原发性肝癌外科治疗方式选择及术后肿瘤复发防治相关性研究
2017-02-10莫凯迪杨建荣李碧锦何二松许宇彪林昌荣
莫凯迪 杨建荣 李碧锦 何二松 许宇彪 林昌荣
原发性肝癌外科治疗方式选择及术后肿瘤复发防治相关性研究
莫凯迪 杨建荣 李碧锦 何二松 许宇彪 林昌荣
目的 比较原发性肝癌患者肝切除术和肝移植术的长期疗效,探讨肝脏功能良好的早期肝癌患者肝切除术后复发的影响因素。方法 选取原发性肝癌患者77例,其中70例肝切除患者,7例肝移植患者;采用SPSS 20.0统计学软件分析肝切除患者和肝移植患者的生存疗效及肝功能Child-Pugh A级患者的肝切除术后复发的影响因素。结果 肝移植组合并肝硬化患者比率显著高于肝切除组(P=0.015);肝切除组肝功能Child-Pugh分级与肝移植组肝功能Child-Pugh分级的差异具有统计学意义(P=0.008);肝移植组患者术前接受TACE治疗比率显著高于肝切除组(P=0.003)。两组患者在性别、年龄、乙肝感染、肿瘤大小、肿瘤分化程度及术后辅助化疗等方面均无统计学差异(P>0.05);肝移植组患者的术后并发症发生率、术中出血量及术中输血率均显著高于肝切除组(P<0.001);但两组患者在围手术期医院死亡率、二次手术率方面比较无显著差异(P>0.05);肝移植组患者的无瘤生存率明显优于肝切除组(P=0.041);单因素分析结果显示:乙肝病毒感染、重度肝硬化、血小板<100×109/L、甲胎蛋白>100 ng/ml和肿瘤中低分化是影响Child-Pugh A级直径≤5 cm的单个小肝癌切除术后肿瘤复发的重要不良预后因素;多因素分析结果显示,重度肝硬化、血小板<100×109/L和肿瘤中低分化是影响Child-Pugh A级直径≤5cm的单个小肝癌切除术后肿瘤复发的独立危险因素。结论 肝移植术治疗重度肝硬化的单个小肝癌患者的疗效优于肝切除术,肝移植术可作为首选方法,非重度肝硬化可考虑肝切除术;因此,术前应对肝功能Child-Pugh A级的单个小肝癌患者进行肝硬化严重程度分级,依此选择合适的外科治疗方法。
原发性肝癌;肝移植术;肝切除术;肝硬化
(ThePracticalJournalofCancer,2017,32:124~127)
原发性肝癌在我国发病率高达1/2000,是我国恶性肿瘤第二位,且每年新患肝癌占世界新患肝癌人数的一半以上[1]。近年来,随着医学影像学及外科手术技术的发展,肝癌患者经治疗后生存率得到大幅度提高[2]。肝移植是早期肝癌最为有效的治疗方法,但由于正常肝源供应紧缺,治疗早期肝癌,仍然较多的首选肝切除[3]。最近有研究报道,肝功能良好Child-Pugh A级的早期肝癌患者,肝切除与肝移植的治疗效果差异不大,但仍存在较大的争议,而且肝硬化严重程度亦有轻重之分,我们设想肝硬化严重程度的分级是否影响早期肝癌切除术后肿瘤复发和患者的生存率[4]。因此,本研究选取江滨医院在2013年1月至2016年1月期间诊治的原发性肝癌患者77例,比较原发性肝癌患者肝切除术和肝移植术的长期生存疗效,探讨肝功能Child-Pugh A级的单个小肝癌早期患者肝切除术后复发的影响因素。
1 资料与方法
1.1 病例来源
选取江滨医院在2013年1月至2016年1月期间诊治的原发性肝癌患者77例,其中70例肝切除患者,7例肝移植患者。肝切除患者中,男性59例,女性11例;年龄17~80岁,中位年龄51岁;合并乙型肝炎61例;合并肝硬化56例,其中重度4例;肿瘤大小1.1~5.0 cm,中位大小3.6 cm;术前肝功能Child-Pugh分级:64例为A级,6例为B级;肿瘤分化程度:高分化21例,中分化42例,低分化5例;术前接受TACE治疗2例;术后接受辅助治疗21例。肝移植患者中,男性6例,女性1例;年龄27~64岁,中位年龄50岁;合并乙型肝炎6例;合并肝硬化7例,其中重度3例;肿瘤大小0.9~5.0 cm,中位大小3.4 cm;术前肝功能Child-Pugh分级:2例为A级,3例为B级,2例为C级;肿瘤分化程度:高分化4例,中分化3例;术前接受TACE治疗2例;术后接受辅助治疗4例。选择标准[5]:①肝脏肿瘤为单个且直径≤5 cm;②肿瘤未远处转移;③患者无其他手术禁忌;④术中切除肿瘤完整;⑤手术切除标本为原发性肝细胞癌。
1.2 方法
治疗方法[6-8]:两组患者均在全身麻醉下行手术,且在术后常规予保肝、感染控制,并及时处理并发症;肝切除组行常规开腹肝癌根治性切除术,肝移植组行原位背驼式全肝移植术。术后随访:两组患者术后2年内每月1次B超及肝功能检查;每2个月行1次胸部X线片检查。术后2年平均每半年复查1次,一旦确诊肿瘤复发及时住院治疗,1年内复发行TACE治疗;1年后复发再次行手术切除。生存时间以月计算,无瘤生存时间以确诊为肿瘤复发为终点。
1.3 统计学分析
应用SPSS 20.0软件对患者资料进行统计分析。计量资料采用t检验,计数资料采用χ2检验;Kaplan-Meier法计算患者术后无瘤生存率;采用log-rank检验和Cox风险比例模型进行预后单因素和多因素分析;P<0.05表示差异具有统计学意义。
2 结果
2.1 肝切除组和肝移植组患者病理因素比较(表1)
肝移植组合并肝硬化患者中42.86%为重度肝硬化,显著高于肝切除组的8.57%,两者差异具有统计学意义(P=0.015);肝切除组91.43%为肝功能Child-Pugh分级A级,而肝移植组71.43%为肝功能Child-Pugh分级B级或C级,两者差异具有统计学意义(P=0.008);肝移植组中28.57%患者接受术前TACE治疗显著高于肝切除组的2.86%,两者差异具有统计学意义(P=0.003)。两组患者在性别、年龄、乙肝感染、肿瘤大小、肿瘤分化程度及术后辅助化疗等方面均无统计学差异(P>0.05)。
2.2 近期疗效
肝移植组中出现术后并发症4例,其中肺部感染3例,胆道感染1例,均经保守治疗后好转;术中中位出血量为1 400 ml(300~12 000 ml),其中6例需术中输血。肝切除组(70例)出现术后并发症6例,其中肺部感染4例,腹腔内出血1例,大量腹腔积液1例,均经保守治疗后好转;术中中位出血量为300 ml(100~1 500 ml),其中7例需术中输血。肝移植组患者的术后并发症发生率、术中出血量及术中输血率均显著高于肝切除组(P<0.001)。但两组围手术期医院死亡率、二次手术率比较无显著差异(P>0.05),见表2。

表1 两组患者的病理因素比较(例,%)
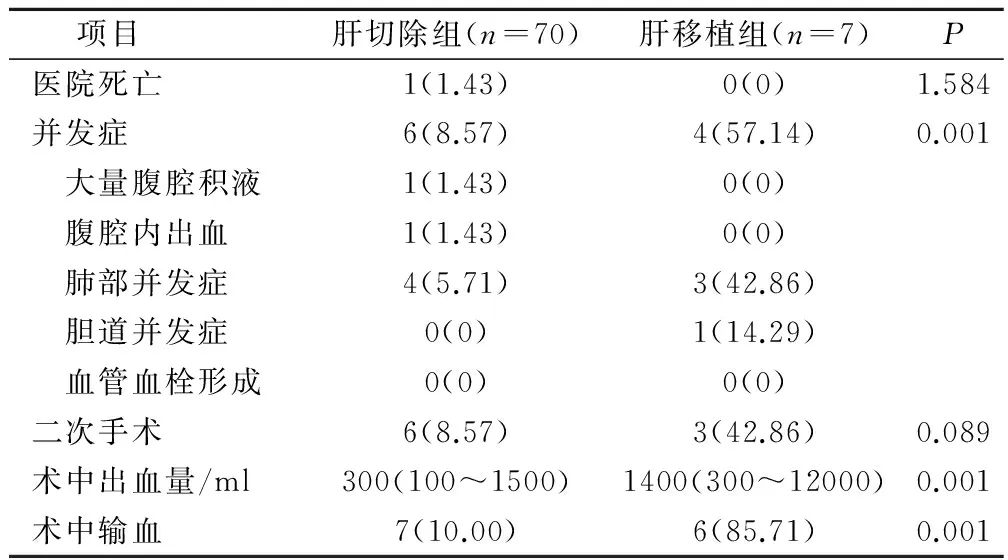
表2 两组患者的围手术期资料(例,%)
2.3 远期疗效
截止2016年4月,肝移植组中1例患者出现肿瘤复发并死亡;肝切除组29例患者出现肿瘤复发,24例已经死亡,其中21例死于肿瘤复发,3例死于上消化道大出血。肝切除组1年、2年和3年无瘤生存率分别为85.71%,74.29%和65.71%;肝移植组患者1年、2年和3年无瘤生存率分别为100.0%,85.71%和85.71%。肝移植组患者的无瘤生存率明显优于肝切除组(P=0.041)。
2.4 肝功能Child-Pugh A级肝切除组患者预后分析
为了鉴别肝功能Child-Pugh A级肝切除组患者术后肿瘤复发的不良预后因素,对该组64例患者的年龄、性别、乙肝病毒感染、重度肝硬化、血小板计数、血浆甲胎蛋白、肿瘤大小、肿瘤分化程度、肝切除类型、术中输血、术前TACE、术后预防性化疗等因素进行分析。单因素分析结果显示:乙肝病毒感染、重度肝硬化、血小板<100×109/L、甲胎蛋白>100 ng/ml和肿瘤中低分化是影响Child-Pugh A级单个小肝癌切除术后肿瘤复发的重要不良预后因素。多因素分析结果显示,重度肝硬化、血小板<100×109/L和肿瘤中低分化是影响Child-Pugh A级单个小肝癌切除术后肿瘤复发的最重要的不良预后因素,见表3、表4。

表3 肝切除组患者术后肿瘤复发的单因素分析(例,%)
3 讨论
肝移植术具有去除肿瘤及潜在病变的肝脏,因此被认为是早期肝癌患者的最佳治疗方法[9]。最近有研究报道,肝功能良好Child-Pugh A级的早期肝癌患者,肝切除术与肝移植术的治疗效果差异不大[10]。若肝功能Child-Pugh A级的早期患者伴有肝硬化,肝切除术的治疗效果并非全部良好[11]。Taura研究报道293例早期肝癌行肝切除术患者,伴有肝硬化166例;结果显示,伴有肝硬化患者具有更高的围手术期死亡率和肿瘤复发率[12]。本研究结果显示,重度肝硬化是影响Child-Pugh A级单个小肝癌切除术后肿瘤复发的重要不良预后因素。因此,我们建议,肝切除术前应对肝功能Child-Pugh A级的早期肝癌患者进行肝硬化严重程度分级[13]。由于正常肝源供应紧缺,治疗Child-Pugh A级早期肝癌,仍然较多的首选肝切除[14]。本研究结果显示,肝移植组患者的无瘤生存率明显优于肝切除组,可能是由于肝切除术后复发性肝癌可能性更高,需再次进行肝切除等治疗,导致无瘤生存率下降。可以预见,随着术后时间的延长,Child-Pugh A级早期肝癌肝移植组患者的长期生存率亦优于肝切除组[15-16]。以往研究表明,Child-Pugh A级早期肝癌患者肝切除术后3年无瘤生存率60%左右,肝移植术后的3年无瘤生存率为80%左右,本研究与之相符[17]。本次研究发现,重度肝硬化是影响Child-Pugh A级单个小肝癌切除术后肿瘤复发的重要不良预后因素。因此,对Child-Pugh A级合并肝硬化的早期肝癌患者,研究其肝硬化严重程度分级对治疗方法选择具有重要临床指导意义[18]。本研究结果表明,对非重度肝硬化的单个小肝癌患者,肝切除术疗效显著,其无瘤生存率接近肝移植术,肝切除术可作为首选治疗方法;而对重度肝硬化的单个小肝癌患者,肝移植应该作为该类病人的首选治疗方法。综上所述,肝移植术治疗重度肝硬化的单个小肝癌患者的疗效优于肝切除术,肝移植术可作为该类病人的首选方法,非重度肝硬化可考虑肝切除术;因此,我们建议,肝切除术前应对肝功能Child-Pugh A级的早期肝癌患者进行肝硬化严重程度分级,依此选择合适的外科治疗方法,从而对术后肿瘤的复发具有一定的抑制作用。
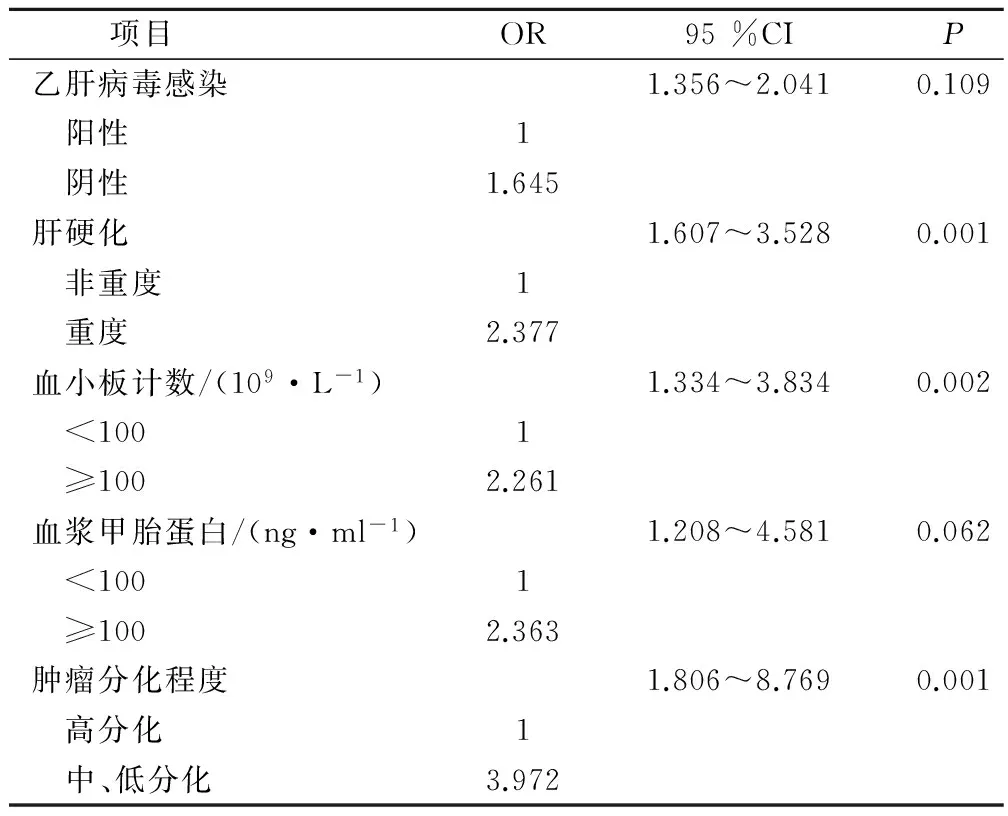
表4 肝切除组患者术后肿瘤复发的多因素分析
[1] Schroeder MC,Lynch CF,Abu-Hejleh T,et al.Chemotherapy Use and Surgical Treatment by Receptor Subtype in Node-Negative T1a and T1b Female Breast Cancers,Iowa SEER Registry,2010-to 2012〔J〕.Clin Breast Cancer,2015,15(1):e27-344.
[2] Alagaratnam S,Kurzawinski TR.Aetiology,Diagnosis and - Surgical Treatment of Primary Hyperparathyroidism in Children:New Trends〔J〕.Horm Res Paediatr,2015,83(6):365-375.
[3] Nishikawa H,Osaki Y,Komekado H,et al.Clinical significance of the FIB-4 index for non-B non-C hepatocellular carcinoma treated with surgical resection〔J〕.Oncol Rep,2015,33(1):88-94.
[4] Fukubayashi K,Tanaka M,Izumi K,et al.Evaluation of sorafenib treatment and hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma:a comparative study using the propensity score matching method〔J〕.Cancer Med,2015,4(8):1214-1223.
[5] Taylor H.Translationally controlled tumor protein in prostatic adenocarcinoma:correlation with tumor grading and treatment-related changes〔J〕.Biomed Res Int, 2015,2015:985950.
[6] Ng KT,Lo CM,Wong N,et al.Early-phase circulating miRNAs predict tumor recurrence and survival of hepatocellular carcinoma patients after liver transplantation〔J〕.Oncotarget,2016,7(15):19824-19839.
[7] Sestak I,Cuzick J,Dowsett M,et al.Prediction of late distant recurrence after 5 years of endocrine treatment:a combined analysis of patients from the Austrian breast and colorectal cancer study group 8 and arimidex,tamoxifen alone or in combination randomized trials using the PAM50 risk 〔J〕.J Clin Oncol,2015,33(8):916-922.
[8] Hou W,Zhu X.Extra vascular interventional treatment of liver cancer,present and future〔J〕.Drug Discov Ther,2015,9(5):335-341.
[9] Kataoka K,Kanazawa A,Nakajima A,et al.Prognostic value of biomarkers in metastatic colorectal cancer patients〔J〕.J Surg Res,2015,194(2):343-350.
[10] Song J,Liu H,Zhen L,et al.Long-term prognosis of surgical treatment for early ampullary cancers and implications for local ampullectomy〔J〕.Bmc Surgery,2015,15(1):1-7.
[11] Sironi S,Ferrero C,Gianolli L,et al.The Role of Imaging in the Diagnosis and Staging of Primary and Recurrent Rectal Cancer〔M〕.Springer London,2015:81-95.
[12] Fuster J.Surgical treatment of hepatocellular carcinoma:sh- ould resection be performed according to Barcelona Clinic Liver Cancer classification〔J〕.Hepatic Oncology,2015,2(3):1-9.
[13] Varvares MA,Shannon Poti MD,Bianca Kenyon MD,et al.Surgical margins and primary site resection in achieving local control in oral cancer resections〔J〕.Laryngoscope,2015,125(10):2298-2307.
[14] Meng Y,Liao YB,Xu P,et al.Perineural invasion is an independent predictor of biochemical recurrence of prostate cancer after local treatment:a meta-analysis〔J〕.Int J Clin Exp Med,2015,8(8):13267-13274.
[15] Xia W,Ke Q,Wang Y,et al.Predictive value of pre-transplant platelet to lymphocyte ratio for hepatocellular carcinoma recurrence after liver transplantation〔J〕.World J Surg Oncol,2015,13(1):1-7.
[16] Mastoraki A,Toliaki E,Chrisovergi E,et al.Metastatic Liver Disease Associated with Gastrointestinal Stromal Tumors:Controversies in Diagnostic and Therapeutic Approach〔J〕.J Gastrointest Cancer,2015,46(3):237-242.
[17] Zhang X,Liu S,Shen C,et al.DNA methylation consistency implicates the primary tumor cell origin of recurrent hepatocellular carcinoma〔J〕.Epigenomics,2015,7(4):581-592.
[18] Fujiki M,Aucejo F,Choi M,et al.Role of Neoadjuvant and Adjuvant Treatment in HCC Recurrence After Liver Transplantation〔M〕.Springer New York,2016.
(编辑:吴小红)
Surgical Treatment of Primary Liver Cancer and Its Correlation with Tumor Recurrence After Surgical Treatment
MOKaidi,YANGJianrong,LIBijin,etal.
GuangxiJiangbinHospital,Nanning,530021
Objective To compare the long-term therapeutic effect of liver resection and liver transplantation in patients with primary liver cancer,and to explore the influencing factors of recurrence after hepatectomy in patients with hepatocellular carcinoma.Methods 77 cases of primary liver cancer patients,of which 70 cases of hepatic resection patients,7 cases of liver transplantation patients.The statistical software SPSS 20.0 comparative analysis of hepatic resection patients and patients with liver transplantation survival efficacy and child Pugh class A patients with liver resection and the factors influencing postoperative recurrence.Results Liver combined transplantation and in patients with liver cirrhosis ratio was higher than that in liver resection group(P=0.015);liver resection group child Pugh grading and hepatic transplanted liver function of child Pugh grading difference was statistically significant(P=0.008);liver transplantation patients received TACE ratio was higher than that in liver resection group(P=0.003).Two groups of patients were no significant difference in gender,age,hepatitis B infection,tumor size,tumor differentiation and postoperative adjuvant chemotherapy and other aspects(P>0.05);liver transplantation group patients the incidence of postoperative complications,intraoperative bleeding and blood transfusion rate were significantly higher than those in liver resection group(P<0.001);but 2 patients in the perioperative nosocomial mortality, surgery rate showed no significant difference(P>0.05);liver transplantation in patients with tumor free survival rate was significantly better than the liver resection group(P=0.041);the results of univariate analysis showed that hepatitis B virus infection and severe liver cirrhosis,platelet <100×109/L,>100 ng/ml and tumor AFP low differentiation is an important prognostic factors for tumor recurrence of small hepatocellular carcinoma resection of single Child-Pugh a diameter less than 5cm;the results of multivariate analysis showed that severe liver cirrhosis,blood Effect of child Pugh a less than 5 cm in diameter of a single small hepatocellular carcinoma resection of the independent risk factors of postoperative tumor recurrence is low in <100×109/L and tumor differentiation.ConclusionLiver transplantation in the treatment of severe cirrhosis of single small hepatocellular carcinoma patients with curative effect is better than that of liver resection,liver transplantation can be used as the preferred method,non severe cirrhosis may be considered for liver resection;therefore,preoperative deal with child Pugh class a single small hepatocellular carcinoma in patients with liver cirrhosis severity grading,and choose appropriate surgical treatment.
Primary liver cancer;Liver transplantation;Liver resection;Liver cirrhosis
530021 广西壮族自治区江滨医院
10.3969/j.issn.1001-5930.2017.01.039
R735.7
A
1001-5930(2017)01-0124-04
2016-07-06
2016-09-06)
