平面上位于切口内侧,一般不会损伤,在小转子平面,股外侧皮神经外侧支则已跨过切口至切口外侧。所以髋关节前入路若欲延长切口,首先要避开该神经,游离股外侧皮神经至内侧,否则容易损伤该神经,导致股前区感觉障碍。旋股外侧动脉是股深动脉或股动脉的主要分支,该研究的尸体标本旋股外侧动脉均在股三角处发自股深动脉。旋股外侧动脉升支在股直肌的后面斜向外上行于阔筋膜张肌和臀小肌前部纤维的深面,分出阔筋膜张肌支、臀中肌支、缝匠肌支、髂腰肌支、股直肌支、股外侧肌支,并营养以上肌肉和大转子。旋股外侧动脉横支发出到股骨颈前部的分支(前颈升动脉)供应转子间线和股骨颈前部。由此可得知,旋股外侧动脉分支大量地参与股四头肌近端的血管形成[22-25]。该研究显示旋股外侧动脉升支与X1线的距离非常接近,直接前入路切口延长若超出大转子平面,则非常有可能损伤该分支,造成出血,并且影响髋关节的血供。因此,前路手术仔细观察股外侧动脉升支与间隙的关系,如血管横越过间隙或血管走行平面过高,需进行结扎;如血管靠近间隙外侧缘,特别是对于经前路髋关节松解术或减压术操作的情况,可暂时不予结扎。保留股外侧动脉升支有利于髋关节手术的恢复,同时可为股前外侧皮瓣游离移植保留良好的皮瓣。该研究中,股神经股外侧肌神经分支的入肌点距离X1线最短仅有1.1cm,当前入路切口超过大转子平面1.1cm,则很有可能损伤股神经股外侧肌分支,从而导致部分股外侧肌失神经支配,影响髋关节的功能。当然这种程度的失神经支配能否经过其他部分的股四头肌代偿则有待进一步的研究明确。
综上所述,本研究结果说明髋关节直接前入路的远端延长非常困难,因为它可能损害支配股四头肌前外侧部的神经血管束。髋关节直接前入路最适合在股骨转子间线近端的操作,如初次的髋关节置换,股骨头骨折处理,髋臼翻修,还有简单的股骨干翻修。在复杂的迫切需行远端延长切口的股骨干翻修术中,它需要髋关节其他入路或者扩大术的股骨转子截骨术。
[1]Hallert O,Li Y,Brismar H,et al.The direct anterior approach:initial experience of a minimally invasive technique for total hip arthroplasty[J].J Orthop Surg Res,2012,7:17.doi:10.1186/1749-799X-7-17.
[2]Zawadsky M W,Paulus M C,Murray P J,et al.Early outcome comparison between the direct anterior approach and the mini-incision posterior approach for primary total hip arthroplasty: 150 consecutive cases[J].J Arthroplasty,2014,29(6):1256-1260. doi:10.1016/j.arth.2013.11.013.
[3]Rathod P A,Orishimo K F,Kremenic I J,et al.Similar improvement in gait parameters following direct anterior&posterior approach total hip arthroplasty[J].J Arthroplasty,2014,29(6): 1261-1264.doi:10.1016/j.arth.2013.11.021.
[4]Barrett W P,Turner S E,Leopold J P.Prospective randomized study of direct anterior vs postero-lateral approach for total hip arthroplasty[J].J Arthroplasty,2013,28(9):1634-1638.doi:10. 1016/j.arth.2013.01.034.
[5]Parvizi J,Restrepo C,Maltenfort M G.Total hip arthroplasty performed through direct anterior approach provides superior early outcome:results of a randomized,prospective study[J].Orthop Clin North Am,2016,47(3):497-504.doi:10.1016/j.ocl.2016.03.003.
[6]Thürig G,Schmitt J W,Slankamenac K,et al.Safety of total hip arthroplasty for femoral neck fractures using the direct anterior approach:a retrospective observational study in 86 elderly patients[J].Patient Saf Surg,2016,10:12.doi:10.1186/s13037-016-0100-2.
[7]Tsukada S,Wakui M.Lower dislocation rate following total hip arthroplasty via direct anterior approach than via posterior approach:five-year-average follow-up results[J].Open Orthop J, 2015,9:157-162.doi:10.2174/1874325001509010157.
[8]Lanting B A,Odum S M,Cope R P,et al.Incidence of perioperative events in single setting bilateral direct anterior approach total hip arthroplasty[J].J Arthroplasty,2015,30(3):465-467.doi:10. 1016/j.arth.2014.09.021.
[9]Christensen C P,Karthikeyan T,Jacobs C A.Greater prevalence of wound complications requiring reoperation with direct anterior approach total hip arthroplasty[J].J Arthroplasty,2014,29(9): 1839-1841.doi:10.1016/j.arth.2014.04.036.
[10]Hartford J M,Knowles S B.Risk factors for perioperative femoral fractures:cementless femoral implants and the direct anterior approach using a fracture table[J].J Arthroplasty,2016,31(9): 2013-2018.doi:10.1016/j.arth.2016.02.045.
[11]PurcellR L,Parks N L,Gargiulo J,et al.Severely obese patients have a higher risk of infection after direct anterior approach total hip arthroplasty[J].J Arthroplasty,2016,31(9 Suppl):162-165. doi:10.1016/j.arth.2016.03.037.
[12]Jahng KH,Bas MA,Rodriguez J A,et al.Risk factors for wound complications after direct anterior approach hip arthroplasty[J]. J Arthroplasty,2016,31(11):2583-2587.doi:10.1016/j.arth.2016. 04.030.
[13]Homma Y,Baba T,Ochi H,et al.Greater trochanter chip fractures in the direct anterior approach for total hip arthroplasty[J]. Eur J Orthop Surg Traumatol,2016,26(6):605-611.doi:10.1007/ s00590-016-1798-3.
[14]Tamaki T,Oinuma K,Miura Y,et al.Perioperative complication rate of one-stage bilateral total hip arthroplasty using the direct anterior approach[J].J Orthop Sci,2016,21(5):658-661.doi:10. 1016/j.jos.2016.06.002.
[15]Manrique J,Chen A F,Heller S,et al.Direct anterior approach for revision total hip arthroplasty[J].Ann Transl Med,2014,2 (10):100.doi:10.3978/j.issn.2305-5839.2014.09.11.
[16]Nogler M,Mayr E,Krismer M.[The direct anterior approach to the hip revision][J].Oper Orthop Traumatol,2012,24(2): 153-164.doi:10.1007/s00064-011-0113-z.
[17]Cogan A,Klouche S,Mamoudy P,et al.Total hip arthroplasty dislocation rate following isolated cup revision using Hueter's direct anterior approach on a fracture table[J].Orthop TraumatolSurg Res,2011,97(5):501-505.doi:10.1016/j.otsr.2011.04. 005.
[18]叶斌,苗华,于光生,等.髋关节前外侧入路的应用解剖及临床意义[J].解剖与临床,2004,9(1):19-20.doi:10.3969/j.issn.1671-1673. 2004.01.006.
[19]PatilS,Grigoris P,Shaw-Dunn J,et al.Innervation of vastus lateralis muscle[J].Clin Anat,2007,20(5):556-559.doi:10.1002/ca. 20444.
[20]Kennon R E,KeggiM J,KeggiK J.[The minimally invasive anterior approach to hip arthroplasty][J].Orthopade,2006,35(7): 731-737.doi:10.1007/s00132-006-0965-3.
[21]Grob K,Monahan R,Gilbey H,et al.Distal extension of the direct anterior approach to the hip poses risk to neurovascular structures:an anatomical study[J].J Bone Joint Surg Am,2015, 97(2):126-132.doi:10.2106/JBJS.N.00551.
[22]Loskot P,Tonar Z,Baxa J,et al.The descending branch of the lateral circumflex femoral artery as an alternative conduit for coronary artery bypass grafting:Experience from an anatomical,radiologicaland histologicalstudy[J].Clin Anat,2016,29(6): 779-788.doi:10.1002/ca.22737.
[23]Boonrod A,Thammaroj T,Jianmongkol S,et al.Distal anastomosis patterns of the descending branch of the lateral circumflex femoral artery[J].J Plast Surg Hand Surg,2016,50(3):167-170.doi:10.3109/2000656X.2015.1137927.
[24]GoelS,Arora J,Mehta V,et al.Unusualdisposition of lateralcircumflex femoral artery:anatomical description and clinical implications[J].World J Clin Cases,2015,3(1):85-88.doi:10. 12998/wjcc.v3.i1.85.
[25]Vuksanovic-Bozaric A,Radojevic N,Muhovic D,et al.Significance of anatomical variations of the lateral circumflex femoral artery for the tensor fasciae latae flapping[J].Folia Morphol (Warsz),2015,74(3):389-395.doi:10.5603/FM.2015.0060.
Applied anatomy of distal extension of direct anterior approach incision in the hip
LI Bin,CAI Ningyu,SHI Xuchao,et al.
Traumatic Orthopedics,the Second Affiliated Hospital of Wenzhou Medical University,Wenzhou 325027,China
Objective To provide an anatomical basis for the distal extension of direct anterior approach and its surrounding vulnerable structures in the hip. Methods Ten adult cadaveric lower extremities were dissected to observe anatomical structures of significant nerves and vascularities according to the operational process. Results The distances from the lateral branch of the lateral femoral cutaneous nerve to the incision on X1,X2,X3 plane were 0.61±0.39,-0.65±0.39, -0.10±0.32cm,respectivley,the distances from the medial branch of the lateral femoral cutaneous nerve to the incision on X1, X2,X3 plane were 1.53±0.52,0.67±0.56,1.28±0.56cm,respectively.The distances from the intersections of the branches of the lateral femoral circumflex artery(ascending,transverse and descending)with the incision to ASIS were 7.77±0.79,11.01± 1.48,14.91±1.48cm,respectively,the distances from the intersections of the branches of the lateral femoral circumflex artery (ascending,transverse and descending)with the incision to X1 plane were 0.48±0.58,4.99±1.18,7.35±1.07cm,respectively. The distances from the entrance points of nerve branches of the vastus lateralis(the proximal one and the distal one)to ASIS were 11.26±0.96,15.09±1.74cm,respectivley,the distances from the entrance points of nerve branches of the vastus lateralis(the proximal one and the distal one)to X1 plane were 4.70±2.09,7.71±1.45cm,respectively. Conclusion The area distal to the intertrochanteric line is a common entry point for several nerve branches.The distal extension of the direct anterior approach should not exceed 1.1cm under the plane of the great trochanter.
Hip jointDirect anterior approach Distal extension Applied anatomy
2 0 1 6-0 9-2 8)
(本文编辑:陈丽)
10.12056/j.issn.1006- 2785.2017.39.8.2016- 1531
浙江省医药卫生平台计划(骨干人才)(2 0 1 4 R C A 0 1 7)
325027温州医科大学附属第二医院创伤骨科
潘骏,E- m ail:panjun@ hotm ail.com