右美托咪定对开腹手术中老年患者脑氧饱和度及术后认知功能的影响
2016-12-01侯大亮吴秀英
侯大亮,吴秀英
(中国医科大学附属盛京医院麻醉科,沈阳 110004)
右美托咪定对开腹手术中老年患者脑氧饱和度及术后认知功能的影响
侯大亮,吴秀英
(中国医科大学附属盛京医院麻醉科,沈阳 110004)
目的探索右美托咪定是否能通过提高术中脑氧饱和度而改善择期行全麻下开腹手术的中老年患者术后认知功能。方法选择行全麻下开腹手术的中老年患者40例,随机分为2组:D组(n=20),术前静注右美托咪定(0.5 μg/kg),浓度4 μg/ mL,10 min静脉泵入;N组(n=20),术前静注等量的生理盐水。监测2组患者的心率、平均动脉压及脑氧饱和度。术前与术后进行简易智力状态检查(MMSE)。结果入室时2组患者心率无明显差异(P>0.05),在给药后各时间点,D组心率显著低于N组,差异有统计学意义(P<0.05)。2组患者在各时间点的血压及脑氧饱和度无明显差异(P>0.05)。D组患者术后第1天的MMSE评分高于N组,差异有统计学意义(P<0.05)。结论术前给予右美托咪定可以改善择期行全麻下开腹手术的中老年患者术后认知功能,但不能影响患者的脑氧饱和度。右美托咪定改善术后认知功能的作用不是通过提高术中脑氧饱和度实现的。
右美托咪定;中老年患者;开腹手术;脑氧饱和度;术后认知功能
网络出版地址
脑氧饱和度监测是目前公认的即时反映脑氧代谢情况的监测手段[1],是一种无创测定局部脑组织血液氧饱和度的监测方法,不受温度和搏动血流影响,灵敏性和特异性高,能够体现脑区的氧供需平衡状况[2]。
术后认知功能障碍(postoperative cognitive dys⁃function,POCD)是老年患者常见的术后并发症,在接受腹部手术的患者中发生率较高,可达38%[3]。POCD的发生可能与术中脑氧代谢有关[4]。多项研究[5⁃7]表明,POCD与术中脑氧饱和度降低密切相关。
右美托咪定是一种高选择性的α2肾上腺素受体激动剂,药理作用包括交感神经抑制、镇静、镇痛、抗焦虑等[8]。有研究[9⁃10]认为,术中使用右美托咪定可以改善患者术后认知功能,然而其机制有待进一步研究。
本研究旨在探索右美托咪定是否能通过提高术中脑氧饱和度而改善择期行全麻下开腹手术的中老年患者术后认知功能。
1 材料与方法
1.1病例选择
选择年龄>55岁,择期行全麻下开腹手术的中老年患者。手术种类包括胰十二指肠切除术、直肠癌根治术、结肠癌根治术、胃癌根治术、半肝切除术等。手术时间为1.5~6 h。对患者进行术前评估,并严格按照以下标准进行排除:术前简易智力状态检查(mini⁃mental state examination,MMSE)评分<23分,肝肾功能不全,中枢神经系统病史,心理疾病史,目前服用镇静药物、抗抑郁药物等精神药物,有吸毒、药物依赖史或酗酒史,视力、听力障碍或其他原因导致的交流困难,严重的呼吸系统疾病,严重内环境失调、休克等严重合并症,对本研究中使用的药物过敏,有使用右美托咪定的禁忌证。
共入选患者40例。其中男20例,女20例,年龄(66.7±11.7)岁。ASA分级Ⅱ~Ⅲ级。将患者随机平均分为2组:D组和N组。D组20例患者,术前静注右美托咪定;N组20例患者,术前静注等量的生理盐水。其中D组男11例,女9例,年龄(68.9±12.3)岁,N组男9例,女11例,年龄(64.5±10.9)岁。2组患者的一般情况具有可比性。
1.2麻醉方法
患者入室后,进行心电监护、脉搏血氧饱和度监测和无创血压监测。使用CASMED公司生产的FORE⁃SIGHT脑氧饱和度监护仪进行脑氧饱和度的连续监测。用酒精棉球清洁患者前额皮肤后,将脑氧饱和度监测探头置于患者左、右前额部,发光点距离眉弓上缘2 cm,监测患者的脑氧饱和度。
D组入室后给予0.5 μg/kg的右美托咪定,浓度4 μg/mL,10 min静脉泵入,N组以相同速度泵入等量的生理盐水。麻醉诱导采用舒芬太尼0.3 μg/kg,依托咪酯0.2 mg/kg,顺阿曲库铵0.2 mg/kg。药物充分起效后进行气管内插管,机械通气,氧气流量2 L/min,潮气量8 mL/kg,呼吸频率12次/分,吸呼比1∶2,维持呼气末二氧化碳分压35~45 mmHg。麻醉维持采用吸入七氟醚并静注顺阿曲库铵。根据手术需要调整七氟醚浓度,顺阿曲库铵根据手术的需要追加。整个麻醉过程中不再使用其他镇静、镇痛药物。记录各项所需数据。
1.3观察指标
采用某一时刻在左、右脑测得的平均值作为患者该时刻的脑氧饱和度。分别记录2组患者入室时(T1)、术前给予右美托咪定或生理盐水后(T2)、诱导并插管后(T3)、手术开始时(T4)、手术开始30 min时(T5)、手术开始60 min时(T6)、手术结束时(T7),患者的心率、平均动脉压及脑氧饱和度。
分别记录2组患者的麻醉时间、手术时间、输液量和出血量。用MMSE评估患者术前和术后第1天的认知功能。
1.4统计学分析
2 结果
2.12组患者一般情况比较
2组患者年龄、体质量、麻醉时间、手术时间、输液量及出血量无统计学差异(P均>0.05)。2组患者的一般情况具有可比性。见表1。
表1 2组患者一般情况比较Tab.1 Comparison of general conditions in both groups
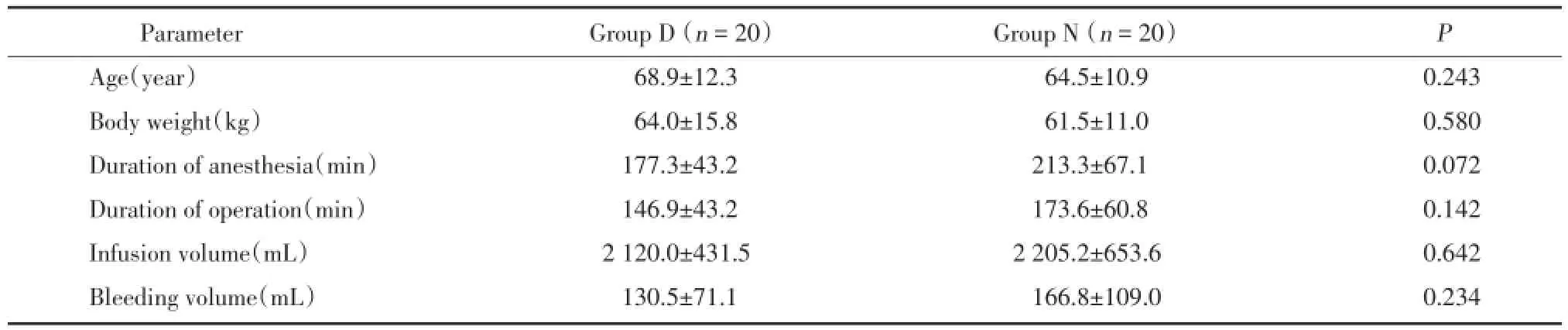
表1 2组患者一般情况比较Tab.1 Comparison of general conditions in both groups
Parameter Group D(n=20) Group N(n=20) P Age(year) 68.9±12.3 64.5±10.9 0.243 Body weight(kg) 64.0±15.8 61.5±11.0 0.580 Duration of anesthesia(min) 177.3±43.2 213.3±67.1 0.072 Duration of operation(min) 146.9±43.2 173.6±60.8 0.142 Infusion volume(mL) 2 120.0±431.5 2 205.2±653.6 0.642 Bleeding volume(mL) 130.5±71.1 166.8±109.0 0.234
2.22组患者各时间点的心率
2组患者在入室时(T1)心率无统计学差异(P>0.05)。给予右美托咪定或生理盐水后的其余各时间点,D组患者的心率均低于N组,差异均有统计学意义(P<0.05)。见表2。
2.32组患者各时间点的平均动脉压
表2 2组患者各时间点心率Tab.2 The heat rates of the two groups at different time points
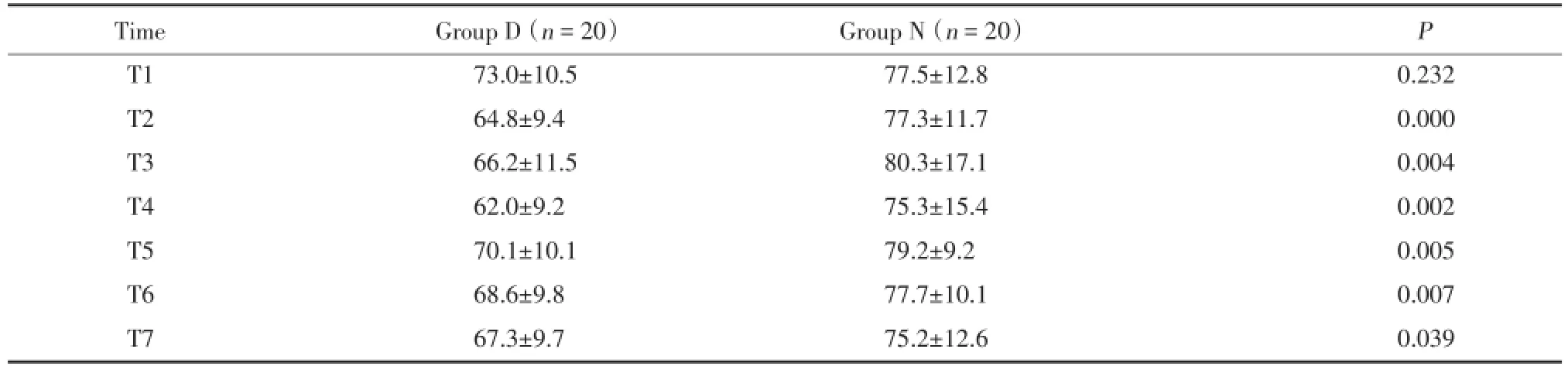
表2 2组患者各时间点心率Tab.2 The heat rates of the two groups at different time points
Time Group D(n=20) Group N(n=20) P T1 73.0±10.5 77.5±12.8 0.232 T2 64.8±9.4 77.3±11.7 0.000 T3 66.2±11.5 80.3±17.1 0.004 T4 62.0±9.2 75.3±15.4 0.002 T5 70.1±10.1 79.2±9.2 0.005 T6 68.6±9.8 77.7±10.1 0.007 T7 67.3±9.7 75.2±12.6 0.039
D组和N组患者相比,在各个时间点的平均动脉压差异均无统计学意义(P>0.05)。见表3。
2.42组患者各时间点的脑氧饱和度
2组患者在各个时间点的脑氧饱和度无统计学差异(P>0.05)。见表4。
2.52组患者术前术后的MMSE得分
表3 2组患者各时间点的平均动脉压Tab.3 The mean arterial pressure of the two groups at different time points
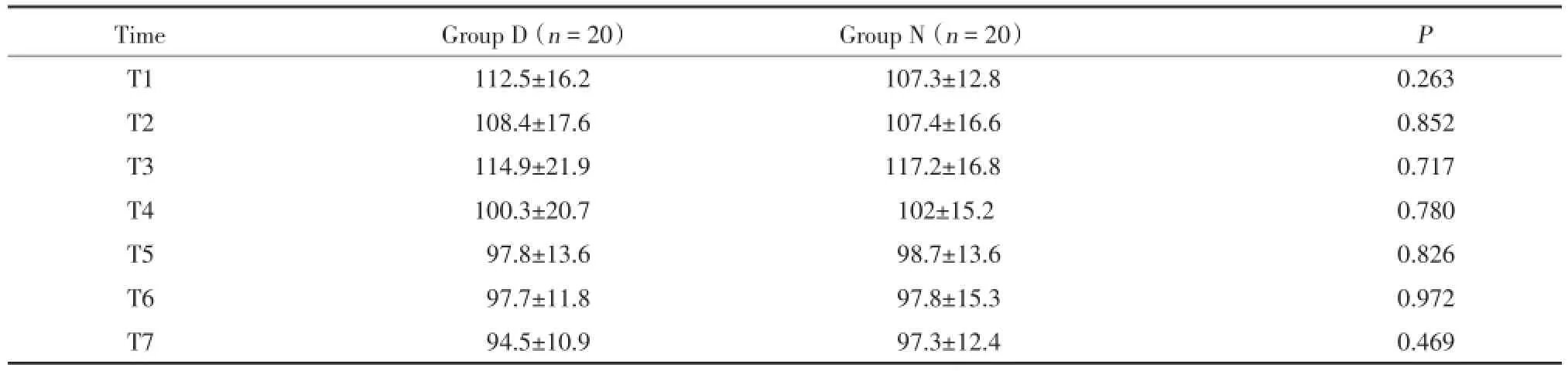
表3 2组患者各时间点的平均动脉压Tab.3 The mean arterial pressure of the two groups at different time points
Time Group D(n=20) Group N(n=20) P T1 112.5±16.2 107.3±12.8 0.263 T2 108.4±17.6 107.4±16.6 0.852 T3 114.9±21.9 117.2±16.8 0.717 T4 100.3±20.7 102±15.2 0.780 T5 97.8±13.6 98.7±13.6 0.826 T6 97.7±11.8 97.8±15.3 0.972 T7 94.5±10.9 97.3±12.4 0.469
表4 2组患者各时间点的脑氧饱和度Tab.4 The regional cerebral oxygen saturation of the two groups at different time points
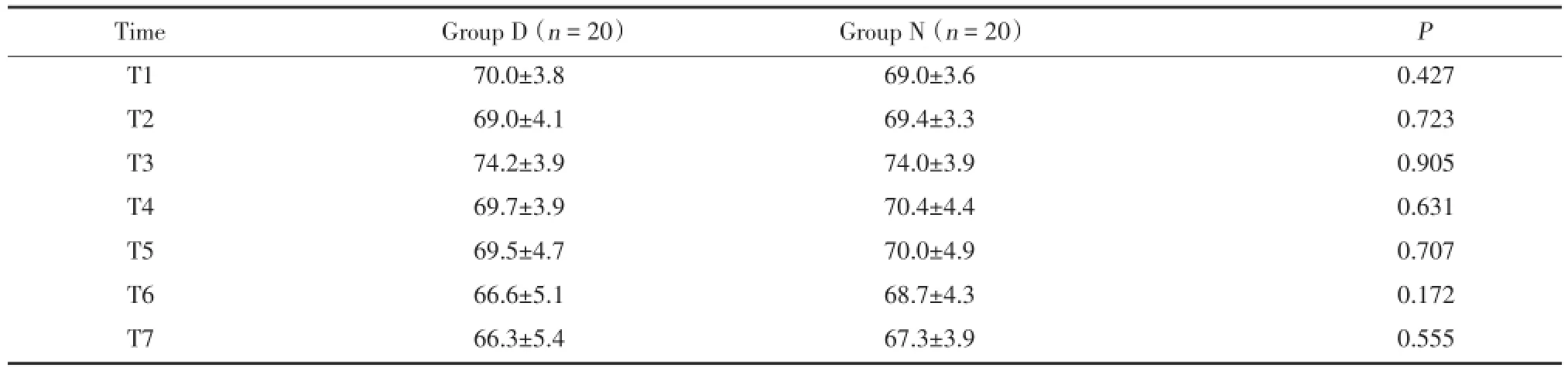
表4 2组患者各时间点的脑氧饱和度Tab.4 The regional cerebral oxygen saturation of the two groups at different time points
Time Group D(n=20) Group N(n=20) P T1 70.0±3.8 69.0±3.6 0.427 T2 69.0±4.1 69.4±3.3 0.723 T3 74.2±3.9 74.0±3.9 0.905 T4 69.7±3.9 70.4±4.4 0.631 T5 69.5±4.7 70.0±4.9 0.707 T6 66.6±5.1 68.7±4.3 0.172 T7 66.3±5.4 67.3±3.9 0.555
2组患者术前的MMSE评分无统计学差异(P>0.05),术后的MMSE评分较术前相比均有所下降(P<0.05)。D组术后的MMSE评分高于N组,差异有统计学意义(P<0.05)。见表5。
3 讨论
脑氧饱和度可反映脑氧代谢情况。吸入氧浓度、二氧化碳分压、血压、血红蛋白含量、体温、颅骨厚度、探头位置、皮肤色素等都可影响脑氧饱和度数值[11⁃12]。脑血供增加、吸入氧浓度增高或脑代谢抑制时,脑氧饱和度升高,反之则降低[1]。此测量方法基于朗伯-比尔定律[13⁃14]。脑氧饱和度监测简便无创,灵敏性和特异性高,能够体现脑区的氧供需平衡[1-2,15]。
表52 组患者术前术后的MMSE得分Tab.5 The preoperative and postoperative MMSE scores of the two groups

表52 组患者术前术后的MMSE得分Tab.5 The preoperative and postoperative MMSE scores of the two groups
Time Group D(n=20) Group N(n=20) P Preoperative 27.0±1.7 27.3±1.8 0.605 Postoperative 1 day 26.1±1.8 24.8±1.8 0.035
POCD可影响术后恢复情况[16],在接受腹部手术的老年患者中发生率可达38%[3],其发生可能与术中脑氧代谢有关[4]。SAMRA等[5]研究发现若脑氧饱和度值较基础值下降20%以上,可提示出现神经系统并发症。有研究[6]证实脑氧饱和度如在短期内下降至50%以下,认知功能的损害加剧。
右美托咪定是高选择性的α2肾上腺素能受体激动药,受体选择性(α2∶α1)为1 620∶1[8,17]。右美托咪定可产生镇静、镇痛、交感神经抑制等作用。有多项证据[9-10,18-21]表明,右美托咪定有神经保护作用,能改善患者术后认知功能。
本研究旨在探索右美托咪定是否能通过提高术中脑氧饱和度而改善择期行全麻下开腹手术的中老年患者术后认知功能。患者术后第1天的MMSE评分,D组高于N组,有统计学差异。这表明右美托咪定可改善患者术后认知功能。这与之前的报道一致。然而,2组患者各时间点的脑氧饱和度均无统计学差异。该药物对认知功能的改善,并不是通过提高术中脑氧饱和度来实现的。
右美托咪定改善认知功能的机制,可能涉及以下因素:(1)儿茶酚胺释放增加,可造成神经元的损伤和死亡[19]。右美托咪定减少儿茶酚胺释放,保护神经元。(2)α2受体的激活可减少谷氨酸释放,并增强神经元对谷氨酸的耐受[22]。(3)PI3K/Akt和ERK1/2通路对于细胞存活有关键作用[23]。ZHU等[24]研究发现,右美托咪定可能激活PI3K/Akt和ERK1/2通路,减少神经元凋亡。(4)脑源性神经营养因子(brain⁃derived neurotrophic factor,BDNF)具有神经保护作用[25]。有报道[26]认为右美托咪定可引起BDNF的表达上调。
右美托咪定通过激活神经系统的α2受体以及激活靶器官中的α2受体而产生降心率、降血压等心血管效应[17]。本研究给药后的各个时间点,D组患者心率明显低于N组。然而D组与M组各时刻血压无统计学差异。原因分析如下:本研究的麻醉深度调节主要根据患者血流动力学变化来进行。术中主要根据血压来调节七氟醚的浓度,维持合适的麻醉深度。因此,2组患者血压未出现明显差异。
综上所述,术前给予右美托咪定,可以改善择期行全麻下开腹手术的中老年患者术后认知功能,但不能影响患者的脑氧饱和度。右美托咪定改善术后认知功能的作用,不是通过提高术中脑氧饱和度来实现的。
[1]TRIPP LD,WARM JS,MATTHEWS G,et a1.On tracking the course of cerebral oxygen saturation and pilot performance during gravity⁃induced loss of consciousness[J].Hum Factors,2009,51(6):775-784.DOI:10.1177/0018720809359631.
[2]EDMONDS HL.Advances in neuromonitoring for cardiothoracic and vascular surgery[J].J Cardiothorac Vasc Anesth,2001,15(2):241-250.DOI:10.1053/jcan.2001.21992.
[3]曹建国,洪涛,闻大翔,等.老年患者术后精神和认知障碍的发病率及相关因素分析[J].上海医学,2005,28(11):939-941.DOI:10.3969/j.issn.0253⁃9934.2005.11.011.
[4]蔡一榕,薛张纲,朱彪,等.非心脏大手术老年患者术后认知功能障碍与术中脑氧代谢的关系[J].中华麻醉学杂志,2008,28(5):434-436.DOI:10.3321/j.issn:0254⁃1416.2008.05.020.
[5]SAMRA SK,DY EA,WELCH K,et al.Evaluation of a cerebral ox⁃imeter as a monitor of cerebral ischemia during carotid endarterecto⁃my[J].Anesthesiology,2000,93(4):964-970.DOI:10.1097/ 00000542⁃200010000⁃00015.
[6]YAO FS,TSENG CC,HO CY,et al.Cerebral oxygen desaturation is associated with early postoperative neuropsychological dysfunction in patients undergoing cardiac surgery[J].J Cardiothorac Vasc Anesth,2004,18(5):552-558.DOI:10.1053/j.jvca.2004.07.007.
[7]SCHOEN J,MEYERROSE J,PAARMANN H,et a1.Preoperative regional cerebral oxygen saturation is a predictor of postoperative delirium in on⁃pump cardiac surgery patients:a prospective observa⁃tional trial[J].Crit Care,2011,15(5):218.DOI:10.1186/ cc10454.
[8]HAYASHI Y,MAZE M.Alpha⁃2 adrenoceptor agonists and anaes⁃thesia[J].Br J Anaesth,1993,71(1):108-118.DOI:10.1093/bja/71.1.108.
[9]CHEN J,YAN J,HAN X.Dexmedetomidine may benefit cognitive function after laparoscopic cholecystectomy in elderly patients[J]. Exp Ther Med,2013,5(2):489-494.DOI:10.3892/etm.2012.811.
[10]柏平,闫东,税春玲.术中使用右美托咪啶对老年患者术后认知功能的影响[J].重庆医学,2013,42(18):2107-2109.DOI:10.3969/j.issn.1671⁃8348.2013.18.017.
[11]MADSEN PL,SECHER NH.Near⁃infrared oximetry of the brain[J].Prog Neurobiol,1999,58(6):541-560.DOI:10.1016/S0301⁃0082(98)00093⁃8.
[12]DAVIE SN,GROCOTT HP.Impact of extracranial contamination on regional cerebral oxygen saturation,a comparison of three cere⁃bral oximetry technologies[J].Anesthesiology,2012,116(4):834-840.DOI:10.1097/ALN.0b013e31824c00d7.
[13]杨玉星,彭涤芳,王左.一种新型的测量血样血氧饱和度的系统[J].中国医疗器械杂志,1991,15(6):331-333.
[14]TREMPER KK,BARKER SJ.Pulse oximetry[J].Anesthesiology,1989,70(1):98-108.
[15]MOERMAN A,VAN HERZEELE I,VANPETEGHEM C,et a1. Near⁃infrared spectroscopy for monitoring spinal cord ischemia during hybrid thoracoabdominal aortic aneurysm repair[J].J En⁃dovasc Ther,2011,18(1):91-95.DOI:10.1583/10⁃3224.1.
[16]RUNDSHAGEN I.Postoperative cognitive dysfunction[J].Dtsch Arztebl Int,2014,111(8):119-125.DOI:10.3238/arztebl.2014. 0119.
[17]KHAN ZP,FERGUSON CN,JONES RM.Alpha⁃2 and imidazoline receptor agonists.Their pharmacology and therapeutic role[J]. Anaesthesia,1999,54(2):146-165.DOI:10.1046/j.1365⁃2044. 1999.00659.
[18]COSAR M,ESER O,FIDAN H,et al.The neuroprotective effect of dexmedetomidine in the hippocampus of rabbits after subarachnoid hemorrhage[J].Surg Neruol,2009,71(1):54-59.DOI:10.1016/ j.surneu.2007.08.020.
[19]MA D,RAJAKUMARASWAMY N,MAZE M.Alpha2⁃adrenocep⁃tor agonists:shedding light on neuroprotection?[J].Br Med Bull,2005,71(1):77-92.DOI:10.1093/bmb/ldh036.
[20]ENGELHARD K,WERNER C,EBERSPÄCHER E,et al.The ef⁃fect of the alpha 2⁃agonist dexmedetomidine and the N⁃methyl⁃D⁃aspartate antagonist S(+)⁃ketamine on the expression of apoptosis⁃regulating proteins after incomplete cerebral ischemia and reperfu⁃sion in rats[J].Anesth Analg,2003,96(2):524-531.DOI:10.1097/00000539⁃200302000⁃00041.
[21]陈力,李传翔,宋伏虎,等.右美托咪定对老年人全髋置换术后早期认知功能障碍的影响[J].广东医学,2012,33(21):3321-3323.DOI:10.3969/j.issn.1001⁃9448.2012.21.052.
[22]MADISON DV,NICOLL RA.Actions of noradrenaline recorded in⁃tracellularly in rat hippocampal pyramidal neurons,in vitro[J].J Physiol,1986,372(1):221-244.DOI:10.1113/jphysiol.1986. sp016006.
[23]CANTLEY LC.The phosphoinositide 3⁃kinase pathway[J].Sci⁃ence,2002,296(5573):1655-1657.DOI:10.1126/science.296.55 73.1655.
[24]ZHU YM,WANG CC,CHEN L,et al.Both PI3K/Akt and ERK1/2 pathways participate in the protection by dexmedetomidine against transient focal cerebral ischemia/reperfusion injury in rats[J]. Brain Res,2013,1494(1):1-8.DOI:10.1016/j.brainres.2012.11. 047.
[25]DEGOS V,LORON G,MANTZ J,et al.Neuroprotective strategies for the neonatal brain[J].Anesth Analg,2008,106(6):1670-1680.DOI:10.1213/ane.0b013e3181733f6f.
[26]DEGOS V,CHARPENTIER TL,CHHOR V,et al.Neuroprotective effects of dexmedetomidine against glutamate agonist⁃induced neu⁃ronal cell death are related to increased astrocyte brain⁃derived neurotrophic factor expression[J].Anesthesiology,2013,118(5):1123-1132.DOI:10.1097/ALN.0b013e318286cf36.
(编辑于溪)
Effect of Dexmedetomidine on Postoperative Cognitive Function and Intraoperative Regional Cerebral Oxygen Saturation of Middle⁃aged and Elderly Patients Undergoing Open Surgery
HOU Daliang,WU Xiuying
(Department of Anesthesiology,Shengjing Hospital,China Medical University,Shenyang 110004,China)
ObjectiveTo investigate whether dexmedetomidine can improve the postoperative cognitive function of middle⁃aged and elderly pa⁃tients undergoing selective open surgery with general anesthesia via elevating intraoperative regional cerebral oxygen saturation.MethodsForty middle⁃aged and elderly patients that were scheduled for open surgery were recruited in the study and randomly assigned to two groups:patients in group D(n=20)
dexmedetomidine 0.5 μg/kg iv(concentration 4 μg/mL)injected at 10 minutes before the operation while those in group N(n=20)were injected with normal saline with the same quantity.ResultsThere was no significant difference of the heart rates of the pa⁃tients in two groups when they entered the operating room(P>0.05).The heart rates of the patients in group D decreased significantly compared with those in group N at all⁃time points after the administration of drugs(P<0.05).No significant difference in mean arterial pressure or regional cerebral oxygen saturation was observed at any time point(P>0.05).The patients in group D had higher MMSE scores than those in group N(P<0.05),with statistical significance.ConclusionPreoperative administration of dexmedetomidine improves postoperative cognitive function of mid⁃dle⁃aged and elderly patients undergoing selective open surgery with general anesthesia,which cannot affect the regional cerebral oxygen saturation of the patients.The effect of improving postoperative cognitive function of dexmedetomidine is not achieved by elevating intraoperative regional cere⁃bral oxygen saturation.
dexmedetomidine;middle⁃aged and elderly patients;open surgery;regional cerebral oxygen saturation;postoperative cog⁃nitive function
R614.2
A
0258-4646(2016)11-1039-04
10.12007/j.issn.0258⁃4646.2016.11.019
侯大亮(1989-),男,医师,硕士.
吴秀英,E-mail:wuxy@sj⁃hospital.org
2016-04-13
网络出版时间: