食管癌放射治疗计划的剂量学比较
2016-11-12熊绮丽倪千喜中国科学院上海应用物理研究所嘉定园区上海0800
熊绮丽 徐 刚 石 勇 倪千喜 顾 强(中国科学院上海应用物理研究所 嘉定园区 上海 0800)
2(上海大学 上海 200444)
3(中南大学湘雅医学院附属肿瘤医院 长沙 410013)
4(中南大学湘雅三医院 长沙 410013)
食管癌放射治疗计划的剂量学比较
熊绮丽1,2,3徐 刚2石 勇4倪千喜3顾 强1
1(中国科学院上海应用物理研究所 嘉定园区上海 201800)
2(上海大学上海 200444)
3(中南大学湘雅医学院附属肿瘤医院长沙 410013)
4(中南大学湘雅三医院长沙 410013)
比较食管癌患者应用螺旋断层(TomoHelical, TH)、径照断层(TomoDirect, TD)、容积旋转调强(Volumetric modulated arc therapy, VMAT)和固定野动态调强(Intensity modulated radiation therapy, IMRT) 4种放疗计划的剂量学差异。选取18例食管癌患者,利用Pinnacle9.2计划系统设计单弧360°VMAT放疗计划和5野IMRT放疗计划。利用TomoHDTM2.0.7计划系统设计TH放疗计划和5野TD放疗计划。利用剂量体积直方图(Dose volume histogram, DVH)统计靶区剂量参数、适形性指数(Conformity index, CI)和均匀性指数(Heterogeneity index, HI),肺、心脏、脊髓剂量体积参数,出束时间和治疗跳数。TH计划靶区适形性和靶区均匀性略优于TD计划,VMAT计划靶区适形性和靶区均匀性略优于IMRT计划,且前两种计划明显优于后两种;TH计划和VMAT计划肺V20Gy、V30Gy,心脏V30Gy、V40Gy分别优于TD计划和IMRT计划;但是TD计划肺V5Gy具有其他计划都不具有的优势。TH计划优于TD计划优于VMAT计划优于IMRT计划。但如果考虑性价比,本研究认为对于食管癌VMAT计划是首选;如果考虑放射治疗计划的质量,TH计划是首选;但如果靶区体积比较大,肺的低剂量无法达到临床要求时,可以考虑用TD计划解决这一难题。
食管癌,螺旋断层,径照断层,容积旋转调强,固定野动态调强,剂量学比较
CLCTL72
放射治疗是食管癌的主要治疗手段之一,但是由于病变区与脊髓、肺等重要器官紧邻,所以主要考虑静态调强放射治疗(Intensity modulated radiation therapy, IMRT)和容积旋转调强放射治疗(Volumetric modulated arc therapy, VMAT),有关两种计划剂量学比较的研究也颇多[1-3],总体来说,VMAT计划剂量分布优于IMRT计划,且能减少治疗跳数和降低危及器官的受量[4-6]。随着放疗技术的发展,螺旋断层放射治疗(Tomotherapy)成为目前最先进的光子放疗技术[7],尤其是第二代Tomotherapy机器的出现,它不仅能提供螺旋断层放射照射(TomoHelical, TH),即机架360°旋转的同时治疗床缓慢移动,而且能提供断层径照射(TomoDirect,TD),即机架仅固定在给定的 n个角度但治疗床缓慢进出 n次[8]。美国 MD Anderson 肿瘤中心的LANGEN 博士[9]对用螺旋断层方式和断层径照方式在乳腺癌短程放疗的计划对比研究中发现,在靶区的适形度上,螺旋断层的剂量分布要更好,但是断层径照在同侧肺的保护上明显超过螺旋断层方式。TH计划能给予更加精细的剂量分布,但是由于 360°旋转治疗造成食管癌,主要危及器官肺低剂量大体积,从而增加引起放射性肺炎的机率[10],第二代Tomotherapy独有的TD技术不仅同样能给予相对精细的剂量分布,而且能降低肺低剂量的体积,该结论已在乳腺癌上得到验证[11]。本研究通过比较TH、TD、VMAT和IMRT四种放射治疗计划的靶区剂量分布和危及器官受到的剂量来为食管癌的临床放射治疗的应用提供依据。
1 材料和方法
1.1一般资料
随机选取湖南省肿瘤医院2015年1~10月的18例食管放射治疗的食管癌患者,其中男性15例,女性3例;中位年龄62 (46~72)岁;根据UICC2002TNM分期,其中T3N1M0 8例、T3N2M0 5例、T2N1M0 1例、T3M0N0 3例、T4N0N0 1例;患者颈胸热塑体膜固定,仰卧位双臂上举抱头。在GE 型 CT 模拟定位机下进行自由平静呼吸螺旋和静脉增强扫描,层厚 5 mm,扫描上、中、下整段食管,获得CT图像传输至放射治疗计划系统进行三维重建。
1.2靶区和危及器官定义
由科室放疗医生根据ICRU50和62号文件应用Pinnacle9.2计划系统在CT影像上勾画出原发肿瘤区(Gross target volume, GTV);临床靶区(Clinical target volume, CTV)由GTV纵轴方向外扩3~5 cm,前后左右外扩0.5 cm(外放后根据解剖结构稍微调整),计划靶区(Planning target volume, PTV)由CTV外放0.5 cm得到。肺、脊髓和心脏为危及器官。
1.3放射治疗计划
临床处方剂量 DT要求:DPTV=60 Gy/30次,VDT≥95%,Dmax≤66 Gy,危及器官处方剂量要求:肺V5Gy≤60%~65%、V20Gy≤30%、V30Gy≤20%;心脏V30Gy≤40%、V40Gy≤30%;脊髓D1%≤45 Gy;按照临床处方剂量要求设计以下 4组计划:(1)TomoHDTM2.0.7计划系统,剂量率为863 MU/min,螺旋断层照射方式(TH);(2) TomoHDTM2.0.7计划系统,剂量率为863 MU/min,五野的断层径照方式(TD);(3) Pinnacle9.2计划系统,6MV-X线,最大剂量率为 600 MU/min,单弧逆时针容积旋转治疗(VMAT):起始角度179°,终止角度181°,准直器角度5°,治疗床角0°,每4°一个弧形野;(4)Pinnacle9.2计划系统,6MV-X线,剂量率为 600 MU/min,固定野调强放射治疗(IMRT),采取与TD计划相同角度的五野。
1.4评估方法
根据ICRU83[12]号报告,通过评估剂量体积直方图(Dose volume histogram, DVH)的以下参数来评估靶区剂量分布(Vx表示靶区或者危机器官受到不大于xGy剂量照射的体积,单位:%;Dx%表示靶区或者危机器官 x%的体积接受的吸收剂量,单位Gy;Dmean表示平均剂量):D50%、D95%、Dmean、V50以及适形性指数(Conformity index, CI)[13]和均匀性指数(Heterogeneity index, HI)[14]。
式中:VDT-PTV计划靶区中达到处方剂量的体积,VDT表示达到处方剂量的体积,VDT-PTV表示计划靶区的体积。
适形性指数CI值越接近1,说明计划适形度越高;HI值越接近0,说明计划的均匀度越高。
危及器官中评估肺 V5Gy、V10Gy、V20Gy、V30Gy和 Dmean;脊髓 D1%和 Dmean;心脏 V30Gy、V40Gy和Dmean;由于Tomotherapy是采用出束时间(min)来表示治疗效率,而普通加速器是采取治疗跳数(MU)来表示治疗跳数,所以只存在TH与TD比较,VMAT与IMRT比较。
1.5统计学分析
2 结果
2.1靶区剂量分布
四种计划的靶区剂量分布均能满足临床剂量要求。如表1和图1所示:靶区适形性指数CI、均匀性指数HI、VDT和D95%的TH、TD、VMAT和IMRT计划差异均具有统计学意义。四种计划的D95%相当,且差异均具有统计学意义。D50%是TH计划、TD计划和VMAT计划相当且优于IMRT计划,但差异不具有统计学意义。
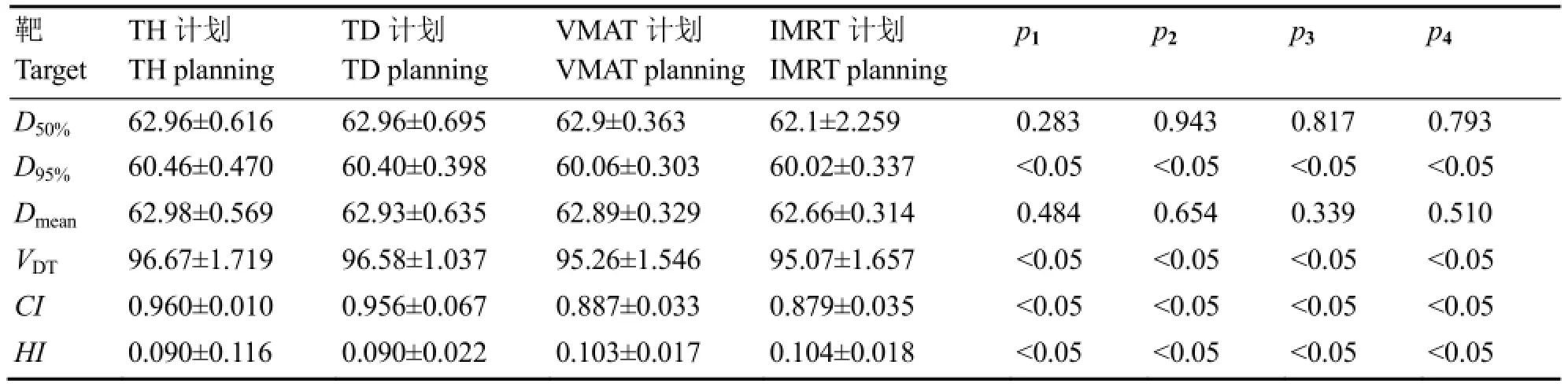
表1 四种放疗计划的靶区剂量学参数比较Table 1 Target dosimetric parameters among the four kind of radiation treatment planning (Gy or %)
2.2危及器官剂量分布
四种计划的肺、心脏和脊髓的剂量均能达到临床剂量要求。如表 2所示,肺 V5Gy、V10Gy、V20Gy和V30Gy的TH、TD、VMAT和IMRT计划差异均具有统计学意义;肺Dmean是TH和TD相当,但优于也相当的VMAT和IMRT,且除VMAT和IMRT比较差异不具有统计学意义外,其余均有。心脏V30Gy和V40Gy的TH、TD、VMAT和IMRT计划、差异均具有统计学意义;脊髓D1%的TH、TD、VMAT和IMRT计划差异均具有统计学意义。
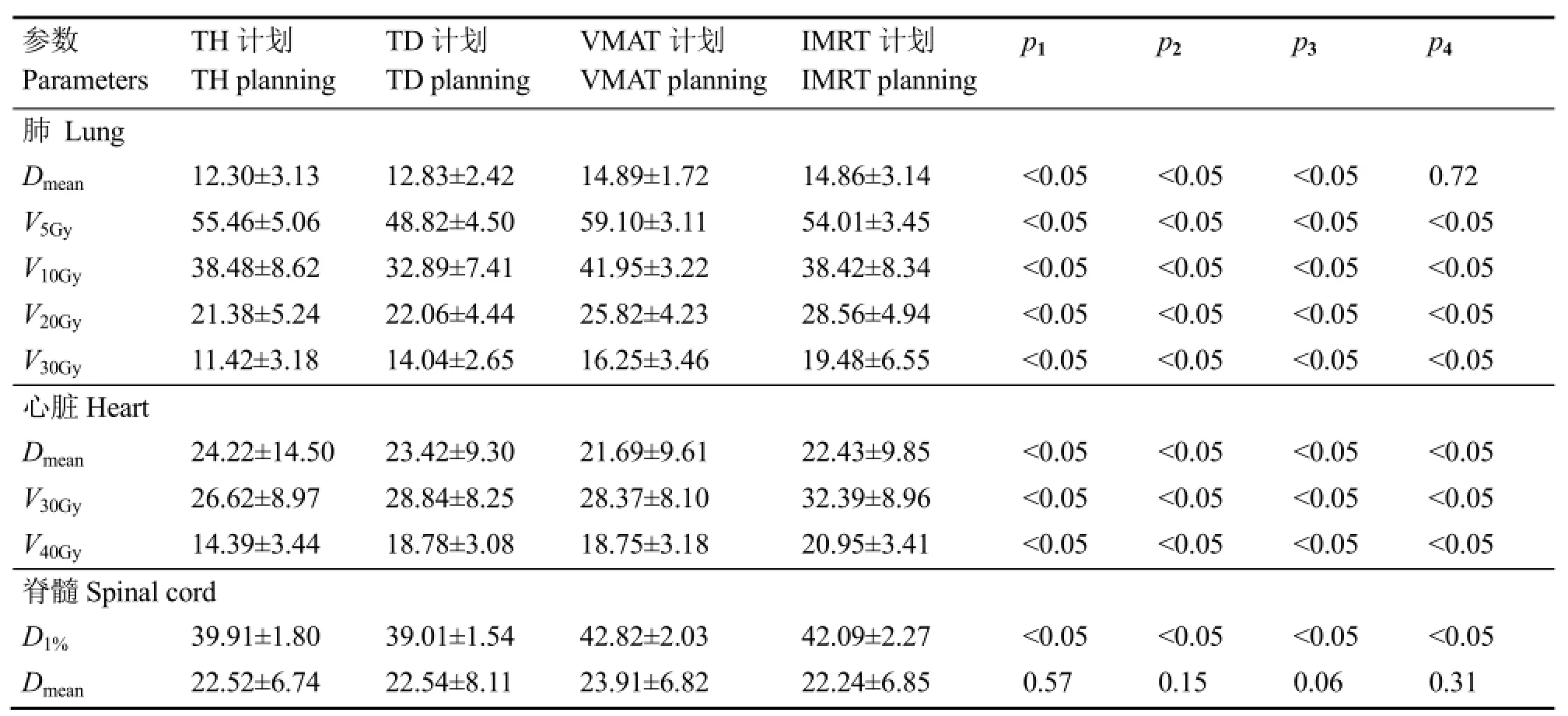
表2 四种计划的危及器官剂量学参数比较Table 2 Risking organ dosimetry parameters between the four kind of radiation treatment planning (Gy or %)
2.3出束时间或跳数
TH和TD计划的出束时间分别为(11.85±4.112)min和(6.780±1.424) min,VMAT和IMRT计划跳数分别为(459.33±59.93) MU 和(862±150.945)MU,且差异均具有统计学意义。
3 讨论
国内外关于食管癌放射治疗计划的剂量学比较颇多,但是多为VMAT、IMRT和3D-CRT之间的比较[15-16]。大量研究表明,VMAT与IMRT的计划相比,对于食管癌最大的优势在于显著降低治疗时间,减少跳数 MU,同时还能提高靶区适形性和均匀性,降低肺和心脏高剂量的体积[17-18],而肺V20Gy和 V30Gy均是临床放射性肺炎的重要指标[19],但是由于360°旋转照射治疗会增加肺低剂量即V5Gy的体积,而V5Gy也是临床认为引发放射性肺炎的重要指标[20];本研究中,VMAT和IMRT计划的比较得到了同样的结论,相对于IMRT计划,VMAT计划的治疗跳数减少46.8%,肺V20Gy和V30Gy均降低3%,心脏V30Gy和V40Gy分别降低4%和2%,但是肺V5Gy和V10Gy分别提高5%和3%,脊髓D1%两者相当。VMAT计划靶区适形性指数CI、均匀性指数HI、D50%、D95%、Dmean和VDT都有优势,但是优势并不明显。而Fu等[21]研究表明,当食管癌IMRT计划超过5个射野时,靶区的适形性并不会随着射野的增加而提高。食管癌中危及器官肺是大体积器官,处于整段食管的两侧,是食管癌中重要关注的器官,为了不引起放射性肺炎降低肺受到的剂量,往往是以牺牲靶区适形性和均匀性为代价的。
国内为有关Tomotherapy的TH计划、VMAT和IMRT计划比较的研究也有一些,主要是在肺癌、鼻咽癌和宫颈癌等[22-24]。但是由于TD技术是二代Tomotherapy机型独有,所以相关的研究很少。已有研究[11]比较乳腺癌TH和TD 计划,表明TD照射方式改善了危急器官的低剂量区受照体积,改善了出束时间,在减少危急器官低剂量区体积和更好的靶区剂量适形性与均匀性分布上是一个很好的选择。它给需要大范围的危急器官保护患者提供了一种治疗方式的选择;Mcintosh 等[25]在运用TD研究乳腺癌治疗上也得出同样或类似的结果,即对肺、心脏等关键器官的保护上,TD优势明显。本研究通过比较食管癌TH计划和TD计划剂量学差异发现, 与 TD计划相比, TH计划靶区适形性指数CI、均匀性指数HI、D50%、D95%、Dmean和VDT都略有优势,但是优势并不明显。TD计划的出束时间较TH计划减少了42.78%,大大提高了射线的利用率。肺V5Gy和V10Gy,TD计划比TH计划分别降低7%和6%,但是肺V20Gy和V30Gy分别增加1%和3%,心脏V30Gy和V40Gy分别增加2%和4%,脊髓D1%两者相当。由此可知,TD计划对于肺的低剂量体积确实有一定优势,而TH计划的优势体现在肺和心脏的高剂量体积。对于食管癌计划来讲,如果十分关注肺低剂量的体积但TH计划又不能满足临床要求的情况下,可以考虑使用TD计划,而且TD计划可以大量减少出束时间。但是如果TH计划的肺低剂量体积能满足临床要求,出束时间合适的情况下,优先考虑TH计划不仅能降低肺高剂量的体积降低放射性肺炎发生几率,而且能降低心脏受到的剂量提高患者的生存质量。
整体来讲,TH计划和 TD计划的靶区适形性CI、靶区均匀性 HI、VDT、肺 V20Gy、V30Gy、Dmean和脊髓D1%都要优于VMAT和IMRT计划; 四种计划的靶区D50%和Dmean是相当,没有明显的差异;心脏V30Gy和V40Gy均是TD计划VMAT计划相当,劣于TH计划但比优于IMRT计划;靶区剂量D95%是TH计划优于TD计划优于VMAT计划优于IMRT计划;肺V5Gy和V10Gy是TD计划优于IMRT计划优于TH计划优于VMAT计划。综上所述,食管癌的四种计划均能满足临床剂量要求,其中TH计划的质量最优,但对肺低剂量体系的保护上TD计划更具有优势。由于目前国内Tomotherapy机器新且少,加之很多省份还未纳入医保范围内,所以从实际临床工作和治疗费用来讲,无论是对于患者还是对于技术员,VMAT计划和IMRT计划的性价比更高,而这其中 VMAT计划对于提高患者的治疗效果和生存质量具有一定优势。所以如果考虑性价比,本研究认为对于食管癌VMAT计划是首选;如果考虑治疗效果和生存质量,TH计划是首选,但如果靶区体积比较大,肺的低剂量无法达到临床要求时,可以考虑用TD计划解决这一难题。
1Van Benthuysen L, Hales L, Podgorsak M. Volumetric modulated arc therapy vs. IMRT for the treatment of distal esophageal cancer[J]. Medical Dosimetry Official Journal of the American Association of Medical Dosimetrists,2011, 36(4): 404-409. DOI: 10.1016/j.meddos.2010.09. 009.
2刘晓静, 张西志, 李军, 等. 胸中段食管癌旋转容积调强与固定野动态调强放疗的剂量学研究[J]. 实用癌症杂志, 2011, 26(6): 630-633. DOI: 10.3969/j.issn.1001-5930.2011.06.025. LIU Xiaojing, ZHANG Xizhi, LI Jun, et al. Dosimetric comparison between rapidarc and fixed gantry dynamic IMRT for middle esophageal carcinoma[J]. The Practical Journal of Cancer, 2011, 26(6): 630-633. DOI: 10.3969/j.issn.1001-5930.2011.06.025.
3Nicolini G, Ghosh-Laskar S. Shrivastava S K. et al. Volumetric modulated arc therapy with flattening filter-free beams compared with static gantry IMRT and 3D conformal radiotherapy for advanced esophageal cancer: a feasibility study[J]. International Journal of Radiation Oncology Biology Physics, 2012, 84(2):553-560. DOI: 10.1016/j.ijrobp.2011. 12.041.
4Otto K. Volumetric modulated arc therapy: IMRT in a single gantry arc[J]. Medical Physics, 2008, 35(1):310-317. DOI: 10.1118/1.2818738.
5Abbas A S, Moseley D, Kassam Z, et al. Volumetricmodulated arc therapy for the treatment of a large planning target volume in thoracic esophageal cancer[J]. Journal of Applied Clinical Medical Physics, 2013, 14(3):1269. DOI: 10.1120/ jacmp.v14i3.4269.
6Hawkins M A, Bedford J L, Warrington A P, et al. Volumetric modulated arc therapy planning for distal oesophageal malignancies[J]. British Journal of Radiology,2012, 85(1009): 44-52. DOI: 10.1259/bjr/25428720.
7马林. 螺旋断层放疗系统的临床应用[J]. 中国医疗设备, 2014(10): 12-14. DOI: 10.3969/j.issn.1674-1633.2014. 10.004. MA Lin. Clinical Application of Tomotherapy System[J]. China medical devices, 2014(10): 12-14. DOI: 10.3969/j. issn.1674- 1633.2014.10.004.
8Franco P, Catuzzo P, Cante D, et al. TomoDirect: an efficient means to deliver radiation at static angles with tomotherapy[J]. Tumori, 2011, 97(4): 498-502. DOI: 10. 1700/950.10404.
9Langen K M, Buchholz D J, Burch D R, et al. Investigation of accelerated partial breast patient alignment and treatment with helical tomotherapy unit[J]. International Journal of Radiation Oncology biology physics, 2008, 70(4): 1272-1280. DOI: 10.1016/j.ijrobp. 2007.11.019.
10 Murai T, Shibamoto Y, Manabe Y, et al. Intensitymodulated radiation therapy using static ports of tomotherapy (TomoDirect): comparison with the TomoHelical mode[J]. Radiation Oncology, 2013, 8(1): 100-112. DOI:10.1186/1748-717X-8-201.
11 Borca V C, Franco P, Catuzzo P, et al. Does TomoDirect 3DCRT represent a suitable option for post-operative whole breast irradiation? A hypothesis-generating pilot study[J]. Radiation Oncology, 2012, 7(1): 1-10. DOI: 10. 1186/1748-717X-7-211.
12 International Commission on Radiation Units and Measurements (ICRU)(2010). Prescribing, recording, and reporting photon beam intensity-modulated radiation therapy (IMRT)[J] . Journal of the ICRU, 2012, 10(1):26-29. DOI: 10. 1093/jicru/ndq002.
13 Vivekanandan N, Sriram P, Kumar S A, et al. Volumetric modulated arc radiotherapy for esophageal cancer[J]. Medical Dosimetry Official Journal of the American Association of Medical Dosimetrists, 2012, 37(1): 108-113. DOI: 10.1016/j.meddos. 2011.01.008.
14 Yin Y, Chen J, Xing L, et al. Applications of IMAT in cervical esophageal cancer radiotherapy: a comparison with fixed field IMRT in dosimetry and implementation[J]. Journal of Applied Clinical Medical Physics, 2011, 12(2):48-57. PMID: 21587177.
15 张瑞, 习勉, 李巧巧, 等. 胸上段食管癌容积旋转调强和静态调强与三维适形放疗计划的剂量学比较[J]. 中山大学学报(医学科学版), 2012, 33(2): 260-264. DOI: 10. 13471/j.cnki.j.sun.yat-sen.univ(med.sci).2012.0046. ZHANG Rui, XI Mian, LI Qiaoqiao, et al. Volumetric modulated arc therapy, conventional intensity-modulated radiotherapy and three-dimensional conformal techniques for upper thoracic esophageal cancer: a planning comparison study[J]. Journal of Sun Yat-sen University(Medical Sciences), 2012, 33(2): 260-264. DOI: 10. 13471/j.cnki.j.sun.yat-sen.univ (med. sci). 2012.0046.
16 陈进琥, 尹勇, 刘同海, 等. 颈段食管癌固定野调强与旋转调强放疗计划比较研究[J]. 中华放射肿瘤学杂志,2010, 19(5): 429-435. DOI: 10.3760/cma.j.issn.1004-4221. 2010.05.013. CHEN Jinhu, YI Yong, LIU Tonghai, et al. Application of IMAT versus fixed-gantry IMRT in cervical esophageal cancer : a comparison in dosimetry and implementation[J]. Chinese Journal of Radiation Oncology, 2010, 19(5): 429 -435. DOI: 10.3760/cma.j.issn.1004-4221.2010.05.013.
17 陈婷婷, 张西志, 花威, 等. 容积旋转调强与固定野动态调强在上段食管癌治疗中的剂量学比较[J]. 临床肿瘤学杂志, 2013, 18(2): 151-154. DOI: 10.3969/j.issn. 1009-0460.2013.02.014. CHEN Tingting, ZHANG Xizhi, HUA Wei, et al. Dosimetric comparison between rapid arc and fixed gantry dynamic IMRT for upper esophageal cancer[J]. Chinese Clinical Oncology, 2013, 18(2): 151-154. DOI:10.3969/j.issn.1009-0460.2013.02.014.
18 Palma D, Vollans E, James K, et al. Volumetric modulated arc therapy for delivery of prostate radiotherapy:comparison with intensity-modulated radiotherapy and three-dimensionalconformalradiotherapy[J]. International Journal of Radiation Oncology Biology Physics, 2008, 72(4): 996-1001. DOI: 10.1016/j.ijrobp. 2008.02.047.
19 Marks L B, Yorke E D, Jackson A, et al. Use of normal tissue complication probability models in the clinic[J]. International Journal of Radiation Oncology Biology Physics, 2010, 76(3): 10-19. DOI: 10. 1016/j.ijrobp.2009. 07.1754.
20 Mayo C S, Urie M M. Fitzgerald T J, et al. Hybrid IMRT for treatment of cancers of the lung and esophagus[J]. International Journal of Radiation Oncology Biology Physics, 2008, 71(5): 1408-1418. DOI: 10.1016/j.ijrobp. 2007.12.008.
21 Fu W H, Wang L H, Zhou Z M, et al. Comparison of conformal and intensity-modulated techniques for simultaneous integrated boost radiotherapy of upper esophagealcarcinoma[J].WorldJournalof Gastroenterology, 2004, 10(8): 1098-1102. PMID:15069706 PMCID: PMC4656341.
22 Cattaneo G M, Delloca I, Broggi S, et al. Treatment planning comparison between conformal radiotherapy and helical tomotherapy in the case of locally advanced-stage NSCLC[J]. Radiotherapy and Oncology, 2008, 88(5):310-318. DOI: 10.1016/j.radonc.2008.06.006.
23 刘清智, 蒋华勇, 许卫东, 等. 胸膜间皮瘤螺旋断层调强放疗和容积旋转调强放疗的剂量学评估[J]. 中国医学物理学杂志, 2015, 32(5): 690-693. DOI: 10.3969/j.issn. 1005-202X.2015.05.017. LIU Qingzhi, JIANG Huayong, XU Weidong, et al. Dosimetric evaluation of helical tomotherapy and volumetric-modulatedarctherapyforpleural mesothelioma[J]. Chinese Journal of Medical Physics,2015, 32(5): 690-693. DOI: 10.3969/j.issn.1005-202X. 2015.05.017.
24 Murthy V, Master Z, Gupta T, et al. Helical tomotherapy for head and neck squamous cell carcinoma: dosimetric comparison with linear accelerator-based step-and-shoot IMRT[J]. Journal of Cancer Research and Therapeutics,2012, 6(2): 194-198. DOI: 10.4103/0973-1482.65245.
25 Mcintosh A, Read P W, Khandelwal S R, et al. Evaluation of coplanar partial left breast irradiation using tomotherapy-based topotherapy[J]. International Journal of Radiation Oncology Biology Physics, 2008, 71(2): 603-610. DOI: 10.1016/j.ijrobp.2008.01.047.
Dosimetric comparing four kinds of radiation treatment planning for esophagus cancer
XIONG Qili1,2,3XU Gang2SHI Yong4NI Qianxi3GU Qiang1
1(Shanghai Institute of Applied Physics, Chinese Academy of Sciences, Jiading Campus, Shanghai 201800, China)
2(Environmental and Chemical Engineering, Shanghai University, Shanghai 200444, China)
3(The Affiliated Cancer Hospital of Xiangya School of Central South University, Changsha 410013, China)
4(The Third Xiangya Hospital of Central South University, Changsha 410013, China)
Dose differences among TomoHelical (TH), TomoDirect (TD), Volumetric modulated arc therapy(VMAT) and intensity modulated radiation therapy (IMRT) for esophagus cancer were compared. Eighteen esophageal patients were chosen. The Pinnacle 9.2 treatment planning system was used to generate the VMAT plan and the five field IMRT plan. For comparison, the TH plan and five field TD plan were generated by TomoHDTM2.0.7 treatment planning system. It was available to adopt the dose volume histograms to investigate the dose parameters of target, the statistics of conformity index (CI), the heterogeneity index (HI) of planning target volume(PTV), the dose volumetric parameters of lung, and the spinal cord and heart, total accelerator output monitor units and total treatment time. The results showed that the CI and HI of TH plan was better than TD plan, and VMAT plan was better than IMRT plans, and the first two plans were better than the latter two; the lung's V20Gyand V30Gy, heart's V30Gyand V40Gyof TH plan and VMAT plan were better than those of TD plan and IMRT plan. However, the lung's V5Gyof TD plan had a greater advantage among them. The TH plan was better than TD plan, TD plan was better than VMAT plan, VMAT plan was better than IMRT plan. Taken the cost into consideration, the esophageal VMAT plan is preferred, and considering the therapeutic effect and quality of survival, the TH plan is preferred. When the target volume is relatively large, the low-dose lung is unavailable to achieve the clinical requirements. Therefore it is proposed to use the TD plans to cure the patients. Dose volume histograms are adopted for the statistics of CI, HI of PTV, dose volumetric parameters of lung, spinal cord and heart, total accelerator output monitor units and total treatment time.
Esophagus cancer, TomoHelical, TomoDirect, Volumetric modulated arc therapy, Intensity modulated radiation therapy, Dosimetric comparison
XIONG Qili (female) was born in September 1991 and graduated with a master degree from Shanghai University in 2016. E-mail: xiongqili@sinap.ac.cn
Ph.D. GU Qiang, professor, E-mail: guqiang@sinap.ac.cn
17 June 2016; accepted 29 August 2016
TL72
10.11889/j.1000-3436.2016.rrj.34.050201
国家自然科学基金(No.11175112)资助
熊绮丽,女,1991年9月出生,2016年于上海大学获得硕士学位,E-mail: xiongqili@sinap.ac.cn
顾强,博士,研究员,E-mail: guqiang@sinap.ac.cn
初稿2016-06-17;修回2016-08-29
Supported by the National Natural Science Foundation (No.11175112)
