改良完壁式鼓室成形术治疗上鼓室局限性阻塞性病变
2016-12-22马玉坤蒋立新廖志芳涂博肖志文
马玉坤 蒋立新 廖志芳 涂博 肖志文
暨南大学附属第一医院耳鼻咽喉头颈外科
·咽鼓管专辑·
改良完壁式鼓室成形术治疗上鼓室局限性阻塞性病变
马玉坤 蒋立新 廖志芳 涂博 肖志文
暨南大学附属第一医院耳鼻咽喉头颈外科
目的 探讨上鼓室局限性阻塞性病变的手术方法与疗效。方法75例(88耳)上鼓室局限性阻塞性病变,其中胆脂瘤及内陷袋46耳,肉芽肿42耳。经上鼓室外侧壁进路,在颞线下自后上嵴至颧弓后根磨开骨壁,保留菲薄的外耳道后上骨壁和完好天盖,于后拱柱开放面神经隐窝,清除病变组织,修复或重建听骨链,疏通中、上鼓室气流通道,保留鼓窦乳突,完成改良完壁式鼓室成形术。结果术后鼓膜和外耳道完整。局限性上鼓室胆脂瘤及内陷袋患者平均语頻听力较术前提高15-25dBHL;慢性中耳炎上鼓室肉芽患者平均语频听力较术前提高15-30dBHL。随访5.0年未见胆脂瘤复发。结论改良完壁式鼓室成形术,进路便捷,再通气道,疗效满意。
中耳炎;上鼓室局限性病变;改良完壁式;鼓室成形术
Scientific research training and innovation fund of Jinan University Item number:21612310
Declaration of interest:The authors report no conflicts of interest.
上鼓室经鼓峡与中鼓室相通,砧骨长脚位于鼓峡中央将其分为鼓前峡和鼓后峡,而锤砧关节是上鼓室前后间隙与内外间隙的分隔屏障。此外,上鼓室区有纵横交错的粘膜皱襞,使该区域与声音传导和气流通道密切相关。在咽鼓管通常情况下,各种原因引起鼓峡部分或完全堵塞,对气体流通及听骨链的活动都有不同程度的影响,形成上鼓室局限性病变如内陷袋、胆脂瘤或胆固醇肉芽肿等,有学者称谓局限性上鼓室阻塞综合症(selective epitympanic dysventilation syndrome)[1,10]。由于病灶局限于上鼓室区,很少累及鼓窦及乳突,因此,选择完壁式上鼓室进路手术有一定的临床意义。以上鼓室局限性胆脂瘤为例,目前多行上鼓室开放手术[1,2],如软组织或软骨重建外耳道后上壁,或上鼓室术腔填塞[3-5],但术后多因影响气流通道而疗效不满意[6,12]。本文参照上鼓室进路相关手术方法[7-9],试行改良完壁式鼓室成形术治疗上鼓室局限性阻塞性病变,报道如下。
1 资料与方法
1.1 一般资料
收集我科2006年1月~2009年1月期间具有完整临床资料的75例(88耳)上鼓室局限性病变患者,其中上鼓室胆脂瘤患者40例(46耳),耳内镜检查:鼓膜松弛部内陷袋16耳,松弛部穿孔30耳,颞骨CT检查:病变局限在上鼓室区、天盖无明显破坏或下垂(如图①),虚拟CT耳镜示:听骨链连续19耳(如图②),变形12耳,骨质破坏15耳,纯音听阈测试:患耳平均气导下降<15dBHL 8耳,15-30dBHL 14耳,30-45dBHL 18耳,>45dBHL 6耳;慢性中耳炎上鼓室肉芽肿35例(42耳),耳内镜检查:鼓膜紧张部穿孔36,其中边缘性穿孔12,松弛部穿孔6耳,颞骨CT检查:病变局限在上鼓室区(如图④),虚拟CT耳镜示:听骨链连续18耳,变形16耳,骨质破坏8耳(如图⑤),纯音听阈测试:患耳平均气导下降<15dB HL 4耳、15-30dBHL 10耳、30-45dBHL 15耳,>45dBHL 13耳。以上病例骨导听力均在正常范围内。
1.2 手术方法
耳后切口,切开外耳道后壁皮肤,探查并处理鼓膜松弛部内陷、结痂及穿孔边缘。对内陷袋形成及松弛部穿孔者,于鼓环上6-8 mm从11点到3点处切开外耳道皮肤,掀起鼓-耳道皮瓣达锤骨柄上方,剥离锤骨前突及前韧带鳞状上皮和病变组织。再于颞线下自外耳道后上嵴至颧弓后根磨开上鼓室外侧壁,保留菲薄外耳道后上骨壁和完整鼓室天盖,前方达上鼓室前隐窝,向后达鼓窦入口。视病变情况可磨开后拱柱开放面神经隐窝上方以暴露后鼓室。如中、上鼓室分隔不通,砧骨表面有鳞状上皮或胆脂瘤侵蚀,则摘下砧骨;如锤骨头及砧骨无破坏,则去除锤砧皱襞,剥下粘连带,同时拨开鼓索-鼓膜张肌皱襞,扩大锤骨短突与匙突之间、砧骨长脚与锥隆起之间气流通道。(如图③);如胆脂瘤或肉芽组织破坏锤骨头和砧骨,镫骨正常,则剪除锤骨头,保留鼓膜张肌腱的连接,用改型砧骨镶嵌在镫骨头上(如图⑥)。
1.3 术后随访
术后1年内定期复查鼓膜,检测纯音听阈。随访5.0年,比较手术前、后语频(0.5、1.0、2.0 kHz)气导平均听力,记录听力结果及术后疗效。
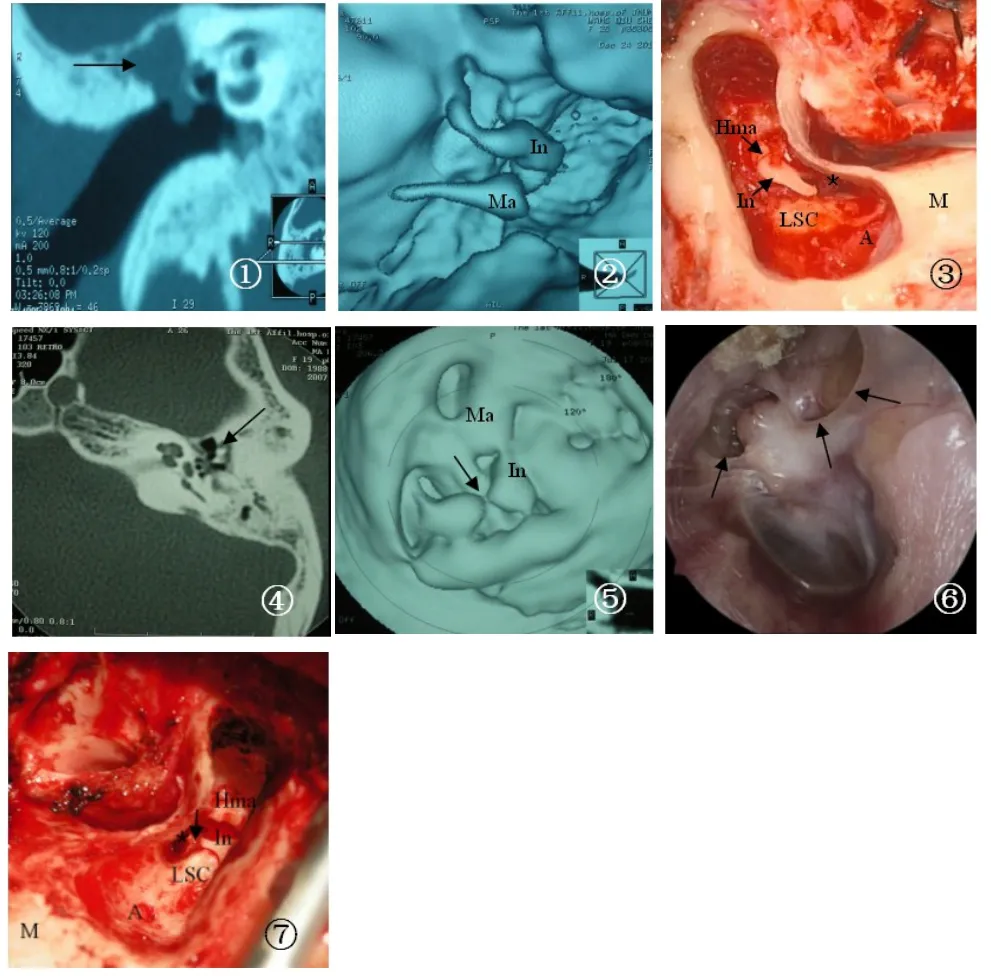
图:①颞骨CT示:右耳上鼓室局限性软组织影(箭头所示),术后病理为胆脂瘤组织;②虚拟耳镜显示:听骨链连续;③术中见上鼓室有完整包囊的胆脂瘤团,期内下方为肉芽组织,中上鼓室通路封闭;LSC:Lateral semicircular canal外半规管,M: mastoid乳突,A:aditus鼓窦入口,Ma:malleus锤骨,Hma: head of malleus锤骨头,In:incus砧骨,*Hst:head of stapes镫骨头.图:④颞骨CT示:左耳上鼓室及听骨链周围可见软组织影(箭头所示),术后病理为肉芽组织;⑤虚拟耳镜显示:听骨链不连续,砧镫关节中断(箭头所示);⑥鼓膜松弛部穿孔,内陷,鼓膜颜色灰黄;⑦术中见锤骨头与砧骨体被肉芽组织包裹,中上鼓室通路阻塞,砧骨长脚远端破坏(箭头所示)。Fig.1 -7①Temporal bone CTshowed localized soft tissue shadow in right ear tympanic(arrow),postoperative pathology was cholesteatoma.②Virtual endoscopy showed intact auditory ossicle chain;③Intraoperative findings:there was a cholesteatoma with complete cyst group in attic,inside and below the attic was the granulation tissue and the path in the attic was closed;LSC: Lateral semi circular canal,M:MASTOID,A:aditus,Ma:malleus,Hma:head of malleus,In:incus,Hst:head of stapes.④Temporal bone CT showed soft tissue around the tympanum in the left ear and ossicular chain(arrow),postoperative pathology was granulation tissue;⑤Virtual endoscopy showed ossicular discontinuity,incudostapedial joint disruption(arrow);⑥Pars flaccida perforated,invaginated,and the drum membrane became yellow.⑦Intraoperative findings:the head of malleus and incus body was wrapped by granulation tissue,attic pathway was blocked, the long process of incusdistal was destroyed(arrow).
2 结果
术中发现,16耳鼓膜松弛部内陷袋及瘢痕形成,11耳均有不同程度的鳞状上皮,5耳胆脂瘤均位于锤骨头与砧骨体外上方。去除胆脂瘤及鳞状上皮,剥开锤砧骨间粘连带,14耳听骨链连续,疏通中、上鼓室气流通道;30耳鼓膜松弛部穿孔,其中16耳胆脂瘤位于锤骨头和砧骨体,1耳达鼓窦入口,13耳锤骨头和砧骨体部分侵蚀,其中9耳砧骨长脚破坏;42耳慢性中耳炎上鼓室肉芽患者,27耳肉芽组织部分包裹听骨链,8耳锤骨头和砧骨体部分侵蚀,锤砧关节破坏,其中7耳砧骨长脚破坏。术后随访5.0年,所有病例耳内镜观察鼓膜完整,无内陷袋及胆脂瘤复发。纯音听阈测试,胆脂瘤患者平均听力较术前提高15-25dB HL,上鼓室肉芽患者平均听力较术前提高15-30dB HL。15耳复查颞骨CT及虚拟CT耳镜,未见胆脂瘤复发或肉芽形成,并见听骨链或听骨链成形术后听小骨位置及连接状态良好。
3 讨论
上鼓室区内有锤骨头、砧骨体形成锤砧关节和相应粘膜皱襞,如有病变则易阻塞。近年来有学者提出局限性上鼓室通气障碍的学说[10],认为即使咽鼓管功能正常,如果存在鼓室隔或鼓峡阻塞,也会导致上鼓室区内陷袋或胆脂瘤形成。通常情况下,上鼓室区有两条气流通路,主通路是气流由咽鼓管进入鼓室,经鼓峡达上鼓室,再经鼓窦入口弥散乳突气房;第二条独立的通道是经Prussak间隙进入上鼓室。如果咽鼓管功能障碍或炎症长期作用,内陷袋和胆脂瘤形成则为定论,但即使咽鼓管功能正常,若Prussak间隙或鼓峡受阻,也会导致上鼓室负压而形成内陷袋及胆脂瘤[10,11,13]。上鼓室反复发生局限性炎性病变,如鼓室积液或难治性分泌性中耳炎,早期多表现为功能性改变,如迁延不愈则粘连带形成,堵塞鼓峡,即使经治疗后咽鼓管功能正常,因中、上鼓室气流通路阻塞仍可能形成内陷袋或胆脂瘤局限于上鼓室的胆脂瘤治疗,早期多遵循Bondy式改良乳突根治术的方法,此后出现了多种改良Bondy式手术,也有行伴乳突切除的开放式或完壁式鼓室成形术[1-5]。但这类患者术前医学影像学检查及术中探查发现乳突和中鼓室多属正常,按常规切除乳突不仅牺牲可保存的乳突气房,同时也使中耳-乳突的气流通道破坏,对术后的解剖与功能均有很大的影响。上鼓室外侧壁切除后,术后重建的鼓膜移植物片缺乏支撑或通气不良,形成上鼓室继发性内陷。也有学者在上鼓室切除后用骨粉或骨水泥填充,但由于鼓室容积缩小,新建鼓膜与听小骨容易粘连。骨皮质修补缺损的外耳道后上壁容易松动和异位,软骨修补上鼓室外侧壁容易发生内陷再发胆脂瘤[3,6,7,12]。最近,有学者针对鼓峡阻塞而鼓窦、乳突无病变的上鼓室局限性病变应用耳内镜手术,清理上鼓室区的炎性组织、内陷袋及胆固醇肉芽肿和胆脂瘤。结果发现,阻塞鼓峡的慢性中耳疾病应该去除鼓膜张肌皱襞并恢复鼓峡功能,重建咽鼓管—上鼓室—乳突区气流通路,术后未见内陷袋形成或胆脂瘤复发[10]。
该术式施行要求术者有较熟练的耳显微外科基本功,对于手术解剖标志较好的定位,否则实际操作中,可能导致病变清除不彻底;术者需术前对于患者病变及术者对术式掌握程度,综合考虑。此外术前阅读颞骨CT,如发现硬脑膜严重低垂者,则不适于本术式。
本文试行改良完壁式鼓室成形术,直接开放上鼓室外侧壁,暴露并清除上鼓室区病灶,处理听骨链和气流通路,不做乳突开放,直接于砧骨窝开放面神经隐窝进入后鼓室,处理锥隆起及镫骨旁病变。改良的上鼓室进路为处理上鼓室胆脂瘤及其它局限性病变提供了一个进路便捷而损伤较小的微创方法,有效地防止了术后粘连、内陷袋形成或胆脂瘤复发。经上鼓室进路手术是通向上鼓室包括前上鼓室间隙的最短路径[7],对上鼓室局限性病变,经开放的上鼓室可方便、快捷地完成手术。但对于中耳慢性炎性病变及胆脂瘤,早期多局限在上鼓室未侵犯乳突、鼓窦,主要表现为鼓膜内陷或穿孔,压迫性骨质吸收或骨质破坏。临床经验表明,当病变较局限时,所采取的手术方式越简捷,手术后的效果越明显[9]。本文按照联合径路鼓室成形术的基本原则,直接经上鼓室外侧壁进路,保留完整的外耳道后上壁和天盖骨板,暴露鼓窦入口及后鼓室,不做乳突切除,疏通咽鼓管—鼓室—乳突气体交流通道。经验表明,鼓室成形术的听力效果取决于鼓膜和听骨链的有效重建及良好的中耳换气功能[11-12],本文注重开放气体通道和重建听力传导装置,保障术后中耳气体流通系统和声音有效传导,获得较满意的临床疗效。
1 Sanna M,Agarwal M,Khrais T,et al.Modified Bondy's technique for epitympanic cholesteatoma[J].Laryngoscope,2003,113(12): 2218-2221.
2 Tarabichi M.Endoscopic management of limited attic cholesteatoma [J].Laryngoscope,2004,114(7):1157-1162.
3 迟放鲁,王正敏,吴琍雯.上鼓室封闭和外侧壁重建技术在鼓室成形术中的应用[J].中华医学杂志,2002,82(23):1617-1618.CHI FL,WANG ZM,WU LW.Application of lateral attic wall recon⁃struction and sealing of attic cell in tympanoplasty[J].National Med⁃ical Journal of China,2002,82(23):1617-1618.
4 Uzun C,Yagiz R,Tas A,et al.Combined Heermann and Tos(CHAT) technique in cholesteatoma surgery:surgical technique and prelimi⁃nary results.J Laryngol,2005,119(6):429-435.
5 Lee WS,Choi JY,Song MH,et al.Mastoid and epitympanic oblitera⁃tion in canal wall up mastoidectomy for prevention of retraction pocket[J].Otol Neurotol,2005,26(6):1107-1111.
6 Pfleiderer AG,Ghosh S,Kairinos N,et al.A study of recurrence of retraction pockets after various methods of primary reconstruction of attic and mesotympanic defects in combined approach tympano⁃plasty[J].Clin Otolaryngol,2003,28(6):548-551.
7 Duckert LG,Makielski KH,Helms J.Management of anterior epitym⁃panic cholesteatoma:expectations after epitympanic approach and canal wall reconstruction[J].Otol Neurotol,2002,23(1):8-13.
8 蒋立新,马玉坤,罗冬,等.完壁式上鼓室进路鼓室探查术治疗外伤性听骨链中断.临床耳鼻咽喉头颈外科杂志,2008,22(13): 580-582. Jiang LX,Ma YK,Luo D,et al.Treating traumatic ossicular chain⁃idisruption with epitympanum approach following tympanotomy[J]. Journal of Clinical Otorhinolaryngology Head and Neck Surgery, 2008,22(13):580-582.
9 蒋立新,马玉坤,罗冬,等.虚拟耳镜对外伤性听骨链中断手术前后的评估作用.中华耳鼻咽喉头颈外科杂志,2008,43(12): 272-276. Jiang LX,Ma YK,Luo D,et al.Evaluation of the Virtual CT Endos⁃copy in Ossicular Chain Disruption Caused by Temporal Bone Frac⁃ture and Ear Trauma[J].Chinese Journal of Otorhinolaryngology Head and Neck Surgery,2008,43(12):272-276.
10 Marchioni D,Mattioli F,Alicandri-Ciufelli M,et al.Endoscopic evaluation of middle ear ventilation route blockage[J].Am J Otolar⁃yngol,2010,31(6):453-66.
11 Marchioni D,Grammatica A,Alicandri-Ciufelli M,et al.The contri⁃bution of selective dysventilation to attical middle ear pathology[J]. Med Hypotheses,2011,77(1):116-20.
12 A.Mahadevaiah,Bhavin Parikh.Modified intact canal wall mastoid⁃ectomy—long term results in hearing and healing[J].Indian J Oto⁃laryngol.Head Neck Surg,2008,60(4):317-323.
13 王凯,俞杰,李幼珍,等,完壁式鼓室成形术治疗慢性化脓性中耳炎[J].中华耳科学杂志,2013,11(4):561-564. Wang K,Yu J,Li YZ,et al.Intact Canal Wall Tympanoplasty in Treating Patients with Chronic Suppurative Otitis Media[J].Chinese Journal of Otology,2013,11(4):561-564.
Modified intact canal wall tympanoplasty for localized attic lesions
MA Yukun,JIANG Lixin,LIAO Zhifang,TU Bo,XIAO Zhiwen
Department of Otorhinolaryngology,the First Affiliated Hospital,Jinan University
Objective To investigate the efficacy of modified intact canal wall tympanoplasty in treating localized attic lesions.Methods Data from 75 patients(88 ears)who underwent surgery for localized attic lesions were retrospectively reviewed.Among all the 88 ears,lesions included localized attic cholesteatoma and retraction pocket(n=46),chronic otitis media with epitympanic granulation(n=35),and adhesive otitis media(n=7).The operation was performed under the temporal line,with bone tissue removed between the suprameatal spine and the dorsal root of zygomatic arch and the tegmen and a meager intact posterior canal wall retained.Next,the attic and posterior tympanum were opened,and the lesion exposed and managed.Ossiculoplasty was performed if the ossicular chain was destroyed.Results Compared with before surgery,hearing improved by about 15-25 dB in patients with localized attic cholesteatoma or(and)retraction pocket,by about 15-30 dB in patients with epitympanic granulation and by about 15-20 dB in patients with adhesive otitis media.There was no recurrent cholesteatoma and the external auditory canal wall and tympanic membrane integrity remained during the 5 years of follow-up.Conclusion The goal of modified intact canal wall tympanoplasty in this situation is preservation of normal structures and restoration of ventilation to the attic space while eliminating lesions.Clinical effects of this modified technique are satisfactory.
Otitis media;Localized attic lesions;Modified intact canal wall;Tympanoplasty
R764.29
A
1672-2922(2016)05-601-4
2016-07-26)
10.3969/j.issn.1672-2922.2016.05.009
暨南大学科研培养与创新基金项目编号:21612310
马玉坤,博士,职称:主治医师,研究方向:耳与侧颅底外科学
蒋立新,Email:jiangdoc@163.com
